


Rodolfo Ferreira Mendonça1; Lyvia Almeida Nascimento Salem1; Renata Oliveira Alves1; Bomi Hong1; Rute Facchini Lellis2; Elisete Isabel Crocco3
Received on: 20/01/2018
Approved on: 22/10/2018
This study was performed at the Dermatology Service, Santa Casa de São Paulo, São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
This study demonstrated the clinical and histologic result of the treatment of one disseminated superficial actinic porokeratosis patient with non-ablative fractional laser. The patient was treated with seven sessions of 1340-nm Nd:YAP laser, with 4 or 5 week-intervals. Biopsies and photographs were performed before and after treatment, which was well tolerated and lead to improvement in the erythema and texture of the lesions. There was a 1-year follow-up. Histopathologic examination after treatment revealed little changes in the cornoid lamella.
Keywords: Biopsy; Laser Therapy; Lasers; Porokeratosis
Disseminated superficial actinic porokeratosis (DSAP) is a clonal proliferation of aberrant keratinocytes1 that clinically arises as papules and erythematous or hyperchromic plaques with thin elevated borders in photoexposed body sites. 2 Ultraviolet radiation, immunosuppression and genetic factors are likely to contribute to its pathogenesis.3
Follow-up of these patients is necessary due to the potential malignant progression of the lesions. For symptomatic cases, there are a number of therapeutic options, such as diclofenac, calcipotriol, 5-fluoracil, imiquimod, topical and systemic retinoids, phototherapy and laser (CO2: Er:YAG, Q-switched ruby, Q-switched Nd: 1,550nm YAG; erbium-doped, or 1,927nm thulium).4-7
Two case reports5,6 evidenced clinical improvement of DSAP after treatment with fractional laser. Nevertheless, histological follow-up was not carried out. The present article describes both the clinical and histological follow-up of a DSAP case treated with 1,340 nm Nd:YAP (Neodimiun:Ytrium Aluminum Perovskite) laser, which has water as its target.
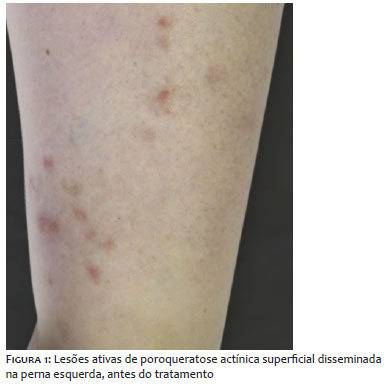
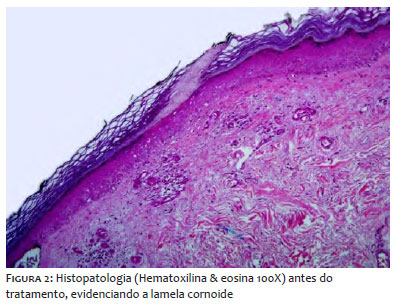
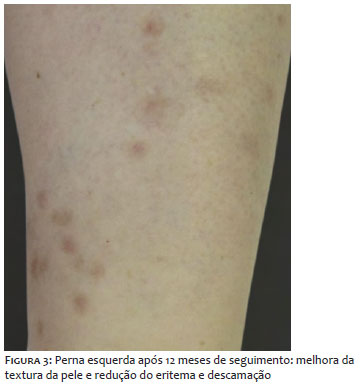
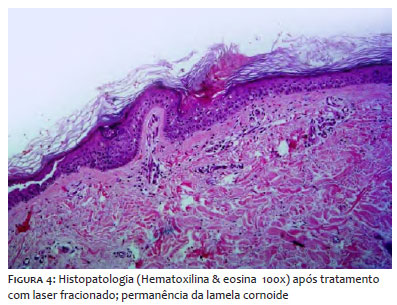
A 61-year-old woman (Fitzpatrick skin phototype II) presented erythematous-hyperchromic papules and annular plaques measuring from 3 to 12 mm, with thin hyperkeratotic borders, predominating in the legs and sparse in photoexposed areas of the thorax and forearms (Figure 1). The lesions emerged 20 years before, having been worsened in the past previous years. The patient denied pain or pruritus. The patient's mother had similar lesions and multiple cutaneous neoplasias. Histological examination revealed cornoid lamella and hypogranulosis, confirming the diagnosis of disseminated superficial actinic porokeratosis (Figure 2). After therapeutic failure with topical 0.5mg/g tretinoin in dermatological cream on alternate days for four months, the patient underwent seven 1,340 nm Nd:YAP laser sessions (Etherea®, Industra Technologies, São Carlos, SP, Brazil ), with intervals of four to five weeks. Four passes per session were performed with 100mJ / MTZ, 3ms pulse duration, 100MTZ / cm2 density and 8mm tip. Tolerance to treatment was excellent. Although new lesions have emerged during the treatment, the patient and the medical team noticed improvement of erythema and cutaneous texture after 12 months of follow-up (Figure 3). Nonetheless, after seven sessions (eight months), the anatomopathological evidenced the presence of the cornoid lamella (Figure 4).
