


Ana Paula Dornelles Manzoni1,2; Fabiane Kumagai Lorenzini1,2; Caroline Lipnharski1,2; Magda Blesmann Weber1,2; Juliana Fontoura Nogueira1,2; Karoline Rizzati1,2
Received on: 30/06/2019
Approved on: 18/08/2019
Study conducted at the Universidade Federal de Ciências da Saúde de Porto Alegre and the Complexo Hospitalar Santa Casa de Porto Alegre - Porto Alegre (RS), Brazil.
Financial support: None.
Conflito de Interesses: None.
INTRODUCTION: Melasma is a highly common dermatosis that has numerous therapeutic alternatives but tends to be a therapeutic challenge due to its refractory and relapsing nature.
OBJECTIVE: Comparison between intense pulsed light with pulse-in-pulse mode (IPL-PIP) and retinoic acid peel (RAP) for melasma treatment.
METHODS: We conducted six bi-weekly IPL-PIP sessions in the left hemiface and three-monthly RAP sessions in the right hemiface.The Melasma Area and Severity Index (MASI) and MelasQol questionnaires were applied before and one month after the last treatment session.
RESULTS: We observed a reduction of approximately 33% in hemiface MASI with RAP and of 35% in hemiface with IPL-PIP, showing significant improvement of melasma with both methods.There was no statistically significant difference between the two groups. Both practices were well tolerated by patients, but RAP had more reports of adverse events than IPL-PIP.There was a substantial improvement in the quality of life of the patients with both therapeutic methods.
CONCLUSIONS: RAP and IPL-PIP are effective in treating melasma and improving patients' quality of life.There was no statistical difference between the methods concerning lesion clearance and quality of life of patients.
Keywords: Chemexfoliation; Light; Melanosis; Retinoids
INTRODUCTION: Melasma is a highly common dermatosis that has numerous therapeutic alternatives but tends to be a therapeutic challenge due to its refractory and relapsing nature.
OBJECTIVE: Comparison between intense pulsed light with pulse-in-pulse mode (IPL-PIP) and retinoic acid peel (RAP) for melasma treatment.
METHODS: We conducted six bi-weekly IPL-PIP sessions in the left hemiface and three-monthly RAP sessions in the right hemiface.The Melasma Area and Severity Index (MASI) and MelasQol questionnaires were applied before and one month after the last treatment session.
RESULTS: We observed a reduction of approximately 33% in hemiface MASI with RAP and of 35% in hemiface with IPL-PIP, showing significant improvement of melasma with both methods.There was no statistically significant difference between the two groups. Both practices were well tolerated by patients, but RAP had more reports of adverse events than IPL-PIP.There was a substantial improvement in the quality of life of the patients with both therapeutic methods.
CONCLUSIONS: RAP and IPL-PIP are effective in treating melasma and improving patients' quality of life.There was no statistical difference between the methods concerning lesion clearance and quality of life of patients.
Keywords: Chemexfoliation; Light; Melanosis; Retinoids
Melasma is a benign and acquired dermatosis, whose prevalence can reach up to 24% in women in some populations.1 It is characterized by hyperpigmented and asymptomatic spots in photo exposed areas. It is more common in women and patients with higher Fitzpatrick skin phototypes. Genetic, hormonal, vascular, visible light, and ultraviolet light factors are considered the main causal factors.2 According to the literature, this dermatosis, although asymptomatic and with a benign course, causes a significant negative impact on patients' quality of life (QoL), interfering in the psychosocial, family and professional spheres.3
Due to its refractory and recurrent nature, melasma can be a therapeutic challenge. Although there are numerous therapeutic options, none is considered to have the potential for total and definitive improvement. Response to treatments varies widely among patients, requiring, in most cases, combinations of methods and individualization according to tolerability and clinical response.4 Thus, this study aims to compare the effectiveness, tolerance, adverse events, and quality of life of patients with melasma treated in a hemiface with a traditional and widely known option (retinoic acid peel - RAP) and in the other with a promising but still little studied option (intense pulsed light with pulse-in-pulse mode - IPL-PIP). This technology emits the same wave as IPL but fractionates the pulse duration of 10 ms into 100 sub-pulses of 40 µs. Through these fractional pulses, PIP can remove more gently the unwanted pigmentation without aggravating or exacerbating melasma.5
This is a split-face, single-center, clinical trial conducted in 17 patients with melasma. The inclusion criteria were the presence of clinically typical melasma lesion, located on the face, bilateral, in patients with Fitzpatrick skin phototype I and IV.2 The exclusion criteria were pregnancy, lactation, use of oral medications that influenced melasma treatment (such as oral contraceptives), skin lighteners (or bleachers), and laser or light treatment for melasma for six months before inclusion. The institution's research ethics committee (UFCSPA) approved the study, and all patients signed an informed consent form (ICF).
