


José Antônio Jabur da Cunha1; Nabila Scabine Pessotti1; Caroline Andrade Rocha2; Flávia Nunes Maruyama2
Received on: 26/02/2019
Approved on: 11/04/2019
Study conducted at Dermatology Clinic, Medicine Department of the Santa Casa de São Paulo - São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
Nasal surgical defects resulting from the removal of non-melanoma skin cancer represent a challenge for the surgeon due to the anatomical complexity and the high functional and aesthetic relevance of the region.The purpose of this paper is to demonstrate the jigsaw puzzle advancement flap. Resection of basal cell carcinoma was performed in the patient's perialar region, followed by the reconstruction with the jigsaw puzzle advancement flap, with excellent aesthetic and functional results.The presented technique is useful and not yet widespread, and it should be part of the dermatological surgeon's arsenal in the reconstruction of surgical defects located in the nasal ala-perialar region.
Keywords: Nose; Reconstructive surgical Procedures; Surgical flaps
Non-melanoma skin cancer (NMSC) is mainly located on the face, accounting for 75% of cases; of these, 30-35% are located in the nose.1 These tumors are homogeneously distributed in the nose, being more frequent in the wings (nasal ala), followed by the dorsum and tip of the nose.2
The treatment of NMSC is mostly surgical, aiming at complete removal of the lesion and minimal functional and aesthetic damage. Surgical defects located in the nasal ala are challenging to reconstruct since the integrity of this region is very important for maintaining the aesthetics and function of the nose.3 Because it is a prominent and central structure, the nose has considerable aesthetic relevance where minimal distortion may compromise facial harmony.
Several methods are described for the closure of surgical defects of the alar region. Minor defects may heal by secondary closure.3 Superficial defects, in turn, can be repaired with full-thickness skin grafts, often with substantial aesthetic results. Rarely, some defects in the nasal ala may be repaired by direct closure.
Although they are more difficult to perform than grafts, the flaps have aesthetic advantages since they use adjacent skin similar to that of the surgical defect, thus minimizing the problems related to contour, color, and texture.3 There are several types of flaps described for closing the alar region,4 and the surgeon should indicate which technique best suits the patient considering factors such as site, size, depth, and personal experience. New flaps have been described to compose the set of therapeutic options in the nasal reconstruction of surgical defects. Goldberg et al., in 2005, described the jigsaw puzzle advancement flap with good results.4 This paper aims to illustrate and disseminate this technique that, although still little known, is reproducible and useful in the reconstruction of surgical defects located in the nasal alar and perialar regions.
Description of the surgical technique
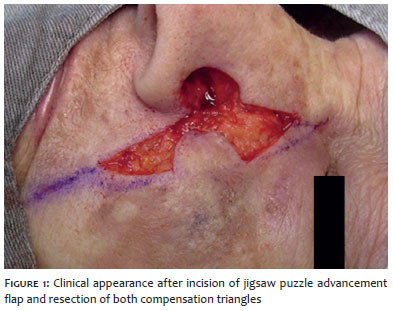
The lesion was excised, resulting in a 13 mm deep surgical defect in the perialar region. An advancement flap was drawn with the offset tissue triangles inferiorly along the nasolabial fold and superiorly along the boundary between the nasal and malar anatomical units (Figure 1). The flap was incised, and the compensation triangles were removed. The flap had a random pedicle and lateral base. The underlying fat was removed from the flap to give it the thickness of the surgical defect. Secondary defects resulting from the excision of compensation triangles were closed with absorbable subcutaneous sutures. Anchorage points were made by attaching part of the flap to the periosteum of the maxillary bone and the piriform foramen. The closure was completed by performing skin sutures using nylon thread (Figure 2).
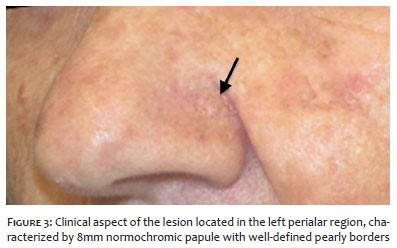
A 72-year-old woman, phototype III, presented a lesion located in the left perialar region (Figures 3 and 4), characterized by an 8mm papule with perlaceous borders and typical dermoscopy. The pathological examination confirmed the diagnosis of basal cell carcinoma.
After total resection of the lesion, which resulted in a 13 mm deep surgical defect in the largest diameter (Figures 1 and 2), the nasal ala was reconstructed with a jigsaw puzzle advancement flap using the tissue located between the nasal and malar anatomical units.
The immediate postoperative period was uneventful, without flap distress, hematoma, seroma, or surgical site infection. The aesthetic result was very satisfactory, without loss of nasogenian sulcus or nasal ala contour, or distortion of free margins. In the six-month postoperative period, the treated region maintained excellent aesthetic and functional results (Figure 5).
The nasal region is a common area for NMSC, and total surgical resection of the lesion is the method of choice for its treatment.5 The functional needs, anatomical characteristics, and aesthetic relevance of the nasal alar and perialar regions are often a challenge to the dermatologic surgeon in reconstructing surgical defects in this area.
