


Heloísa Del Castanhel Ubaldo1; Marcos Noronha Frey1; Gerson Dellatorre2
Received on: 19/12/2018
Approved on: 10/04/2019
Study conducted at Dermatology Service, Hospital Santa Casa de Curitiba - Curitiba (PR), Brazil.
Financial support: None.
Conflito de Interesses: None.
Lip reconstruction after tumor excision is challenging because the results must be functional and cosmetic. In this context, Mohs micrographic surgery (MMS) is essential in ensuring maximum tissue preservation, with lower recurrence rates and the possibility of less complicated reconstructions.We report three cases of lip tumors treated with Mohs surgery, whose reconstruction was performed with island advancement flaps (V-Y).The relevance of the correct management of this type of tumor is discussed,highlighting the use of Mohs surgery and V-Y advancement flap,which provide satisfactory aesthetic and functional results.
Keywords: Lip neoplasms; Mohs surgery; Surgical flaps
Lip reconstruction of surgical defects affecting the skin and the vermilion border is challenging considering the impact that may be caused by unfavorable cosmetic and functional results.1,2,3 The control of surgical margins, obtained through Mohs micrographic surgery (MMS), helps to achieve better results, providing maximum tissue preservation combined with lower recurrence rates and the possibility of less complicated surgical reconstructions.1,3
We report three cases of malignant lip neoplasms, whose surgical treatment was performed with MMS and reconstruction used an island advancement flap (V-Y).
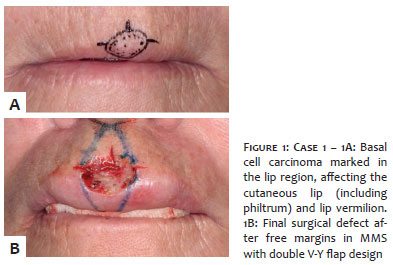
Case 1: Woman with nodular basal cell carcinoma (BCC) in the center of the upper lip, 0.5cm in diameter, involving the philtrum and the vermilion border (Figure 1A). The repair was performed by anatomical subunits with double V-Y advancement flap (Figures 1B and 2A). The three-month clinical follow-up demonstrates the maintenance of anatomical and functional characteristics (Figure 2B).
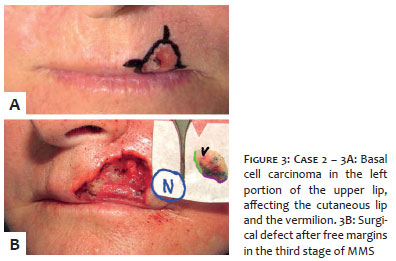
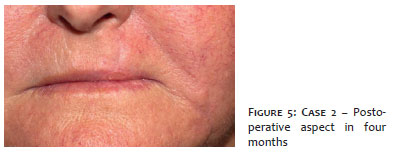
Case 2: Woman with nodular and ulcerated BCC in the left portion of the upper lip, 0.8 cm in its largest length, affecting the philtrum and the vermilion border (Figure 3A). After free margins in the second stage of the MMS (Figure 3B), the repair was performed with a skin-mucosa double opposing V-Y advancement flap (Figure 4). The four-month clinical follow-up (Figure 5) demonstrates the preservation of anatomical and functional characteristics.
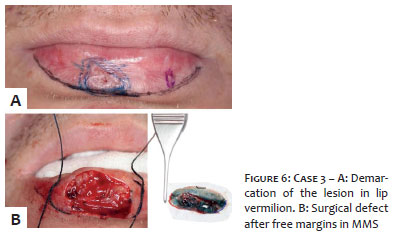
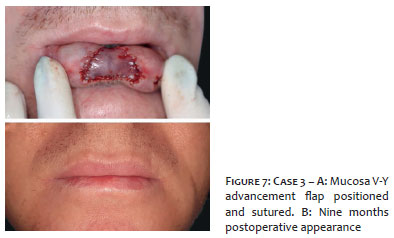
Case 3: Man with well-differentiated invasive squamous cell carcinoma (SCC) in the central region of the lower lip, with a diameter of 1cm and exclusive involvement of the vermilion border (Figure 6A). After MMS (Figure 6B), the repair was performed with a V-Y advancement flap of the lip mucosa (Figure 7A). The nine-month clinical follow-up (Figure 7B) showed satisfactory cosmetic and functional results.
