


Ana Cláudia Cavalcante Espósito1; Eliandre Palermo1; Osório Alves C. de Castro Lara2; Marcela Pesce de Souza2; Mariana Bellini Vieira1 Luiz Roberto Terzian1
Received on: 31/05/2018
Approved on: 06/06/2019
This study was performed at the Faculdade de Medicina do ABC, Santo André (SP), Brazil.
Financial support: None
Conflict of interests: None
There are a few descriptions in the literature on surgical techniques for the closure of synchronous facial defects. We report three cases of patients with synchronous lesions on the face, which were reconstructed using the following types of flaps: Yin-Yang double-opposing rotation; Burrow's triangle advancement; and a combination of the dorsal nasal flap with the transposition flap. Reconstructions of synchronous facial defects represent challenges to dermatologic surgeons, especially when one of the lesions is located in the nose. In cases involving relatively small defects and not so far apart, there is the possibility of a single flap to close both defects.
Keywords: Surgical flaps; Mohs surgery; Carcinoma, basal cell
The most common body site for the occurrence of skin cancer is the face. Surgical treatment of these lesions requires an approach based on oncological principles associated to functional and aesthetic reconstructions. 1
The literature brings together numerous reports of flaps being used to close single facial defects, however there are few descriptions of simultaneous closure of two lesions located near to each other. 1 The synchronous occurrence, excision and closure of facial lesions in the same surgical act represents a challenge to the dermatological surgeon.
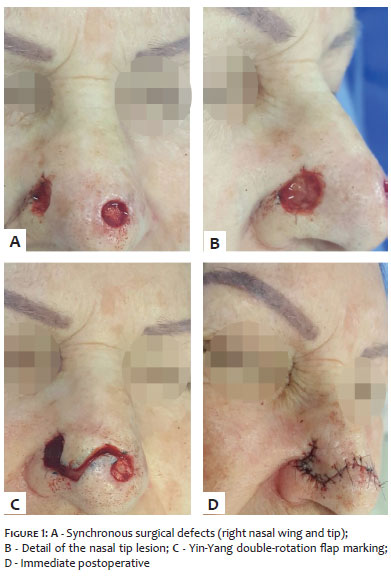
Case 1 – A 76-year-old female patient, with absence of comorbidities, underwent Mohs micrographic surgery (MMC) for the excision of a superficial basal cell carcinoma (BCC) (initial size: 0.8cm x 0.6cm) in the right nasal wing and a well differentiated squamous cell carcinoma in situ (initial size: 0.4cmx 0.4cm) in the nasal dorsum. Only one MMC phase was required for complete resection of both tumors. The final defects measured 1.2cm x 1.2cm (nasal wing) and 0.6cm x 0.6cm (nasal dorsum) ( Figures 1A and B). Due to the proximity of the lesions and the relatively small size of the defects, it was possible to use the untouched skin located between the lesions to perform a Yin-Yang double-rotation flap to close both defects ( Figures 1B and C). On the seventh postoperative day, the aesthetic-functional outcome was very satisfactory, without any distortion of the nasal tip or wing (Figure 2).
Case 2 - A 53-year-old male patient, with absence of comorbidities, bore three asymptomatic lesions on the face for one year. The lesions were operated in the same surgical procedure using the MMC technique. In the glabella, he had a solid and micronodular BCC measuring 1.3cm x 0.9cm, which required only one phase for the complete resection. The final surgical defect of this lesion measured 2.2cm x 1.3cm and the closure was carried out directly (edge to edge).
Additionally, there was a solid BCC measuring 1.0cm x 1.0cm in the left lateral nasal wall, that was fully resected with two MCC phases (final defect: 1.9cm x 1.9cm). Close to this defect, in the left malar region, a micronodular BCC was also resected (initial size: 0.6cm x 0.5cm) in a single MMC phase (final defect: 1.4cm x 1.3cm). The untouched skin located between the defects allowed the implementation of a two-triangle Burrow's advancement flap (Figure 3).
