


Chan I Thien; Mairam Santos Steffen; Mariana Rita de Novaes Fernandes; Daniela Alves Pereira Antelo
Received on: 26/05/2019
Approved on: 14/07/2019
Study conducted at Pedro Ernesto University Hospital, Universidade do Estado do Rio de Janeiro - Rio de Janeiro (RJ), Brazil.
Financial support: None
Conflict of interests: None
The application of botulinum toxin to patients with sequelae of Bell's palsy is a beneficial adjuvant therapy for the reduction of synkinesia and facial asymmetries. Bell's palsy is the most common cause of facial nerve paralysis.After the paralysis phase of the facial muscles, the condition may evolve with facial asymmetry and synkinesia. In the treatment of synkinesia, punctual injections into the orbicularis and platysma muscles relieve the spasms. Selective application to the unaffected hemiface aims to reduce facial asymmetry and its negative social impact, with improved quality of life.
Keywords: Facial paralysis; Bell palsy; Botulinum toxins, type A; Rehabilitation; Quality of life
Bell's palsy has a sudden onset and is unilateral, with facial paralysis associated with retroauricular pain, dysgeusia, paraesthesia, and hyperacusis. The maximum symptomatology occurs within the first 48-72 hours.1 The severity of paralysis correlates with the duration of facial distension, the extent of facial recovery, and the impairment of quality of life.1
Some patients have incomplete recovery and develop hypertonia, synkinesis, or hyperkinesis. Physical therapy associated with botulinum toxin is an option in the treatment of synkinesis.
In this study, we report the case of a patient with an excellent therapeutic response to the use of botulinum toxin to correct facial asymmetry. The review of the specialized literature, conducted between May and July 2018, used selected scientific articles by searching the Pubmed database. The keywords employed were Bell's palsy, facial palsy, and botulinum toxin.
The inclusion criteria for the studies found were the therapeutic approach of the use of botulinum toxin in the treatment of synkinesis and facial asymmetry after facial paralysis, with emphasis on cases of Bell's palsy. We excluded studies that reported the use of botulinum toxin in other facial asymmetry etiologies.
Soon after, we sought to study and compare the number of patients involved in each study (n), the botulinum toxin used, the average dose used, the application interval, the duration of the effect, and the follow-up time.
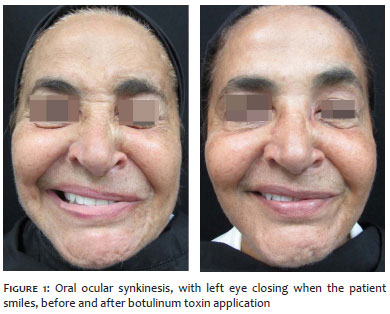
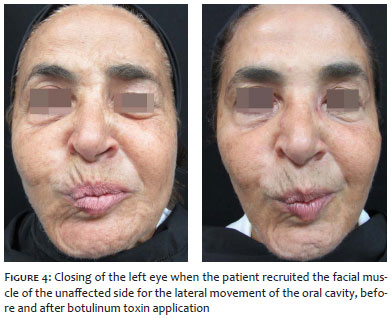
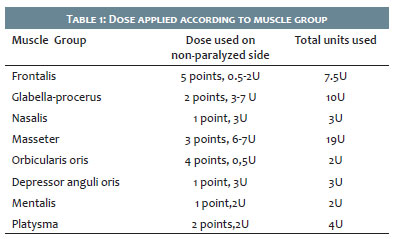
A 54-year-old woman reported that, during the summer of 1999, when moving from one refrigerated area to another with room temperature, she presented paralysis and paresthesia in the left hemiface. Bell's palsy was diagnosed, and she started the treatment with systemic corticosteroid therapy and physiotherapy (cryo and electrostimulation). She had a history of herpes episodes in the same area affected by the paralysis, the last one occurring four months ago. The patient maintained sequelae of left hemifacial paralysis and oro-ocular synkinesis, closing her left eye when smiling (Figure 1). When recruiting the facial muscles of the unaffected side (to contract (Figure 2) or raise the right forehead (Figure 3), as well as to close or move the oral cavity (Figure 4) laterally), the left eye also closes. There is ipsilateral platysma band contracture, causing pain in the region (Figure 5). She is having annual applications of botulinum toxin (she has performed approximately 16 sessions), reducing asymmetry, painful contractions, and synkinesis. Otolaryngologist, neurologist, dermatologist, and physiotherapist are following her multi-disciplinarily. It was decided to apply onabotulinum toxin A (totaling 85 U - Figure 6 and Table 1), using anesthetic cream before the procedure and syringe with a 30G needle in order to reduce the pain of the injection. In the left (affected) hemiface, injections of 1U of botulinum toxin were applied at three points in the orbicularis oculi muscle and of 2U at each of the four points in the platysma muscle to relieve the spasms. The corrugator supercilii muscle was also approached, and injections of 3Us were applied at one point in order to reduce hypertonia. The selective application to the right (unaffected) hemiface, forehead, glabella, orbicularis oculi, orbicularis oris, depressor anguli oris muscle, as well as to the masseter, mental, nasal and platysma muscles was guided in an attempt to improve facial asymmetry and correct some wrinkles, according to Table 1. The functional and aesthetic results were considered satisfactory by the patient in the review 20 days after the procedure.