The reconstruction of surgical defects involving the lip region, especially those including the vermilion, is technically complex.4,5 Due to the region's limited reserve tissue, there is a potential distortion of facial symmetry and losses in speech, eating, and facial expression functions,1,3,4 what should be considered by the surgeon when planning this type of intervention.
Using MMS in these cases plays an important role. The surgical margin control provided by the technique minimizes the sacrifice of healthy tissues adjacent to the tumor and allows more tissue to be made available for reconstruction.3 MMS also guarantees excellent long-term cure rates,3 preventing re-approaches in this critical area.
There are some closure options for surgical defects of the lip region. Primary linear closure may be considered when the operative wound is especially small or in the case of the philtrum when it is less than half of its width.3,4 Rotation flaps also include small surgical wounds due to potential anatomical changes in this limited area.3 Full-thickness skin grafts can be used and are suitable for treating large defects, with better results when positioned to occupy a whole cosmetic subunit.3 Even secondary wound closure may be considered in the concave area of the philtrum; however, the scar contraction of large wounds in this area may evolve with eclabium.3 As, in general, the surgical defects usually have an intermediate size between the ones mentioned in our study, the correction through these techniques can result in microstomy, vermilion reduction and potential alteration of the natural lip contour.4
The V-Y advancement flap is an excellent option for treating surgical lip defects as it recruits tissues of very similar texture, thickness, color, and even photodamage,2,4 also maintaining the pattern of facial cosmetic subunits. Notably, the possibility of correcting upper lip defects involving the philtrum, considered even more complicated due to the Cupid's bow contour characteristics,6 evidences the applicability of this technique, as observed in the first case. We also highlight the maintenance of the aesthetically relevant lip contour observed in the three cases.
In case 1, the area to be corrected included the central portion of the upper lip and also the philtrum; two island advancement flaps were performed perpendicular to the lip edge - one containing skin and the other containing mucosa. In case 2, the defect in the left portion of the upper lip also included skin and mucosa; its correction required two V-Y advancement flaps: the first, cutaneous, lateral to the lip; the second, a labial mucosa, which was projected perpendicularly and upwards to maintain the anatomical line of the vermilion border. In case 3, in which only the vermilion was affected, a single mucosal advancement was performed. In all cases, clinical follow-up showed satisfactory cosmetic and functional results.
The V-Y advancement flap should be remembered when planning surgical repairs that affect the labial region, highlighting the importance of its association with the MMS, which provides safety for margin control, in addition to satisfactory aesthetic and functional results.
Heloísa Del Castanhel Ubaldo | ORCID 000-0001-5828-4948
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Marcos Noronha Frey | ORCID 0000-0003-3914-2586
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases.
Gerson Dellatorre | ORCID
0000-0002-9657-0002
Approval of the final version of the manuscript; study design and planning; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Huilgol SC, Ma JHY, Hills RJ. Double island pedicle or V-Y flap repair for partial-thickness combined defects of the cutaneous and mucosal lip. J Am Acad Dermatol. 2014;71(6):1198-203.
2. Griffin GR, Weber S, Baker SR. Outcomes following V-Y advancement flap reconstruction of large upper lip defects. Arch Facial Plast Surg. 2012;14(3):193-7.
3. Kaufman AJ, Grekin RC. Repair of central upper lip (philtral) surgical defects with island pedicle flaps. Dermatol Surg. 1996;22(12):1003-7.
4. Zeitouni NC, Ang JM, Weyer CW, Krunic AL. Horizontally Opposed V-Y Advancement Flaps for Surgical Reconstruction of Central Upper Lip Defects. J Craniofac Surg. 2017;28(2):578-9.
5. Pepper JP, Baker SR. Local flaps: Cheek and lip reconstruction. JAMA Facial Plast Surg. 2013;15(5):374-82.
6. Paniker PU, Mellette JR. A simple technique for repair of Cupid's bow. Dermatol Surg. 2003; 29(6):636-40.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}