


Brenno Augusto Seabra de Mello Netto1,2; José Marcelo Corassa2; Gustavo Facchini3; Michelle Sabrina da Silva3; Ana Lúcia Tabarini Alves Pinheiro3; Samara Eberlin3
Received on: 08/02/2019
Approved on: 10/06/2019
Study conducted at the Kosmoscience Group, Campinas (SP), Brazil.
Financial support: FQM Farmoquímica S/A.
Conflict of interests: Study sponsored by FQM Farmoquimica S/A, but the methodology, execution and analysis of the results obtained were conducted by the researchers, without any interference from the pharmaceutical industry.
INTRODUCTION: Sclerotherapy is the most widely used method for the treatment of varicose veins of the lower limbs. The most common complication is the appearance of hyperchromic spots in the treated region. Pycnogenol® has long been known as a phlebotonic, anti-inflammatory and skin depigmenting drug. Studies have already proven the efficacy of this drug in the prevention and treatment of post inflammatory hyperpigmentation.
OBJECTIVE: To evaluate the effectiveness of Pinus pinaster extract (Pycnogenol®; PPE) in the prevention of hemosiderin deposits in human skin culture submitted to inflammatory stress.
METHODS: Fragments of human skin were stimulated with interleukin 1 alpha (IL-1 α) to induce an inflammatory response and, concurrently treated with PPE for further histological evaluation and hemosiderin semi-quantification.
RESULTS: The histological evaluation of skin fragments exposed to IL-1 alpha revealed a 26.6% higher hemosiderin density compared with the control group. Moreover, skin fragments incubated concomitantly with PPE showed significant reductions in hemosiderin deposits when compared with the group only exposed to the inflammatory microenvironment.
CONCLUSIONS: The results presented in this study showed an important effect of PPE (Pycnogenol®) in the prevention of hemosiderin accumulation caused by inflammatory stress similar to the post-sclerotherapy process.
Keywords: Hemosiderin; Hyperpigmentation; Sclerotherapy
Chronic venous insufficiency (CVI) is the most prevalent of venous diseases, with national data showing rates ranging from 35% to 50% of the population.1 In the twentieth century, several theories were proposed regarding the etiology and pathophysiology of CVI, with more discussion regarding hypertension secondary to reflux and/or obstruction in the venous system. These abnormalities may present features ranging from telangiectasias to more severe conditions such as phlebitis and ulcers (CEAP C0 to C6).2
Sclerotherapy is the most widely performed treatment in the world for varicose veins in all its stages. Knowledge of the technique and the adverse events of each substance can optimize the results. However, each treatment presents a series of complications, especially when using microfoam for the treatment of larger caliber veins.3
The development of post-sclerotherapy hyperchromic spots may occur due to two main factors: hemosiderin deposition and post-inflammatory pigmentation. Hemosiderin is a pigment found in the dermis that results from the extravasation of red blood cells from treated vessels and also from the inflammatory reaction generated by the excessive presence of iron and the formation of free radicals. This pigment presents an ocher color of difficult removal.4-5 Post-inflammatory hyperpigmentation occurs due to the melanocytic reaction to the presence of metallic ions, such as iron and inflammatory kinins, such as interleukin 1 (IL-1), IL-6, and nuclear transcription factor kappa B (NFkB), especially in patients with higher phototype or melasma.6
Most of these spots progress to spontaneous bleaching in up to six months; however, about 2% of these spots remain for more than a year. The early treatment can favor resolution and prevent its chronification, which generates great anxiety to the patient, who will blame the doctor for the damage caused.7
Pycnogenol® (FQM Famoquímica S/A, Rio de Janeiro, Brazil) is a standardized extract of the bark of the French maritime pine (Pinus pinaster), rich in procyanidins. This substance has proven antioxidant and anti-inflammatory actions, acting in the reduction of lower limb edema, improvement of symptoms related to CVI, reduction of melanogenesis and, consequently, reduction of post-inflammatory hyperpigmentation. 8-9
This study aimed to evaluate the efficacy of a Pinus pinaster (Pycnogenol®) extract in the prevention of hemosiderin deposits in human skin culture submitted to inflammatory stress.
The dry Pinus pinaster extract (PPE) was supplied by the FQM Farmoquímica S/A, Rio de Janeiro, Brazil (Flebon® 50 mg), which contains: Pycnogenol®, corn starch, alpha-cellulose, silica (silicon dioxide), magnesium stearate, sodium carboxymethylcellulose, sodium lauryl sulfate and sodium carboxymethyl starch.