The face was cleaned with 2% chlorhexidine aqueous solution and gauze. On the IPL-PIP hemiface, (Multiwave Laser Toning of LMG Solon, Guaxupé, MG, Brazil), a thin layer of water-based gel was applied, and the session started at 550 nm to 800 nm wavelength, fluency 12 J/cm2 to 15 J/cm2, two to three times until reaching mild erythema that disappeared in approximately 40 seconds. Treatments were administered to the left hemiface at two-week intervals with a total of six ILP-PIP sessions. The right hemiface was treated using RAP 5% once a month in a total of three sessions. The patients were instructed to wash the RAP with soap and water after six hours of its application. After each session, patients received a form with guidelines and care to be taken after the procedure, especially strict 4/4 hour photoprotection with Minesol Actif® SPF 80 (Johnson & Johnson do Brasil Indústria e Comércio de Produtos para Saúde Ltda., São Paulo, SP, Brazil) provided by the researchers, and no other topical medications were used. In this same form, patients should describe possible adverse events if they occurred.
Two researchers assessed the modified MASI score at the beginning of the protocol and one month after the last treatment, and the patients answered a quality of life questionnaire (MelasQoL-BP).3,6
Statistical analysis was performed using absolute and relative distributions, as well as measures of central tendency and variability. Regarding the comparison of the means assessed during the follow-up, the study of the data distributions for normality was conducted using the Shappiro Wilk test. In the comparison of continuous variables between two dependent groups (pre- and post-treatment evaluation as well as comparison between the hemifaces), the t-Student and Wilcoxon tests were used. The magnitude of the differences was calculated from the effect size, where an effect size of 0.20-0.49 was considered small; 0.500.79, moderate; and ≥0.80, large magnitude effect. Data were analyzed using the Statistical Package for Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA, 2008) for Windows. For the statistical decision criteria, the significance level of 5% was adopted.
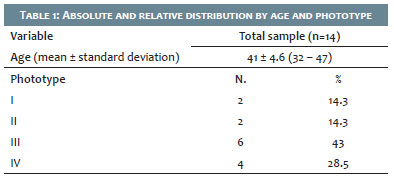
The comparative study between melasma treatment with ILP-PIP and RAP 5% initially involved 17 patients. We excluded one patient after the first session because she presented post-inflammatory hyperpigmentation on the IPL-PIP hemiface. Two other patients were excluded from the study due to loss to follow-up. Therefore, the results were analyzed based on a sample of 14 female patients, aged 32 to 47 years (mean 41 years and SD ± 4,6), and with a predominance of Fitzpatrick skin phototype III in 43% of the patients (Table 1).
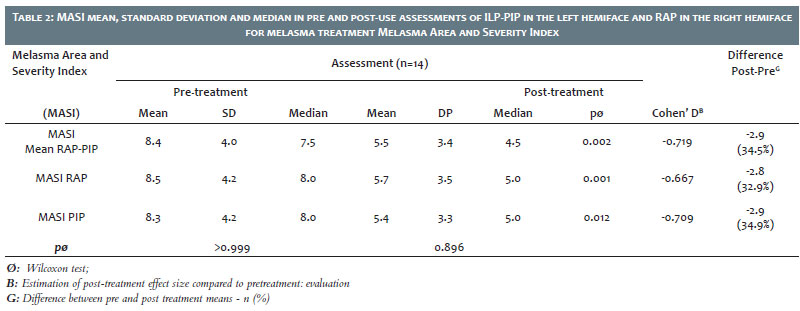
Analysis of pre- and post-treatment MASI indices showed a significant improvement in melasma with both therapeutic modalities (p=0.002). The individual analysis of each hemiface with its respective intervention evidenced the same significant reduction in severity (p=0.001 for RAP and p=0.012 for ILP-PIP). ILP-PIP presented a slight 2% superiority in improving melasma, but with no statistical significance (Table 2).
