


Maria Claudia Almeida Issa1; Diego Cerqueira Alexandre2; Aline Cairo Fassini1; Camila de Oliveira Bento1; Flávio Barbosa Luz1; Enoí Aparecida Guedes Vilar1
Received on: 10/01/2019
Approved on: 14/04/2019
Study conducted at Universidade Federal Fluminense – Niterói (RJ), Brazil.
Financial support: None
Conflict of interests: None
Nevus lipomatosus cutaneous superficialis is an uncommon dermatosis in which the adipose tissue is present ectopically in the dermis.This condition is clinically divided into two variants: classical and solitary.The first is characterized by soft, pedunculated, cerebriform, skin-colored or yellowish papules or nodules, mainly involving the pelvic region.The latter is observed as a solitary or sessile papule. Treatment with surgical excision is usually enough. Nevus lipomatosus cutaneous superficialis may be associated with other conditions such as multiple lipomas, as in our case.
Keywords: Nevus; Dermis;Adipocytes; Lipoma
Nevus lipomatosus cutaneous superficialis (NLCS) is a rare and benign hamartomatous condition characterized by the presence of mature dermal adipocytes. NLCS is usually found at birth or arises within the first two decades of life. There are no reports of gender predilection or genetic predisposition. Clinically, it is classified into two variants. Asymptomatic clusters of soft, pedunculated, cerebriform, skin-colored or yellowish papules or nodules characterize the classical type. Lesions may coalesce into smooth, wrinkled, or peau d’orange textured plaques. This form is usually found in the pelvic girdle, especially in the gluteal, lumbosacral, and upper third of the thighs. The solitary type of NLCS manifests as a solitary or sessile papule. This form usually develops during adulthood and has been described in different locations: lower trunk, knee, armpit, arm, ear, and scalp. NLCS is treated with simple surgical excision. Because the condition is benign, it is removed for aesthetic reasons.1-7
Some lesions, such as angiokeratoma of Fordyce, café-au-lait or vitiligo-like macules, hemangioma, basal cell carcinoma (BCC), nevoid hypertrichosis, comedone-like lesions, and lipoma were described concomitantly with the NLCS.2-6 The rarity of the association of NLCS with lipomas in the literature and the exuberance in the presentation of our patient motivated us to publish it.
NLCS is characterized by the presence of ectopic mature dermal adipocytes. Clusters of soft, yellowish or skin-colored nodules, or papules that do not cross the midline and may follow Blaschko’s lines characterize the classical type, described by Hoffmann and Zurhelle in 1921. They may already be present at birth or, more commonly, appear by the second decade of life. The most frequent locations are the pelvic girdle, lumbosacral region, buttocks and thighs.2,3,4,8
The solitary type, described by Nikolowsky in 1950, consists of a single nodular lesion with later onset, usually occurring after the third decade of life.9 Its location varies greatly, with lesions on the lower trunk, clitoris, knee, armpit, arm, ear and scalp being described. This type is also referred to as a pedunculated lipofibroma. There are no reports of family history or gender preference in any of the clinical variants.10-12
In some cases, NLCS has been described to occur concurrently with some lesions such as angiokeratoma of Fordyce, café-au-lait or vitiligo-like macules, hemangioma, basal cell carcinoma (BCC), nevoid hypertrichosis, and comedone-like lesions.2-5 However, only one Spanish study has reported the association of nevus lipomatosus with lipomas. In this study, a female patient presented, at the age of 34, the onset of soft nodules in the popliteal fossa, the central lesion corresponding to nevus lipomatosus and the peripheral lesions corresponding to lipomas.13
Histologically, nevus lipomatosus cutaneous superficialis is characterized by the accumulation of ectopic mature dermal adipocytes. When they are scarce, they present perivascular distribution with lymphomonocytic infiltrate. When they are abundant, this relationship is not so clear, and the boundary between dermis and hypodermis becomes blurred. Dermal collagen fibers are unchanged and may be disorganized, or with increased density. Elastic fibers may be normal, increased, reduced or even absent. An increase in mucin has also been reported in the papillary and subpapillary dermis. The epidermis is normal or presenting acanthosis and may contain comedonian structures.13,14 Skin appendages are not replaced. However, some cases of NCLS with hairy abnormalities have been described, such as abortive germinal follicular-like structures, hypertrophic pilosebaceous units, perifollicular fibrosis, fibrofolliculomas, and folliculosebaceous cystic hamartoma.8
The pathogenesis of NLCS is not yet determined. Some authors have suggested that it originates from adipocyte precursor cells located around blood vessels.15 However, in a study with electron microscopy, only mature lipocytes were observed inside the perivascular mononuclear infiltrates, and no lipoblasts or the transition from mesenchymal cells to lipocytes were observed.16
The treatment of choice is surgical resection, which is instituted for aesthetic purposes only, given the benignity of the lesion and the possibility of increasing its size. Malignant degeneration and recurrences are extremely rare.1-7
A 33-year-old man presented with four asymptomatic nodular lesions, distributed in the trunk and limbs for two years, and with one asymptomatic pedunculated tumoral lesion, located in the upper third of the right posterior thigh. The latter had progressive growth, becoming unsightly. He had no family history of similar changes.
