


Luiza Helena Urso Pitassi1; Célia Luiza Petersen Vitello Kalil2; Clarissa Prieto Herman Reinehr3; Valéria Barreto Campos4; Christine Chaves5; Stela Cignachi6
Received on: 13/11/2018
Approved on: 22/12/2018
Study conducted at the institution: 1. Clínica Célia Kalil - Porto Alegre, RS Brazil 2. Clínica Valéria Campos - Jundiaí, SP Brazil
Financial support: None
Conflict of interests: None
INTRODUCTION: The chest is a photoexposed area that shows effects of photodamage. Microneedling is a safe option for the rejuvenation of this area, also leading to improvement in dyschromias.
OBJECTIVE: To evaluate histologic cutaneous response after three monthly sessions of microneedling for the treatment of dyschromias on the chest.
METHODS: Three monthly sessions of microneedling, with 1.5mm length needles were performed, as well as skin biopsies before and 90 days after commencement of the study. Histologic samples were evaluated with H&E and Fontana-Masson stains. Melanin content was measured based on dermal clusters.
RESULTS: Six patients between 38 and 67 years of age, phototypes II-III, Glogau scale II-IV were included. A positive correlation was observed between the time and dermal content of melanin (p=0.029): three sessions of microneedling reduced this content on D90 compared to the beginning (6.4 ± 1.7 MC on D0 versus 3.1 ± 0.4 on D90, p = 0.05). Three patients reported global skin improvement on D90.
CONCLUSIONS: The proposed mechanism of microneedling to promote lightening includes fibroblast proliferation and neocollagenesis in the upper dermis. This is the first study to evaluate the histology of the findings associated to lightening of the chest due to microneedling.
Keywords: Histology; Melanins; Needles; Thorax
The chest is an area that can reveal skin ageing, since it is exposed to the sun and is frequently left untreated.1 The aspect of photodamaged skin in this region, that shows skin laxity, dyspigmentation, xerosis, wrinkles, freckles and poikiloderma leads to the patient's aesthetic dissatisfaction, who looks for effective, safe treatment options, with the shorter downtime possible.1 In this context, the use of microneedling associated to drug delivery has been demonstrated as an effective and safe treatment, amongst the available therapeutic arsenal.
In a previous study, the authors observed positive clinical results in the overall rejuvenation of the chest with three sessions of microneedling and drug delivery, with significant improvement in the skin's texture and firmness. Besides, clinical improvement in dyspigmentation, with lightening of the treated area and achievement of even skin color was observed.2
The lightening effect of the technique of microneedling associated to drug delivery is described in patients with refractory melasma treated with the technique alone or associated to topical lightening agents in drug delivery, such as tranexamic acid, hydroquinone, rucinol, sophora-alpha and ascorbic acid.3-7 Additional studies associating the lightening effect of microneedling for the treatment of the chest were not found in the literature, highlighting the need of further studies that substantiate those findings.
In this context, this study aims to evaluate the histological response observed in the skin after treatment of dyspigmentation in the region of the chest with microneedling.
The present study aims to evaluate histologically the procedure of skin microneedling on the region of the chest. The patients were evaluated before the procedure (D0) and after three monthly sessions (D90).
The study was set up according to good quality procedures and knowledge of the participants, who signed a consent form, the patients were randomly included in the study. The exclusion criteria involved past history of keloid scar, use of isotretinoin, treatment with steroids or anticoagulants, collagen vascular disease, presence of skin infection in the treatment area, skin cancer, warts and pregnancy. Besides, patients were advised to discontinue medications and/or herbal products that could affect blood coagulation, such as aspirin, vitamin E, gingko biloba, garlic capsules, ginseng and ginger for at least 3 days before each procedure of microneedling.