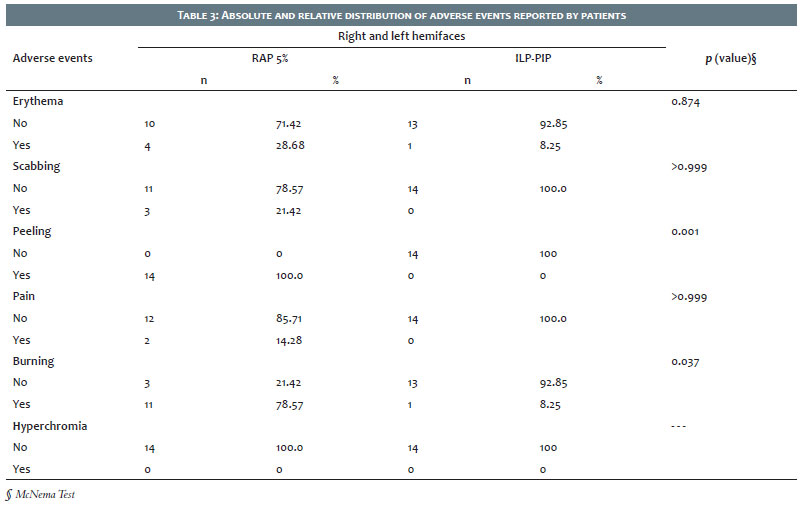
Table 3 shows adverse events with both techniques. RAP presented significantly more burning (78.5% of patients; p=0.047) and peeling (100% of patients; p=0.001) than ILP-PIP (burning in 21.4% of patients and peeling in no patients). Regarding other unwanted events, the differences observed between the treatments were not significant.
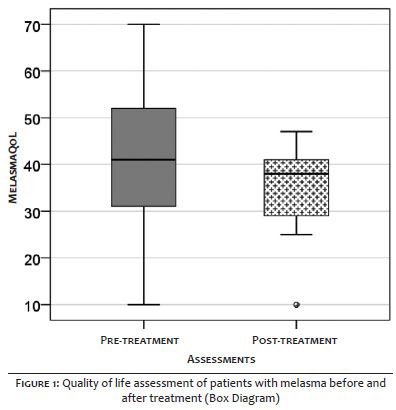
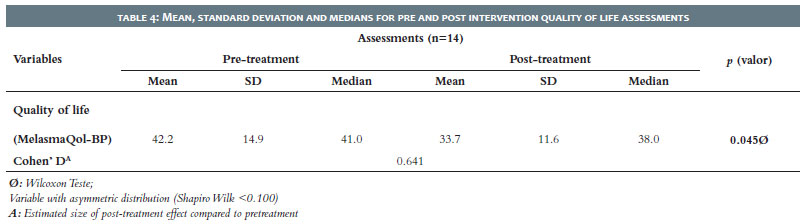
Regarding the assessment of the quality of life of patients with melasma, there was a significant improvement with both treatments (p=0.045) demonstrated by reducing the MelasQoL-BP score by approximately 20%. The effect size of melasma treatment on patients' quality of life was classified as moderate (dCohen= = 0.641) (Figure 1 and Table 4).
Melasma is considered a chronic dermatosis with numerous therapeutic options, but not always enough to achieve satisfactory and lasting improvement.4,7 Over the last decades, studies have shown that its presence goes far beyond a simple change of aesthetic nature to acne with a significant impact on the quality of life of its carriers.3,8 Thus, we continue looking for new therapeutic options that are promising and effective for its treatment. In melasma, high-fluency laser and ILP treatments to treat pigments are not helpful because they can aggravate melasma.5 PIP does not raise the temperature of the target tissue enough to destroy it, gradually increasing skin temperature, thus being safer than conventional ILP. It applies a very low fluency and does not destroy active melanocytes with melanosomes.5,9 Previous experience showed that PIP has induced clinical improvement with fewer treatment sessions (4-6), and may have the additional benefit of avoiding possible adverse events.9 We chose to use RAP 5% as a PIP system control as it is a well-known, effective, and scientifically documented traditional treatment alternative for melasma.10,11
Our study demonstrated a significant improvement of melasma with both treatment modalities in the Melasma Area and Severity Index (MASI) analysis but without superiority between the two intervention methods. However, the PIP system showed a slight superiority of 2% over RAP, which may represent a tendency to significance with the increase of the studied sample.
RAP presented significantly more adverse events than PIP. The presence of burning and peeling, already well described and expected with RAP, confirmed this fact. Although very common, they were described as mild and transient. In the evaluation of PIP para effects, only one patient reported mild erythema, which is a very comfortable procedure with no recovery time to return to daily activities. However, it’s essential to remember that a patient was excluded from the study after a PIP session due to the presence of post-inflammatory hyperpigmentation in the hemiface where this treatment was applied. In addition to suspending her follow-up in the study, we recommended the topical use of hydroquinone 4% and strict photoprotection. In approximately 15 days, the patient had a total improvement of this dyschromia.