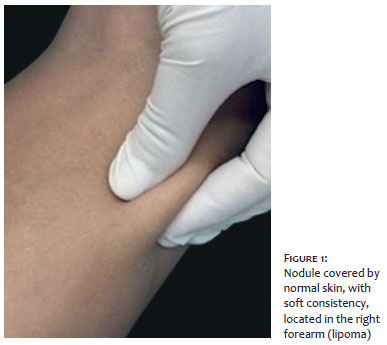
Dermatological examination revealed four nodules covered by normal skin, with a soft consistency, measuring 2-6cm in the largest diameter, located in the lumbar region to the left, in the right and left forearms, and in the anterior aspect of the right thigh (Figure 1). It also revealed a skin-colored, lobulated, pedunculated tumoral lesion with fibrous consistency measuring 6.5cm in length and 3cm in diameter, located below the right infragluteal sulcus (Figure 2). Clinically, we hypothesized lipomas for nodular lesions in the trunk and limbs, and solitary type of nevus lipomatosus cutaneous superficialis for the pedunculated lesion located below the right infragluteal sulcus. The pedunculated lesion and the nodules, except the one located on the left forearm (2cm), were surgically removed and confirmed by histopathological examination (Figure 3).
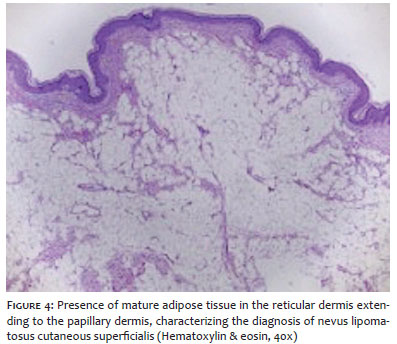
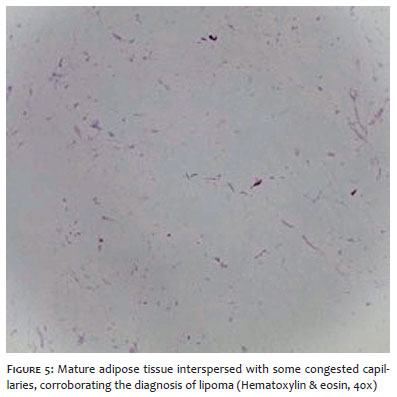
Histopathological examination of the exuberant pedunculated lesion revealed the presence of mature adipose tissue in the reticular dermis extending to the papillary dermis, characterizing the diagnosis of nevus lipomatosus cutaneous superficialis (Figure 4). Histopathological examinations of trunk and limb nodules showed similar characteristics among them, revealing mature adipose tissue interspersed with some congested capillaries, compatible with lipoma (Figure 5).
Nevus lipomatosus cutaneous superficialis (NLCS) may be present from birth or may appear after the third decade of life. When present from birth - the classical type - it is typically located in the pelvic region and lower limbs. In its solitary type, which begins after the third decade of life, it appears as a single and pedunculated lesion and has a very diverse location. In the case reported here, the patient presented the solitary type of the nevus lipomatosus cutaneous superficialis; however, it was located in the common area of the classical type. In agreement with the literature, the patient had no family history.1-7 There are some reports in the literature showing the association of NLCS with other dermatological changes, such as angiokeratoma of Fordyce, café-au-lait or vitiligo-like macules, hemangioma, basal cell carcinoma (BCC), nevoid hypertrichosis, and comedone-like lesions.2-5 However, little is known about the concomitance of this type of nevus with lipomas. To date, only one case has been reported demonstrating this association.13 Our report is similar to the case previously described, but it differs in the location of the lesions. Our patient’s lipomas and nevus lipomatosus were in distant sites of the body.
Despite its benign character, many patients wish to remove the lesion. In our case, the patient sought the Dermatology Service of the Universidade Federal Fluminense for the surgical removal of a lesion with an unusual and exuberant presentation. The aesthetic result after surgery was considered very good by the doctors and the patient (Figure 3A).