Studies show that there is no statistically significant difference regarding complications when comparing flap and total skin grafts.6 Regarding the aesthetic results, it is consensual the superiority of the flaps when well executed, since they present similarity of the texture and color of the local skin and tend to preserve the anatomical contour,3 mainly in deep defects characteristic of the nasal region.
Several flap options are available for the reconstruction of the alar region, such as: V-Y advancement flap, bilobed flaps, and nasolabial interpolation flaps, among others.7, 8 The jigsaw puzzle advancement flap, although unconventional, allows the nasal ala reconstruction while maintaining the contour and structural integrity,4 with great cosmetic result, as showed in our patient. Several authors have used flaps obtained from the nasogenian region and malar area for the reconstruction of nasal alar defects due to good compatibility between the tissues of these different anatomical zones.8
Regarding the choice of the best flap region, the melolabial tissue, which is located between the nasal and malar anatomical units, is an excellent option for nasal and malar region reconstruction.9 Melolabial tissue was considered superior for nasal reconstruction due to its better texture correspondence and absence of noticeable scar when compared to the paramedian forehead flap.10
The advantages of the jigsaw puzzle advancement flap include: 1) excellent aesthetic result due to the similarity of texture and color of the flap skin; 2) incision lines located at the boundary between the nasal, perioral and malar anatomical units, leading to a good scar camouflage; 3) suture anchorage to the periosteum, essential for recreating the alar sulcus and the boundary between the nasal and maxillary anatomical units, also removing the tension of the surgical defect, avoiding the secondary movement of the nasal ala; 4) performance in a single operation.
One of the limitations of this technique is that in order to perform it, the malar region must present sagging skin. It also has the disadvantage of removing healthy skin from both compensation triangles.
Nasal ala amputation may be required for complete tumor removal, leading to extensive and full-thickness surgical defect. In such cases, the jigsaw puzzle advancement flap should be associated with techniques that restore nasal mucosa and cartilage. When performed in isolation, this flap is indicated for the correction of defects that reach the thickness of the dermis as it provides soft tissue thickness but does not provide structural support.4
Surgical defects located in the nasal alar region are frequent since the incidence of basal and squamous cell carcinomas in this region is high. Due to the anatomical characteristics of the alar region, defects located in this area are challenging to reconstruct, involving high aesthetic and functional relevance. The jigsaw puzzle advancement flap is a reproducible, useful, easy-to-perform technique that has excellent aesthetic results. Thus, it should be part of the dermatologic surgeon's arsenal for the reconstruction of surgical defects located in the nasal ala-perialar region.
José Antônio Jabur da Cunha | ORCID 0000-0002-5780-0653
Approval of the final version of the manuscript; study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Nabila Scabine Pessotti | ORCID 0000-0003-0879-2981
Approval of the final version of the manuscript; preparation and writing of the manuscript; data collection, analysis and interpretation; critical literature review; critical revision of the manuscript.
Caroline Andrade Rocha | ORCID 0000-0002-0116-8548
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
Flávia Nunes Maruyama | ORCID 0000-0003-0876-0824
Preparation and writing of the manuscript; critical literature review; critical revision of the manuscript.
1. Santos ABO, Loureiro V, Araújo Filho VJF, Ferraz AR. Estudo epidemiológico de 230 casos de carcinoma basocelular agressivos em cabeça e pescoço. Rev Bras Cir Cabeça Pescoço. 2007;36(4):230-3.
2. Netscher DT, Spira M. Basal Cell Carcinoma: an overview of tumor biology and treatment. Plast Reconstr Surg. 2004;113(5):74e-94e.
3. Lindsay KJ, Morton JD. Flap or graft: The best of both in nasal alar reconstruction. J Plast Reconstr Aesthet Surg. 2015; 68(10):1352-7.
4. Goldberg LH, Kimyai-Asadi A, Silapunt S. "Jigsaw puzzle" advancement flap for repair of a surgical defect involving the lateral nasal ala. Dermatol Surg. 2005; 31(5):569-71.
5. National Comprehensive Cancer Network. NCCN Guidelines for Treatment of Cancer by Site. [Internet]. [uptaded 2018 Aug 31]. Available from: https://www.nccn.org.
6. Rustemeyer J, Gunther L, Bremerich A. Complications after nasal skin repair with local flaps and full-thickness skin grafts and implications of patients' contentment. Oral Maxillofac Surg. 2009; 13(1):15-9.
7. Arginelli F, Salgarelli AC, Ferrari B, Losi A, Bellini P, Magnoni C. Crescentic flap for the reconstruction of the nose after skin cancer resection. J Craniomaxillofac Surg. 2016; 44(6):703-7.
8. Andrade P, Serra D, Cardoso JC, Vieira R, Figueiredo A. Melolabial fold interpolated flap for reconstruction of complex nasal defects. An Bras Dermatol. 2012; 87(5):762-5.
9. Lindsey WH. Reliability of the melolabial flap for alar reconstruction. Arch Facial Plast Surg. 2001; 3(1):33-7.
10. Arden RL, Nawroz-Danish M, Yoo GH, Meleca RJ, Burgio DL. Nasal alar reconstruction: a critical analysis using melolabial island and paramedian forehead flaps. Laryngoscope. 1999;109(3):376-82.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}