This study used fragments of human skin from a healthy woman, phototype II, 54 years old, who underwent elective plastic surgery in the abdominal region (abdominoplasty). After the surgical procedure, the skin fragments were collected in plastic bottles containing 0.9% saline and kept in refrigeration for up to 24 hours. The fragments were fractionated into approximately 2 cm2 pieces, then weighed, incubated in a 24-well plate (Nunc, Denmark) with DMEM (Dulbecco's Modified Eagle's Medium; Corning, USA) containing glucose, L-glutamine, penicillin, streptomycin and fetal bovine serum (Thermo Fisher Scientific, USA).
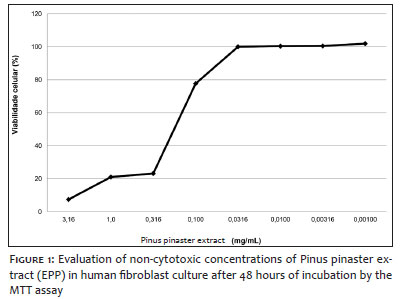
The PPE concentrations assessed in this study were 0.100, 0.0316, and 0.0100 mg/mL, previously determined by the cell viability assay (3-(4,5-Dimethyl-2-thiazolyl)-2,5-diphenyl-2H-tetrazolium bromide). For induction of an inflammatory environment, the cultures were concomitantly stimulated with interleukin-1 alpha (IL-1α; 10 ng/mL; BioLegend, USA) for a period of 48 hours.
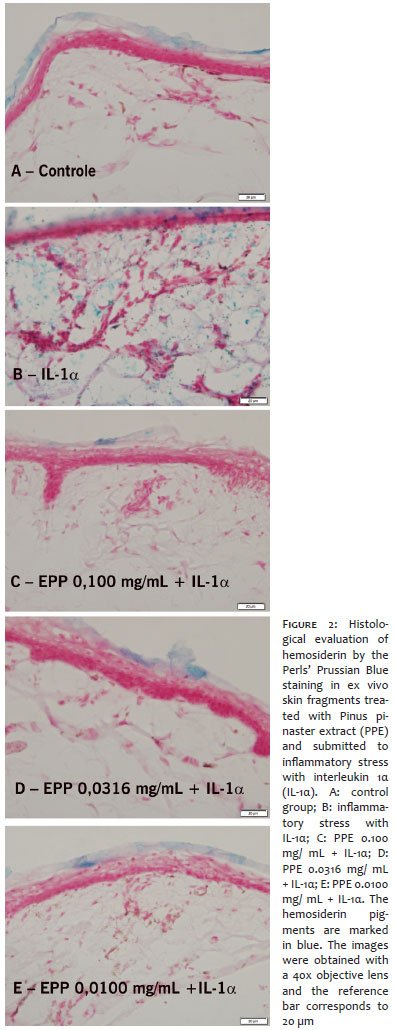
After the treatment and application of inflammatory stress, the skin fragments were fixed in paraformaldehyde for 24 hours and cryoprotected in sucrose solution for 72 hours. Then, serial cuts of 10 µm were collected directly on silanized slides with the aid of Cryostat (Leica Microsystems, Germany) and stained with Perls' Prussian Blue technique.10 For better visualization of the cuts, a counterstaining was performed using an aqueous solution containing 0.1% safranin and 1% glacial acetic acid. The presence of hemosiderin was evaluated under an optical microscope (BX53, Olympus Corporation, Shinjuku, Tokyo, Japan) using the cellSens Standard software (© 2010, Olympus Corporation). After obtaining the images, hemosiderin was semi-quantified (arbitrary units - AU) with ImageJ software (version 1.49V, National Institutes of Health, Bethesda, MD, USA). The images were divided into blue, red and green channels, and blue channel images were binarized for pixel quantification.
The use of fragments of human skin in elective surgeries for this study was approved by the Committee for Ethics in Research of the São Francisco University (SP).
Statistical analysis was performed by ANOVA (GraphPad Prism v6) to measure the variation of the results, comparing the data among all groups. We also applied the Bonferroni post-hoc test, which strengthened and made the results more accurate. Statistical significance was considered as P<0.05. Data were expressed as mean ± standard deviation.
Figure 1 represents the cell viability curve for PPE. The product had non-cytotoxic concentrations from 0.100 mg/mL.