Bell's palsy is the most common cause of paralysis of facial motor neurons and affects motor, sensory, and parasympathetic fibers. It was first described in 1830 by Charles Bell and presents an incidence rate of 15 to 40 per 100,000 patients.2 According to Eviston TJ et al1, there is no preference for gender, but it tends to occur more frequently in older age groups.
The pathogenesis is still controversial and is related to herpesvirus type 1 infection, nerve compression (ischemic mechanisms) and autoimmunity. Herpesvirus HSV-1, HSV-2 EVZV subtypes are known to latently establish in multiple cranial ganglia, dorsal root and autonomic ganglion following mucocutaneous exposure.3 Intra-axonal degradation and activation of apoptotic pathways in response to the virus, associated with a susceptible phenotype, are believed to contribute to the episode of facial paralysis.1
Combined treatment with acyclovir and corticosteroids for classical Bell's palsy in the acute phase remains controversial.4 Some authors suggest the use of systemic corticosteroids only.
Botulinum toxin is a neurotoxin produced by the anaerobic bacteria Clostridium botulinum.5 It acts on the presynaptic membrane of the neuromuscular junction, inhibiting acetylcholine release and causing a dose-dependent reduction in the muscle contraction.
After the paralysis phase of the facial muscles, there is a tendency for hypertonia. The toxin performs chemodenervation, weakening the hypertonic muscles, and contributing to the correction of facial asymmetry and synkinesis.
Synkinesis corresponds to involuntary abnormal muscle contraction during voluntary movements, attributed to aberrant reinnervation after nerve injury. It may be oro-ocular when the patient closes the eye while smiling or eating, or ocular-oral, when the patient twitches the lip while closing the eye. Activation of the platysmal bands to the movement of the contralateral hemiface also occurs.1 In addition to the platysmal bands, the patient presented oro-ocular synkinesis. In the synkinesis treatment, the botulinum toxin punctual injections into the orbicularis and platysma muscle relieve the spasms and should be associated with physiotherapy, with a particular focus on biostimulation exercises.6 Selective application to the unaffected hemiface, forehead, and depressor anguli oris muscle may be considered in an attempt to improve facial asymmetry, as performed in the reported patient. It is essential to highlight that the application to the paresthetic zygomatic muscle or affected by synkinesis is not recommended to prevent loss of its smile function.1
According to Jowett et al.7, the recommended starting dose for correction of contralateral eyebrow weakness is 9U of toxin into the frontal muscle, distributed in three zones, following a triangular pattern, always 1.5 cm above the eyebrow to prevent eyelid ptosis. The starting dose for the platysma muscle would be 20U distributed in four zones (rectangular pattern), 2 cm below the mentum.
Some patients require three to four annual applications, while others do not benefit from the treatment. The reported patient has already undergone about 16 annual applications without loss of efficacy. She denies adverse events and is undergoing adjunctive physiotherapy.