Case 3 – A 70-year-old female patient, former rural worker, had three facial lesions that were resected by MMC (in a single phase). The first lesion was an adenoid BCC (0.6cm x 0.5cm) in the right supralabial region, whose final defect (1.4cm x 1.0cm) was closed edge to edge.
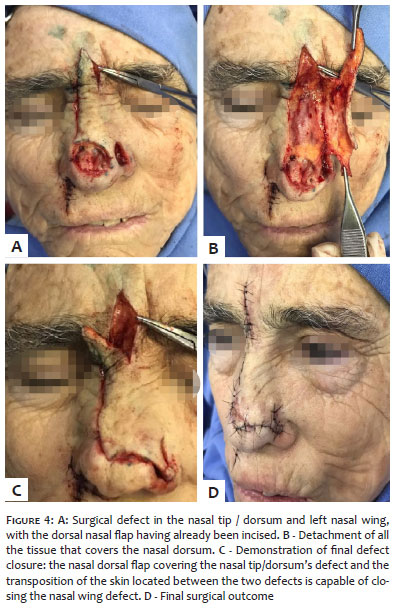
The second lesion was a solid BCC (1.9cm x 1.3cm) in the nasal tip and dorsum, whose final surgical defect measured 2.4cm x 1.7cm. In the left nasal wing, another solid BCC (third lesion) could be observed (0.8cm x 0.6cm), whose surgical defect measured 1.2cm x 0.8cm. The size and location of the lesions did not allow the closure of both defects with a single flap. The authors of the present paper then chose to use a combination flap: a nasal dorsal flap aimed at closing the larger defect, and the untouched skin between the defects being used to transpose and close the nasal wing's defect (Figure 4). There were no distortions of the wing or nasal tip entailing from the implementation of the flaps.
In all three cases, at least one of the lesions was located in the nose, which is the facial site most frequently affected by skin cancer (25.5% of the cases) and also the one that implies greater difficulty for reconstruction. 3, 4 When surgical defects are double – and especially when at least one of them is located in the nose – great technical knowledge and a certain degree of creativity is required from the dermatologist physician. 2
In case 1, a double rotation flap was used for concomitant closure of the lesions. A curved line with the shape of an "S" is drawn tangentiating the two defects, with the double rotation movement being subsequently performed. Such a flap is also called Yin-Yang, in view of the similarity that flap's design has to the traditional Chinese symbol. 1
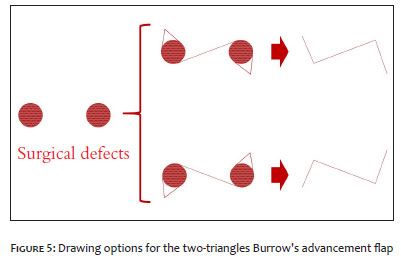
In case 2, the closure was carried out using a two-triangle Burrow's advancement flap. The flap's preparation is relatively simple: a line is drawn tangentiating the defects in a way to unite them. Next, the compensation triangles (Burrow triangles) are drawn – one in each defect – opposite to the tangential incision site. In this manner, for each pair of defects there are two possibilities for drawing this flap (Figure 5). It is up to the dermatological surgeon to evaluate which option is most favorable, in view of the tissue's mobility, skin's tension lines and the patient's rhytids. 5, 6 Even though the resulting suture line is long, it is rather aesthetic (Z-shaped) and promotes a decrease in tension along the incision line. 5, 6
In case 3, the occurrence of two large surgical defects in body sites with poor tissue redundancy did not allow primary closure or reconstruction using a single local flap. 7 An option to close the larger defect – on the nasal tip and dorsum – would be performing a cutaneous graft. Nevertheless, the use of a tissue with another color, the possible demarcation of the borders, and the natural convexity of the nasal tip would tend to lead to an unfavorable aesthetic result. The authors of the present paper then made a decision for performing two independent flaps: a dorsal nasal flap and a transposition flap using the untouched tissue located between the two surgical defects. This association allowed the closure of both defects and avoided the superior deviation of the nasal wing.