Diagnosis of nevus lipomatosus cutaneous superficialis may be difficult due to its rarity and different presentation forms. There are some reports of associations of NLCS to other dermatological changes. However, concomitance with lipomas was described only in a previous case. We report this case because of its peculiarity and exuberance as well as its association with multiple lipomas.
Maria Claudia Almeida Issa | ORCID 0000-0003-1031-7370
Clinical follow-up of the patient; supervision, orientation, and revision of the manuscript
Diego Cerqueira Alexandre | ORCID 0000-0001-9078-5566
Manuscript planning.
Aline Cairo Fassini | ORCID 0000-0002-9523-9342
Clinical follow-up and manuscript structuring.
Camila de Oliveira Bento | ORCID 0000-0002-4607-1432
Clinical follow-up and manuscript structuring.
Flávio Barbosa Luz | ORCID 0000-0001-5454-8950
Surgical follow-up of the patient; supervision, orientation, and revision of the manuscript
Enoí Aparecida Guedes Vilar | ORCID 0000-0001-8069-2104
Histopathological analysis of the findings.
1. Hoffmann EG, Zurhelle E. Uber einen. Naevus lipomatodes cutaneous superficialis der linken glutaalgegend. Arch Derm Syph 1921;130:327-33
2. Dhamija A, Meherda A, D'Souza P, Meena RS. Nevus lipomatosus cutaneous superficialis: An unusual presentation. Indian Dermatol Online J. 2012; 3(3):196-8.
3. Goyal M, Wankhade VH, Mukhi JI, Singh RP. Nevus lipomatosus cutaneous superficialis - a rare hamartoma: report of two cases. J Clin Diagn Res. 2016;10(10): WD01-2.
4. Das D, Das A, Bandyopadhyay D, Kumar D. Huge nevus lipomatosus cutaneous superficialis on back: an unusual presentation. Indian J Dermatol. 2015;60(3):296-7.
5. Ghosh SK, Bandyopadhyay D, Jamadar NS. Nevus lipomatosus cutaneous superficialis: an unusual presentation. Dermatol Online J. 2010; 16(7):12.
6. Turan E, Yesilova Y, Uçmak D, Türkçü G, Çelik ÖI, Gürel MS. Nevus lipomatosus cutaneous superficialis associated with nevus sebaceous of Jadassohn. Indian J Dermatol Venereol Leprol. 2014;80(2):194.
7. Bhushan P, Thatte SS, Singh A. Nevus lipomatosus cutaneous superficialis: a report of two cases. Indian J Dermatol. 2016;61(1):123.
8. Bancalari E, Martínez-Sánchez D, Tardío JC. Nevus lipomatosus superficialis with a folliculosebaceous component: report of 2 cases. Patholog Res Int. 2011; 2011:105973.
9. Nikolowski W. Uber Naevus lipomatodes cutaneous superficialis (Hoffman- Zurhelle). Derm Wschr. 1950; 122:735-42.
10. Hattori R, Kubo T, Yano K, Tanemura A, Yamaguchi Y, Itami S, et al. Nevus lipomatosus cutaneous superficialis of the clitoris. Dermatol Surg. 2003;29(10):1071-2.
11. Kaw P, Carlson A, Meyer DR. Nevus lipomatosus (pedunculated lipofibroma) of the eyelid. Ophthalmic Plast Reconstr Surg. 2005;21(1):74-6.
12. Moss C, Shahidullah H. Nevi and other developmental defects. In: Burns T, Breathnach S, Cox N, Griffiths C, editors. Rook's textbook of dermatology. 8th ed. Oxford: Wiley-Blackwell; 2010. p. 18.1.
13. Villaverde RR, Melguizo JB, Sánchez MCM, Solano JL, Sintes RN. Nevus lipomatosus cutaneous superficialis: coexistence with lipoma. Med cután ibero-lat-am. 2002;30(1): 35-38.
14. Das JK, Sengupta S, Gangopadhyay AK. Nevus lipomatosus superficialis over neck, an atypical site. Indian J Dermatol Venereol Leprol. 2006;72(1):66-7.
15. Jones EW, Marks R, Pongsehirum D. Naevus superficialis lipomatosus. A clinical and pathological report of twenty cases. Br J Dermatol. 1975;93(2):121-33.
16. Dotz W, Prioleau PG. Nevus lipomatosus cutaneus superficialis. A light and electron microscopic study. Arch Dermatol. 1984;120(3):376-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}