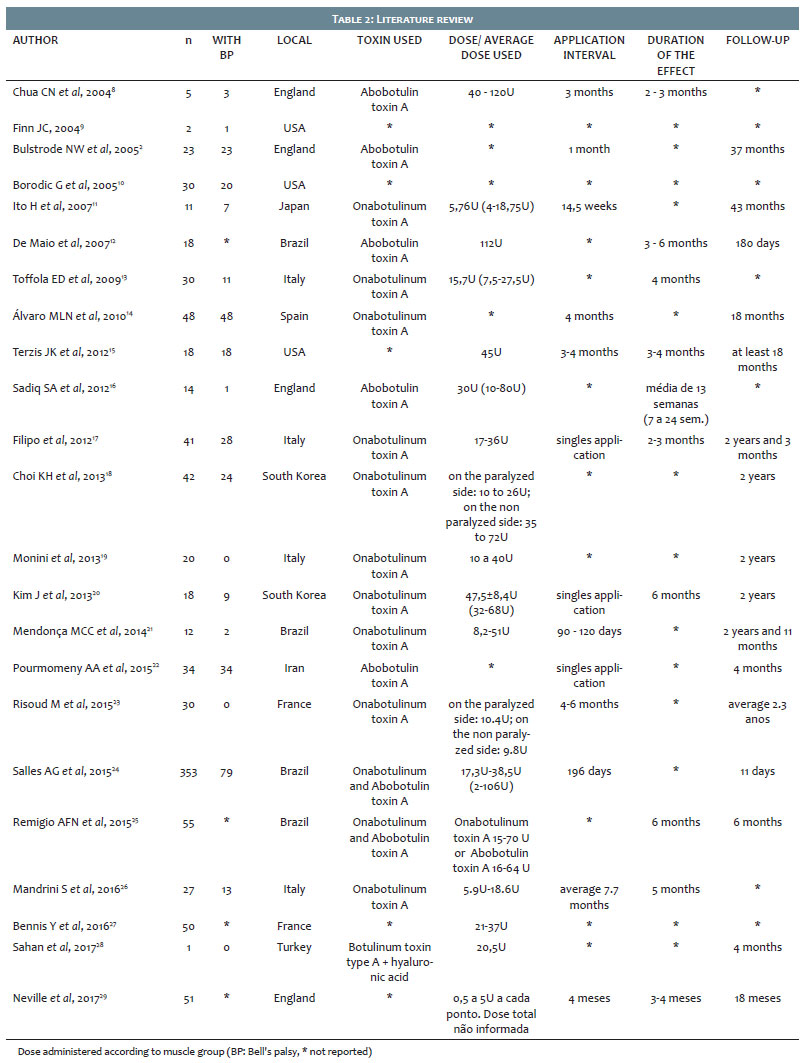
The literature review (Table 2) showed that the number of patients involved in each study on facial paralysis and treated with botulinum toxin ranged from one to 353, and the botulinum toxin used was onabotulinum toxin A and abobotulinum toxin A. The average dose used in each patient ranged from 2U to 120U, the application interval ranged from single application to 7.7 months, with duration of effect from two to six months and follow-up from one month to 11 years.
Botulinum toxin application in the treatment of patients with sequelae of Bell's palsy (approximately 16% of cases)2 is an adjunctive therapy for reducing synkinesis and facial asymmetries. Often performed by other medical specialties, it is also an area of expertise for dermatologists, requiring the study and mastery of the technique for patient safety and obtaining satisfactory results.
To the patients of the Cosmiatrics and Corrective Outpatient Clinic of the Pedro Ernesto University Hospital/ Universidade do Estado do Rio de Janeiro.
Chan I Thien | ORCID 0000-0002-3188-959X
Study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; critical literature review.
Mairam Santos Steffen | ORCID 0000-0003-1728-9640
Preparation and writing of the manuscript; data collection, analysis and interpretation; critical literature review; critical revision of the manuscript.
Mariana Rita de Novaes Fernandes | ORCID 0000-0003-1359-7187
Study design and planning; data collection, analysis and interpretation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
Daniela Alves Pereira Antelo | ORCID 0000-0001-8203-1772
Approval of the final version of the manuscript; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical revision of the manuscript.
1. Eviston TJ, Croxson GR, Kennedy PG, Hadlock T, Krishnan AV. Bell's palsy: aetiology, clinical features and multidisciplinary care. J Neurol Neurosurg Psychiatry. 2015;86(12):1356-61.
2. Bulstrode NW, Harrison DH. The phenomenon of the late recovered Bell's palsy: treatment options to improve facial symmetry. Plastic Reconstr Surg. 2005;115(6):1466-71.
3. Mitchell BM, Bloom DC, Cohrs RJ, Gilden DH, Kennedy PG. Herpes simplex virus-1 and varicella-zoster virus latency in ganglia. J Neurovirol. 2003;9(2):194-204.
4. Kennedy PG. Herpes simplex virus type 1 and Bell's palsy - a current assessment of the controversy. J Neurovirol. 2010;16(1):1-5.
5. Simpson LL. The origin, structure and pharmacological activity of botulinum toxin. Pharmacol Rev. 1981;33(3):155-88.
6. Hadlock TA, Greenfield LJ, Wernick-Robinson M, Cheney ML. Mutimodality approach to management of the paralyzed face. Laryngoscope. 2006;116(8):1385-8.
7. Jowett N, Hadlock, TA. Contemporary Management of Bell Palsy. Facial Plast Surg. 2015;31(2):93-102.
8. Chua CN, Quhill F, Jones E, Voon LW, Ahad M, Rowson N. Treatment of aberrant facial nerve regeneration with botulinum toxin A. Orbit. 2004;23(4):213-18.
9. Finn JC. Botulinum toxin type A: fine-tuning treatment of facial nerve injury. J Drugs Dermatol. 2004;3(2):133-7.
10. Borodic G, Bartley M, Slattery W, Glasscock M, Johnson E, Malazio C, et al. Botulinum toxin for aberrant facial nerve regeneration: double-blind, placebo-controlled trial using subjective endpoints. Plast Reconstr Surg. 2005; 116(1):36-43.