The nasal dorsum's flap – or Rieger's flap – involves the rotation and advancement motions of the skin from the proximal two thirds of the nose and glabella for the defect's closure in the distal third of the nose. 8 It is useful for rebuilding defects up to 2.5cm in diameter. It is considered a safe and of low morbidity flap, despite involving large portions of tissue. 9 Using this flap, it was possible to close the larger defect (nasal tip). The untouched skin located between the two defects was used as a transposition flap for the closure of the smaller defect.
Reconstructions of synchronic defects on the face in a single surgical time is challenging to dermatological surgeons, is special when one of the lesions is located in the nose. In cases involving relatively small defects that are located not so far apart from each other, it is possible to implement a single flap to close both defects.
Ana Cláudia Cavalcante Espósito | ORCID 0000-0001-9283-2354
Study design and planning; manuscript preparation and drafting.
Eliandre Palermo | ORCID 0000-0002-9320-9967
Study design and planning; manuscript preparation and drafting; critical review of the literature.
Osório Alves C. de Castro Lara | ORCID 0000-0003-3899-4293
Preparation and drafting of the manuscript; intellectual participation in propaedeutic and / or therapeutic approach of the cases studied.
Marcela Pesce de Souza | ORCID 0000-0001-9288-4218
4218 Intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied; critical review of the literature; critical review of the manuscript.
Mariana Bellini Vieira | ORCID 0000-0002-7164-5573
Approval of the final version of the manuscript; research guidance; intellectual participation in therapeutic and / or therapeutic approach of the cases studied.
Luiz Roberto Terzian | ORCID 0000-0002-9342-7227
Approval of the final version of the manuscript; intellectual participation in propaedeutic and / or therapeutic approach of the cases studied.
1. Pereira CS, Botero EB, Reis GCN dos, Ota FS. Reconstruction of two defects on the face close to each other: reports of two cases. Surg Cosmet Dermatol. 2016;8(4 Supl. 1):S64-6.
2. Gon ADS, Araújo FM. Zetaplastia como alternativa para fechamento de defeito cirúrgico duplo. Surg. cosmet. dermatol.2015; 7(2): 162-164.
3. Deluca J, Tappeiner L, Pichler M, Eisendle K. Using the Peng flap for a wide dorsal nasal defect. J Dtsch Dermatol Ges. 2014;12(11):1060-2.
4. Salgarelli AC, Bellini P, Multinu A, Magnoni C, Francomano M, Fantini F, et al. Reconstruction of Nasal Skin Cancer Defects with Local Flaps. J Skin Cancer. 2011:181093.
5. Boggio P, Gattoni M, Zanetta R, Leigheb G. Burow's triangle advancement flaps for excision of two closely approximated skin lesions. Dermatol Surg.1999;25(8):622-5.
6. Gormley DE. A brief analysis of the Burow's wedge/triangle principle. J Dermatol Surg Oncol. 1985;11(2):121-3.
7. Lee DM, Bae YC, Nam SB, Bae SH, Choi JS. Reconstruction of Large Facial Defects via Excision of Skin Cancer Using Two or More Regional Flaps. Arch Plast Surg. 2017;44(4):319-23.
8. Redondo P, Bernad I, Moreno E, Ivars M. Elongated Dorsal Nasal Flap to Reconstruct Large Defects of the Nose. Dermatol Surg. 2017;43(8):1036-41.
9. Jena A, Gangasani R, Reddy NR, Patnayak R. Reconstruction with Dorsal Nasal Flap after Excision of Basal Cell Carcinoma of the Nose. J Cutan Aesthetic Surg. 2017;10(1):54-5.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}