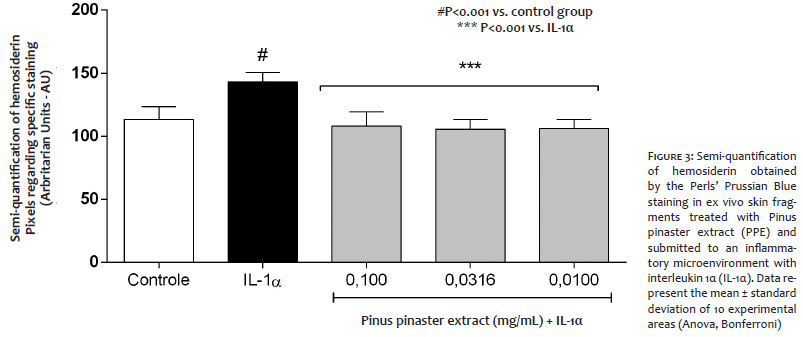
Figure 2 represents the histological evaluation of hemosiderin by the Perls' Prussian Blue technique on fragments of human skin obtained from the elective plastic surgery, incubated with PPE and submitted to IL-1α inflammatory stress. Figure 3 shows the semi-quantification of this pigment. As we can observe, fragments of skin exposed to IL-1α have 26.6% greater hemosiderin density compared with the control group (P<0.001, Figure 3). However, skin fragments incubated with PPE and exposed to the inflammatory microenvironment show significant reductions in hemosiderin deposits when compared with the only group exposed to IL-1α. The observed reductions were 24.55; 26.39 and 25.93%, respectively, at concentrations of 0.100; 0.0316; and 0.0100 mg/mL of PPE (P<0.001; Figure 3).
The choice of the therapeutic method for the treatment of varicose veins should be made based on the degree of affection and the characteristics of the patient, such as skin phototype and the use of concomitant medications, which may predispose or aggravate skin spots. However, once the hyperchromia is installed, the evolution time must be respected, because most of the time a spontaneous resolution occurs within six months. 7
When the outcome is unfavorable, it is common to observe a scenario with some degree of fragility and anguish, since the presence of post-sclerotherapy spots increases the degree of aesthetic expectations and emotional factors. Therefore, during the therapeutic approach to hyperchromia, it is of utmost importance to establish a longitudinal connection with the patient, who will often present a pressing need for outcome. To discuss the duration, indications, and limitations of each proposed method brings clarity and confidence, with greater adherence to the treatment and possibility of satisfactory results. 7
During the sclerotherapy, an endothelial lesion may occur with exposure of subendothelial collagen fibers, causing platelet aggregation and chemotactic factors release. Consequently, vessel thrombosis occurs and the clot formed leads to fibroblast proliferation and fibrotic organization. Cutaneous hematomas originate from the extravasation of blood into the surrounding connective tissue with activation of the inflammatory response and migration of specialized cells to the affected site. The area is first infiltrated with neutrophilic granulocytes and then with macrophages, the latter being responsible for phagocytosis of erythrocyte residues, particularly hemosiderin, which are detected by the specific Perls' Prussian Blue method.10
Preliminary studies conducted by our group demonstrated the effects of Pycnogenol® on the prevention of melanogenesis using fragments of human skin exposed to ultraviolet radiation A and B, infrared radiation A, and visible light, corroborating the bleaching benefit after sun exposure.11 Similar results were observed by Kim (2008), who pointed out that Pycnogenol® has an antimelanogenic effect, inhibiting the activity of the tyrosinase enzyme involved in the production of melanin by mechanisms that encompass free radical suppression and positive regulation in B16 cells.12
Pycnogenol® and its action on microcirculation were exalted by Fitzpatrick et al. (1998) and later by Belcaro et al. (2016). Both authors have demonstrated that the extract causes a significant prevalence of oxygen in the dermis, also reducing the presence of carbon dioxide. They also emphasized the stimulating effect of endothelial function resulting from the prolonged synthesis of endothelial nitric oxide.13-14
Bascones et al. (2006) observed that the treatment of human fibroblasts with 0.100 mg/mL of PPE resulted in the inhibition of damage caused by the oxidative stress. In addition, this extract demonstrated a regulation of the expression of matrix metalloproteinases and the synthesis of pro-collagen type I by inhibition of activating protein 1 (AP-1), a transcription factor that responds to inflammatory stimuli.15
The present study was conducted aiming to assess the effects of the dry Pinus pinaster extract (PPE) on the hemosiderin deposits using an ex vivo model of human skin culture. Histological parameters were investigated in skin explants treated with PPE and stimulated concomitantly with interleukin 1 alpha (IL-1α) for the induction of inflammatory microenvironment.
Our results demonstrated a significant increase in hemosiderin staining in the group exposed only to IL-1α. However, the skin fragments treated with PPE presented hemosiderin staining similar to that observed in the basal control group. Our results are in agreement with data from the literature that report antioxidant and anti-inflammatory actions of the Pinus pinaster extract in in vitro research models.15
To date, no study has demonstrated the activity of Pinus pinaster extract in the cutaneous hemosiderin deposits. Thus, we provide original data on the efficacy of PPE in the prevention of hemosiderin deposits in cultured human skin submitted to inflammatory stress, similar to the environment created after sclerotherapy.