Fractional lasers produce microscopic treatment zones, sparing the tissue that surrounds the treated column. The non-ablative property of 1,340nm laser generates fewer complications and a shorter recovery time as compared to ablative lasers. However, there is absence of literature comparing ablative and non-ablative fractional lasers in the treatment of DSAP.
Just as in other case reports where lesions were treated with non-ablative fractional laser (1,550nm and 1,927nm),5,6 the patient was satisfied with the improvement of the treated lesions, with absence of pain or complications, except for mild erythema. Nevertheless, the intervention did not prevent the occurrence of new lesions – which continued to increase in number despite the clinical improvement.
Biopsies performed before and after treatment revealed a similar corneal lamella, hypogranulosis, and dyskeratosis. This fact does not confirm the possibility that fractional laser is capable of reducing the risk of DSAP malignant transformation, of DSAP, emphasizing the importance of the clinical follow-up.
The literature data offer a variety of therapeutic proposals with limited results for DSAP, a pathology that may bring possible risks to patients. In this way, the use of technologies becomes a potential alternative.
Despite the fact that the histologic picture did not change, treatment with 1,340nm fractional laser was proven as a well-tolerated therapeutic option for cosmetic improvement of DSAP.
Rodolfo Ferreira Mendonça | ORCID 0000-0003-3429-0897
Preparation of the manuscript, photographs and case follow-up.
Lyvia Almeida Nascimento Salem | ORCID 0000-0002-4277-6021
Preparation of the manuscript, photographs and case follow-up.
Renata Oliveira Alves | ORCID 0000-0001-6441-4091
Laser applications.
Bomi Hong | ORCID 0000-0003-1656-601X
Laser applications.
Rute Facchini Lellis | ORCID 0000-0001-7690-0513
Anatomopathological study and evaluation.
Elisete Isabel Crocco | ORCID 0000-0002-8844-2887
Preparation of the manuscript, case follow-up, therapeutics guidance and general supervision.
1. Reed RJ, Leone P. Porokeratosis - a mutant clonal keratosis of the epidermis. I. Histogenesis. Arch Dermatol. 1970;101(3):340-7.
2. Gupta G, Madan V, Lear JT. Squamous Cell Carcinoma and its Precursors. In: Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook's Textbook of Dermatology. Malden, Mass: Wiley; 2016. p. 1-46
3. Murase J, Gilliam AC. Disseminated superficial actinic porokeratosis co-existing with linear and verrucous porokeratosis in an elderly woman: Update on the genetics and clinical expression of porokeratosis. J Am Acad Dermatol. 2010;63(5):886-91.
4. Skupsky H, Skupsky J, Goldenberg G. Disseminated superficial actinic porokeratosis: a treatment review. J Dermatolog Treat. 2012;23(1):52-6.
5. Chrastil B, Glaich AS, Goldberg LH, Friedman PM. Fractional photothermolysis: a novel treatment for disseminated superficial actinic porokeratosis. Arch Dermatol. 2007;143(11):1450-2.
6. Ross NA, Rosenbaum LE, Saedi N, Arndt KA, Dover JS. Disseminated superficial actinic porokeratosis improved with fractional 1927-nm laser treatments. J Cosmet Laser Ther. 2016;18(1):53-5.
7. Aird GA, Sitenga JL, Nguyen AH, Vaudreuil A, Huerter CJ. Light and laser treatment modalities for disseminated superficial actinic porokeratosis: a systematic review. Lasers Med Sci. 2017;32(4):945-52.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}