


Luísa Saccaro1; Carolina Zárate1; Rodolfo Alves Lopes2; André Cesar Antiori Freire Pessanha3
Received on: 20/12/2018
Approved on: 05/04/2019
Study conducted at the Dermatology Service of the Universidade de Mogi das Cruzes - Mogi das Cruzes (SP), Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: The gold standard diagnosis of cutaneous melanoma is essentially histological. Dermoscopy adds to clinical examination improved sensitivity and specificity.
OBJECTIVE: To evaluate the histological profile of risk melanocytic lesions excised in a dermatology service.
METHODS: Case review through Excel spreadsheet and survey of dermoscopic, histological and topographic data (January 2017 to December 2018).
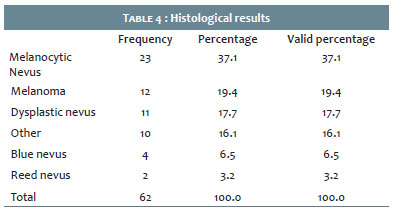
RESULTS: Data from 62 suspected melanoma lesions were evaluated in this period. The main histological results were: melanocytic nevi (37.1%), melanoma (19.35%), and dysplastic nevi (17.7%).
CONCLUSIONS: The positive predictive value for melanoma was 19.35%, considering the search for an early diagnosis in patients at risk.
Keywords: Neoplasms; Melanoma; Dermatology
Melanoma is a neoplasm with a high probability of metastasis. Early diagnosis is a function of the dermatologist since this significantly improves the patient's prognosis.1 Patients with multiple nevi, dysplastic nevus syndrome, personal or family history of melanoma, and with spots in transformation above the age of 35 should be considered at risk.
The gold standard diagnosis of cutaneous melanoma is essentially histological.2 The clinical aspects of melanocytic lesions (nevi) contribute to the clinical hypothesis. The ABCDE rule is used (A- Asymmetry; B- border irregularity; C- color variation; D- Diameter >6 mm; E-Evolving, which includes rapid growth, pruritus, bleeding, and ulceration). The greater number of these signs indicates a higher probability of melanoma.1
Dermoscopy (polarized light that allows visualization of epidermal and dermal structures) is a feature that increases the accuracy of clinical examination and allows the differential diagnosis between a melanocytic and a non-melanocytic lesion.2 Among melanocytic lesions, the pattern analysis stratifies its risk category but its definitive diagnosis will be histological. Through the clues to malignancy, the dermoscopy also contributes to the excision indication of initial atypical melanocytic lesions and melanomas in situ. In addition, comparative analysis of multiple nevi patterns in the same patient may define the excision of a chaotic lesion with a different pattern ("ugly duckling sign").3 This method provides sensitivity ranging from 62% to 94 %.2 Procianoy, 2009, also demonstrated the sensitivity of the dermoscopy through the Pattern Analysis method, finding the value of 91.7%, while the specificity of the method was 41.7%.2 It has already been shown that dermoscopy increases sensitivity and specificity of the melanoma diagnosis in 35% when compared with the clinical diagnosis.2 It is important to remember that dermoscopy has been contributing to an earlier diagnosis of melanoma. Currently, in Sweden, 40% of the diagnosed melanomas are in situ (in 1996 this number was 20%).4
There are several methodologies based on dermoscopy to stratify the risk of melanocytic lesions. The "Chaos and Clues" (Kitler H) method is a simple algorithm to facilitate the medical decision as to whether or not to excise a certain lesion.3 For lesions exhibiting chaos (asymmetry of structures and/or color), one must look for clues to malignancy 3 (Table 1 of clues to malignancy for pigmented lesions exhibiting chaos). This method showed a sensitivity of 90.6% and specificity of 62.7% (malignancies) in a study involving 463 excised pigmented lesions, 29 of which were melanomas.3
Analyzing the dermoscopy, sensitivity is the method ability to detect melanoma in the population. Usually, these numbers are expressive among the several algorithms, i.e., although many benign lesions are removed, melanomas are very little unnoticed. Moreover, specificity is the ability to find benign lesions in the population. This number is expressive but tends to be smaller than the sensitivity because there are many cases of false positive (considering that dysplastic nevus or even melanocytic nevus may present chaos to dermoscopy and/or evolve with growth asymmetry). The positive predictive value regarding an examination is: "since this examination was abnormal, the probability is that the individual is actually sick."5 For the same reason of the specificity, its value tends to be smaller than that of the sensitivity and even smaller than that of the specificity because, in the universe of the melanocytic lesions, finding "normal" is a simpler task than trying to diagnose an initial melanoma considering that in this evolutionary process nevi, dysplastic nevi and melanomas may present the same dermoscopic characteristics without a specific feature to differentiate them, revealing at this moment the dermoscopy limitation despite its unquestionable importance.
To evaluate the histological profile of excised melanocytic lesions at risk, based on clinical standards, clinical history, and dermoscopic method.