11. Ito H, Ito H, Nakano S, Kusaka H. Low-dose subcutaneous injection of botulinum toxin type A for facial synkinesis and hyperlacrimation. Acta Neurol Scand. 2007;115(4):271-4.
12. de Maio M, Bento RF. Botulinum toxin in facial palsy: an effective treatment for contralateral hyperkinesis. Plast Reconstr Surg. 2007;120(4):917-27.
13. Toffola ED, Furini F, Redaelli C, Prestifilippo E, Bejor M. Evaluation and treatment of synkinesis with botulinum toxin following facial nerve palsy. Disabil Rehabil. 2010;32(17):1414-8.
14. Álvaro MLN, Junyent J, Torrent L. Toxina botulínica y parálisis facial. Nuestra experiencia. Acta Otorrinolaringol Esp. 2010;61(4):277-81.
15. Terzis JK, Karypidis D. Therapeutic strategies in post-facial paralysis synkinesis in adult patients. Plast Reconstr Surg. 2012;129(6):925e-39e.
16. Sadiq SA, Khwaja S, Saeed SR. Botulinum toxin to improve lower facial symmetry in facial nerve palsy. EYE. 2012; 26(11): 1431-36.
17. Filipo R, Spahiu I, Covelli E, Nicastri M, Bertoli GA. Botulinum toxin in the treatment of facial synkinesis and hyperkinesis. Laringoscope.2012; 122(2):266-70.
18. Choi KH, Rho SH, Lee JM, Jeon JH, Park SY, Kim J. Botulinum toxin injection of both sides of the face to treat post - paralytic facial synkinesis. J Plast Reconstr Aesthet Surg. 2013; 66(8):1058-63.
19. Monini S, de Carlo A, Biagini M, Buffoni A, Volpini L, Lazzarino AI, et al. Combined protocol for the treatment of secondary effects from facial nerve palsy. Acta Otolaryngol 2011;131(8):882-6.
20. Kim J. Contralateral botulinum toxin injection to improve facial asymmetry after acute facial paralysis. Otol Neurotol. 2013;34(2):319-24.
21. Mendonça MCC, Lopes MGA, Siqueira RR, Oliveira FQ, Pascoal G, Gamonal ACC. Correction of facial asymmetries and dyskinesias with botulinum toxin type A. Surg Cosmet Dermatol 2014;6(3):221-4.
22. Pourmomeny AA, Asadi S, Cheatsaz A. Management of facial synkinesis with a combination of BTX-A and biofeedback: a randomized trial. Iran J Otorhinolaryngol. 2015;27(83):409-15.
23. Risoud M, Aljudaibi N, Duquennoy- Martinot V, Guerreschi P. Long - termsequelae treatment of peripheral facial paralysis with botulinum toxin type A: Repartition and kinetics of doses used. Ann Chir Plast Esthét. 2016; 61(1):10-15.
24. alles AG, da Costa EF, Ferreira MC, Remigio AF, Moraes LB, Gemperli R. Epidemiologic Overview of Synkinesis in 353 Patients with Longstanding Facial Paralysis under Treatment with Botulinum Toxin for 11 Years. Plast Reconstr Surg. 2015;136(6):1289-98.
25. Remigio AFN, Salles AG, Faria JCM, Ferreira MC. Comparison of the efficacy of OnabotulinumtoxinA and AbobotulinumtoxinA at the 1:3 conversion ratio for the treatment of asymmetry after long-term facial paralysis. Plast Reconstr Surg. 2015;135(1):239-49.
26. Mandrini S, Comelli M, Dall'angelo A, Togni R, Cecini M, Pavese C, et al. Long-term facial improvement after repeated BoNT-A injections and mirror biofeedback exercises for chronic facial synkinesis: a case-series study. Eur J Phys Rehabil Med. 2016;52(6):810-18.
27. Grassi Salles A. Reply: Epidemiologic overview of synkinesis in 353 patients with longstanding facial paralysis under treatment with botulinum toxin for 11 years. Plast Reconstr Surg. 2016;138(2):376e-80e.
28. Sahan A, Tamer F. Restoring facial symmetry through non - surgical cosmetic procedures after permanent facial paralysis: a case report. Acta Dermatovenerol Alp Pannonica Adriat. 2017; 26(2): 41-42.
29. Neville C, Venables V, Aslet M, Nduka C, Kannan R. An objective assessment of botulinum toxin type A injection in the treatment of post-facial palsy synkinesis and hyperkynesis using the synkinesis assessment questionnaire. J Plast Reconstr Aesthet Surg. 2017; 70(11): 1624-28.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}