The results presented in this study point to an important effect of the Pinus pinaster extract (Pycnogenol®) in the prevention of hemosiderin accumulation originated by inflammatory stress similar to the post-sclerotherapy process. Although additional studies are required to prove the prophylactic activity in local hyperpigmentation, the use of the Pinus pinaster extract (Pycnogenol®) can be considered as a promising option, differentiating it from the other substances currently available.
Brenno Augusto Seabra de Mello Netto | ORCID 0000-0002-0345-4126
Critical review of the literature.
José Marcelo Corassa | ORCID 0000-0002-8732-888X
Intellectual participation in propaedeutics and/or therapeutics in the cases studied, critical review of the literature.
Gustavo Facchini | ORCID 0000-0003-0111-7596
Statistical analysis, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation.
Michelle Sabrina da Silva | ORCID 0000-0001-6684-970X
Data collection, analysis and interpretation.
Ana Lúcia Tabarini Alves Pinheiro | ORCID 0000-0002-0226-2544
Design and planning of the study.
Samara Eberlin | ORCID 0000-0001-7001-801X
Statistical analysis, design and planning of the study, preparation and writing of the Manuscript, critical review of the original.
1. Maffei FHA, Magaldi C, Pinho SZ, Lastoria S, Pinho W, Yoshida WB, et al. Varicose veis and chronic venous insufficiency in Brazil: prevalence among 1755 inhabitants of a country town. Int J Epidemiol. 1986;15(2):210-7.
2. Beebe HG, Bergan JJ, Bergqvist D, Eklof B, Eriksson I, Goldman MP, et al. Classification and grading of chronic venous disease in the lower limbs: a consensus statement. Vasc Surg. 1996; 30:5-11.
3. Palm MD, Guiha IC, Goldman MP. Foam sclerotherapy for reticular veins and nontruncal varicose veins of the legs: a retrospective review of outcomes and adverse effects. Dermatol Surg. 2010;36(Suppl 2):1026-33.
4. Thibault PK, Wlodarczyk J. Correlation of serum ferritin levels and postsclerotherapy pigmentation. A prospective study. J Dermatol Surg Oncol. 1994;20(10):684-86.
5. Scott C, Seiger E. Postsclerotherapy pigmentation. Is serum ferritin level na accurate indicator? Dermatol Surg. 1997;23(4):281-82.
6. Nordlund JJ. Postinflammatory hyperpigmentation. Dermatol Clin. 1988;6(2):185-92.
7. Goldman MP. Complications and adverse sequelae of sclerotherapy. In: Bergan JJ, editor. The Vein Book. Rio de Janeiro: Elsevier, 2007. p.139-155.
8. D'Andrea G. Pycnogenol: A blend of procyanidins with multifaceted therapeutic applications? Fitoterapia. 2010;81(7):724-36.
9. Ni Z, Mu Y, Gulati O. Treatment of melasma with Pycnogenol. Phytoter Res. 2002;16:567-71.
10. Kostadinova-Petrova I, Mitevska E, Janeska B. Histological Characteristics of Bruises with Different Age. Maced J Med Sci. 2017;5(7):813-7
11. Ayres EL, Costa A, Eberlin S, Cleric SP. Ex vivo study for evaluating the whitening activity of Pycnogenol® after exposure to ultraviolet and infrared radiations, and visible lights. Surg Cosm Dermatol. 2015;7(4):303-7.
12. Kim YJ, Kang KS, Yokozawa T. The anti-melanogenic effect of pycnogenol by its anti-oxidative actions. Food Chem Toxicol. 2008;46(7)2466-71.
13. Fitzpatrick DF, Bing B, Rohdewald P. Endothelium-dependent vascular effects of Pycnogenol. J Cardiovasc Pharmacol. 1998;32(4):509-15.
14. Belcaro G, Cesarone MR, Errichi BM, Ledda A, Di Renzo A, Stuard S, et al. Diabetic ulcers: microcirculatory improvement and faster healing with Pycnogenol. Clin Appl Thromb Hemost. 2006;12(3):318-23.
15. Jung H-Y, Shin J-C, Park S-M, Kim N-R, Kwak W, Choi B-H. Pinus densiflora extract protects human skin fibroblasts against UVB-induced photoaging by inhibiting the expression of MMPs and increasing type I procollagen expression. Toxicol Reports. 2014;1:658-66.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}