A study conducted at the Dermatology Service of the Universidade de Mogi das Cruzes, São Paulo, Brazil, from January 2017 to December 2018, which assessed 62 suspected melanoma lesions.
Retrospective, epidemiological study analyzing the information contained in the Excel spreadsheet of suspicious melanocytic lesions with clinical, dermoscopic, and histological findings. Analysis of medical records of the UMC Polyclinic. The research was approved by the Committee for Ethics in Research of the UMC; CAAE (Presentation Certificate for Ethical Appraisal) number 60657516.0.0000.5497. Data from adults with melanocytic lesions at risk from UMC were assessed during 2017 and 2018. Clinical description and dermoscopy were the criteria used to choose excision. In this period several dermoscopic algorithms were used, but mainly Chaos and Clues (year 2018), so we tried to standardize this study by adapting the other dermoscopic descriptions to the elements of this one that was the most practiced method. The evaluation of the results was conducted from the correlation with the histological reports.
The lesions were recorded in a database with the following information: diagnostic hypothesis, age, sex, and lesion topography. After this step, the diagnostic hypothesis (clinical and dermoscopic data) was compared with the final histological result.
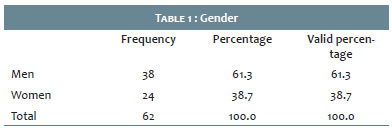
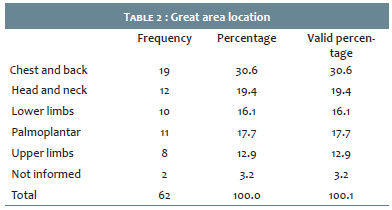
Sixty-two skin lesions with a diagnostic hypothesis of melanoma were assessed, being 24 men (38.7%) and 38 women (61.3%), with a mean age of 56 years (Table 1). The body location with the most biopsied lesions was the trunk with 30.6% of the cases as shown in Table 2.
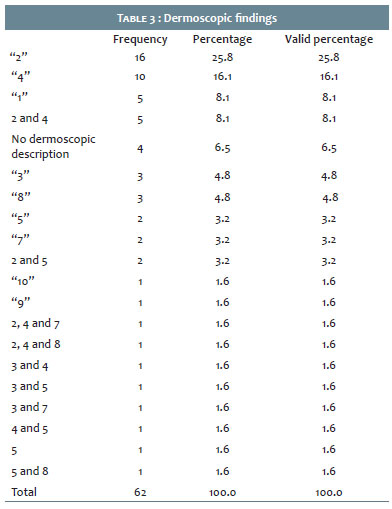
Dermoscopy showed a greater proportion of lesions with spots and lumps asymmetrically distributed in 25.8% of the cases, followed by areas without structure (16.1%) according to Table 3.
As for the histological results (definitive diagnoses), melanocytic nevi were the most frequent lesions (37.1%), followed by melanomas with 19.4% of the cases (Table 4).
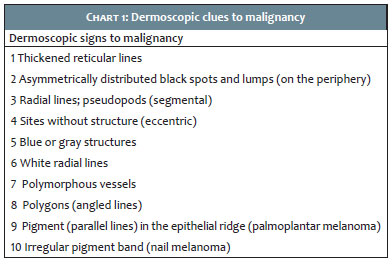
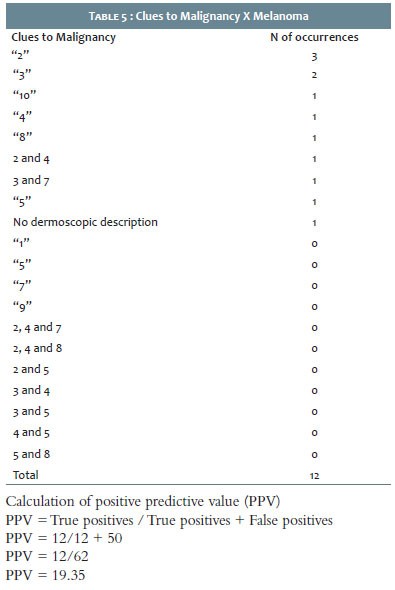
Of the confirmed cases of melanoma, the order of frequency of the finding 2 (Chart 1) coincided with the general excision, i.e., it was the most found, followed by the radial lines/ pseudopods (two cases) (Table 5).
Dermoscopy is an instrument of great importance for the screening of risk diagnoses: low, moderate, and high – criteria that can be used for melanocytic and non-melanocytic lesions. The knowledge of the patterns that allow such stratification defines an appropriate behavior before the patient.
The present study assessed patients with supposedly melanocytic lesions (clinically suspected melanoma or nevoid), with moderate or high risk for melanoma. The following were considered in the decision for excision: personal or family history of melanoma, clinical history, clinical aspect (ABCDE), and multiple nevi, defining the patient at risk.