In this study, we also assessed the impact on patients’ quality of life (QoL) secondary to melasma, and our findings corroborated the worldwide literature showing its decrease. After treatment, there was a significant improvement in the quality of life of the study patients, measured with moderate impact. This fact reinforces the importance of always offering some therapeutic options to patients, regardless of total or partial improvement, because, despite their chronic and relapsing course, patients experience improvement in their quality of life.
Both RAP 5% and PIP systems are significantly effective options for melasma treatment. Despite a slight tendency for the superiority of IPL-PIP over RAP, we found no significant difference between them. Regarding adverse events, RAP is significantly accompanied by burning and peeling, but mildly and transiently. PIP, on the other hand, does not present discomfort and does not require recovery time by patients, but it is a more expensive therapeutic option, in addition to one patient having post-inflammatory hyperchromia. We emphasize the need for further studies with larger samples.
Ana Paula Dornelles Manzoni | 0000-0001-6184-4440
Approval of the final version of the manuscript; study design, and planning; data collection, analysis and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review; critical revision of the manuscript.
Fabiane Kumagai Lorenzini | 0000-0001-6365-8705
Preparation and writing of the manuscript; data collection, analysis, and interpretation; active participation in research orientation; intellectual participation in propaedeutic and/or therapeutic conduct of studied cases; critical literature review.
Caroline Lipnharski | 0000-0002-6902-6909
Study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; critical literature review.
Magda Blesmann Weber | 0000-0001-5885-5851
Approval of the final version of the manuscript.
Juliana Fontoura Nogueira | 0000-0001-8462-2269
Study design and planning; preparation and writing of the manuscript; data collection, analysis and interpretation; critical literature review.
Karoline Rizzati | 0000-0002-4327-535X
Study design and planning; preparation and writing of the manuscript; data collection, analysis, and interpretation; critical literature review.
1. Sarkar R, Gokhale N, Godse K, Ailawadi P, Arya L, Sarma N, et al. Medical management of melasma: A review with consensus recommendations by Indian pigmentary expert group. Indian J Dermatol 2017; 62(6):558-77.
2. Handel AC, Miot LDB, Miot HA. Melasma: a clinical and epidemiological review. An Bras Dermatol. 2014;89(5):771-82
3. Maranzatto CFP, Miot HA, Miot LDB, Meneguin S. Psychometric analysis and dimensional structure of the Brazilian version of melasma quality of life scale (MELASQoL-BP). An Bras Dermatol. 2016; 91(4):422-8.
4. Zhou LL, Baibergenova A. Melasma: systematic review of the systemic treatments. Int J Dermatol. 2017; 56(9):902-8.
5. Chung JY, Choi M, Lee JH, Cho S, Lee JH. Pulse in pulse intense pulsed light for melasma treatment: a pilot study. Dermatol Surg. 2014;40(2):162-8.
6. Pandya AG, Hynan LS, Bhore R, Riley FC, Guevara IL, Grimes P, et al. Reliability assessment and validation of the Melasma Area and Severity Index (MASI) and a new modified MASI scoring method. J Am Acad Dermatol. 2011; 64(1):78-83.
7. Trivedi MK, Yang FC, Cho BK. A review of laser and light therapy in melasma. Int J Womens Dermatol. 2017; 3(1):11-20.
8. Ikino JK, Nunes DH, da Silva VPM, Fröde TS, Sens MM. Melasma and measure of the quality of life in brazilian women. An Bras Dermatol. 2015; 90(2):196-200.
9. Yun WJ, Lee SM, Han JS, Lee SH, Chang SY, Haw S, et al.. A prospective, split-face, randomized study of the efficacy and safety of a novel fractionated intensepulsed light treatment for melasma in Asians. J Cosmet Laser Ther. 2015;17(5):259-66.
10. Rivas S, Pandya AG. Treatment of melasma with topical agents, peels and lasers: an evidence-based review. Am J Clin Dermatol. 2013; 14(5):359-76.
11. Magalhães GM, Borges MFM, Queiroz ARC, Capp AA, Pedrosa SV, Diniz MS. Double-blind randomized study of 5% and 10% retinoic acid peels in the treatment of melasma: clinical evaluation and impact on the quality of life. Surg Cosmet Dermatol 2011;3(1):17-22.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}