The dermoscopic "Chaos and Clues" pattern contributes to the more invasive decision in dubious cases. The higher number of patterns (dermoscopic chaos) indicated a greater probability of melanoma. However, a single pattern among clues to malignancy (clue to malignancy Table) may already represent a melanoma (usually initial: the diagnostic precocity is a major goal in patients at risk or not necessarily at risk). This is what is observed in Table 5: leading cases of melanoma with only one pattern (which is a clue to malignancy): spots and lumps asymmetrically distributed.
A large number of excised benign lesions (melanocytic nevus) is evident, demonstrating that despite the sum of data that confirms the risk, they do not define the diagnosis, which is essentially histological. Carrera et al., when comparing dermoscopic teaching algorithms, found modest levels of diagnostic accuracy.6 In this study, the "three-points checklist" had the lowest sensitivity (68.9%). At the same time, the Menzies method had the highest sensitivity and the lowest specificity (95.1% and 24.8%, respectively). The "ABCDE rule" showed the highest specificity (59.4%), higher than the "Chaos and Clues" method (40.2%). From these last numbers, the large number of false positives is deduced. The bias of the clinical experience of those who performed the dermoscopy is also considered.4
We must consider, among other factors, the interaction between the dermatologist and the pathologist so that in lesions with high suspicion a more accurate microscope slide revision is conducted. The bias of histopathology becomes more evident when one does not know the pathologist who studies the microscope slide, and more than that, several pathologists analyze the samples of the study4 in question, and the interpathologists subjectivity is a limitation of this study.
In this sample, we observed high frequencies of blue nevus/ Reed nevus that have common dermoscopic features (clues) with invasive melanoma (areas without bluish or blackened structures and peripheral pseudopods in the case of Reed nevus).
It should be emphasized that we did not include in the sample supposedly benign excised lesions nor did we perform a dermoscopic imaging test with medical evaluations of this service to quantify the sensitivity and the specificity since we do not have the possible false negatives of dermoscopy. It is known that very recent melanomas may not be discernible from nevi, hence the importance of early follow-up in at-risk patients or of excisions in cases of doubt.7
In the present study, a positive predictive value (PPV) of 19.35% was found for the diagnosis of melanoma. In the Ahnlide study, I7 a PPV of 51% was found for 108 excised melanocytic lesions. This same study also mentions Heal et al., with a PPV of 33.3%, but points out that the prevalence of melanoma (results from Sweden and Australia, respectively) tends to increase this number.
In this study involving 62 lesions of clinical and dermatoscopic risk, we found 12 cases of melanoma, i.e., a positive predictive value of 19.35%. Rigorous dermoscopic follow-ups and the formation of risk scales may be alternatives to optimize the excision criterion. On the other hand, given the magnitude of the progression of melanoma, failing to make an early diagnosis can be fatal for the patient.
Luísa Saccaro | ORCID 0000-0003-0195-0537
Statistical analysis, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation.
Carolina Zárate | ORCID 0000-0001-5737-356X
Statistical analysis, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation.
Rodolfo Alves Lopes | ORCID 0000-0001-5560-2453
Preparation and writing of the manuscript, critical review of the original.
André Cesar Antiori Freire Pessanha | ORCID 0000-0001-9806-4245
Statistical analysis, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation.
1. American Academy of Dermatology Ad Hoc Task Force for the ABCDEs of Melanoma; Tsao H, Olazagasti JM, Cordoro KM, Brewer JD, Taylor SC, et al. Early detection of melanoma: Reviewing the ABCDEs. J Am Acad Dermatol. 2015; 72(4):717-23.
2. Antonio JR, Soubhia RMC, D'Avila SCGP, Caldas AC, Trídico LA, Alves FT. Correlation between dermoscopic and histopathological diagnoses of atypical nevi in a dermatology outpatient clinic of the Medical School of São José do Rio Preto, SP. An Bras Dermatol. 2013;88(2):199-203.
3. Rosendahl C, Cameron A, McColl I, Wilkinson D. Dermatoscopy in routine practice - ‘chaos and clues'. Aust Fam Physician. 2012; 41(7):482-7.
4. Ahnlide I, Bjelerupp M, Nilsson F, Nielsen K. Validity of ABCD rule of dermoscopy in clinical practice. Acta Derm Venereol. 2016; 96(3):367-72.
5. Kawamura T. Interpretação de um teste sob a visão epidemiológica: eficiência de um teste. Arq Bras Cardiol. 2002; 79(4):437-41.
6. Carrera C, Marchetti MA, Dusza SW, Argenziano G, Braun RP, Halpern AC, et al. Validity and reliability of dermoscopic criteria used to differentiate Nevi from Melanoma. JAMA Dermatol. 2016; 152(7):798-806.
7. Ahnlide I, Bjelerupp M. Accuracy of clinical skin tumour diagnosis in a dermatological setting. Acta Derm Venereol 2013; 93(3): 305-8.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}