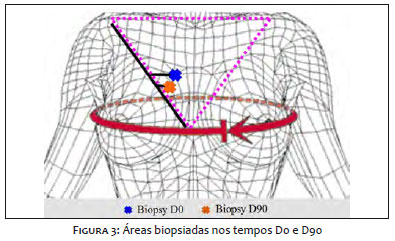
As preparation for the procedure of microneedling, the participants were submitted to marking of the chest area shaped as an inverted triangle, where the line of the base of the triangle has as reference points the external aspect of the right and left clavicles, and the top of the triangle converges to the intermammillary center, delineating the area of the procedure (Figure 1).
After marking, the region to be treated with microneedling was prepared with topical anesthetic (lidocaine gel 23% and tetracaine 7%) one hour prior to the procedure. With the region anesthetized, the gel was removed with 0.2% chlorhexidine solution and a qualified dermatologist performed the procedure of microneedling with the device Dr. Roller® (Anvisa registration/MS: 80669600001, imported and distributed by the company MTO), a medical device made of 192 0.07mm-width and 1.5mm-length surgical steel microneedles arranged in a cylinder (Figure 2). The application technique consists in, with one of the hands, positioning it in a 45º angle over the area to be treated and, with minimal pressure, performing 10 movements in four direction: horizontal, vertical, right diagonal and left diagonal. Rolling the device leads to penetration of the needles many times in the skin, causing microlesions that allow for the release of growth factors and, therefore tissue remodeling.
Immediately after the procedure, the skin was cleaned with 0.9% saline. The participants were instructed to clean the area daily with soap and apply a complementary product with mineral (inorganic) sunscreen SPF30/PPD 11.7 straight away, zinc oxide and silicone based.
With the aim of evaluating microscopic changes induced by microneedling, biopsies of the region treated were obtained with 4mm punches, of each of the 6 patients before and three months after starting treatment. Both areas biopsied on D0 and D90 were located 1cm medially to the middle third of the right side of the inverted triangle and 0.5cm away from the previous biopsy (Figure 3). (Figure 2). Finalizing the procedure, the skin was sutured with Mononylon 5-0 suture.
The skin samples collected on D0 and D90 were fixated in 10% formaldehyde solution and incorporated into paraffin. They then underwent histological cuts of 3µm and were processed using the universal staining hematoxylin-eosin (HE). In the histological slides, inflammatory and actinic lesions were excluded, and the quantity and distribution of melanin were identified in an imprecise manner.
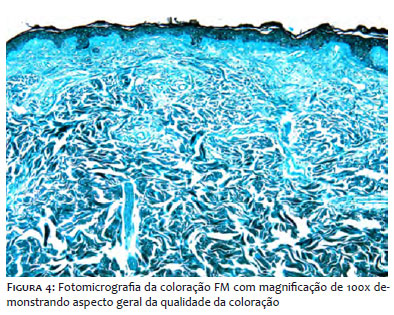
The histochemical reaction of Fontana-Masson (FM) was also performed, which is specific for the identification of melanin, naturally showing a tan/brown coloration, but as showing black with this reaction, which makes its identification easier. With the aim of demonstrating the overall aspect of the quality of the staining, photomicrography of the FM staining was performed with 100x magnification (Figure 4).
The FM reaction allowed for the categorization of the distribution and the amount of melanin in the skin's microarchitecture. Regarding distribution, two compartments were considered: papillary dermis and reticular dermis. To obtain the amount of melanin, the amount of melanin clusters was considered (MC) distributed along the dermis. For counting the MC, microscopic fields with 400x magnification were used (HPF, high power fields). For final identification of the amount of MC in each sample, the mean MC/HPF was considered. Therefore, the global mean papillary and reticular of MC/HPF in groups D0 and D90 was determined.
The subjective evaluation was performed through a structured questionnaire individually answered by all patients on D30 and D90, based on their perception of the treated area regarding the following aspects: texture, wrinkles, color, shine, smoothness, firmness and overall appearance. The answers were classified into 4 scales regarding the improvement in the skin of the area treated: 1 – none; 2 – little; 3 – a lot; 4 – very much. Besides, it was also informed if the patient noticed 'any improvement with the treatment' and the answers were classified as: 1 – no; 2 – yes.
Data were analyzed using the statistical software SPSS version 21, IBM Corporation. Quantitative variables were compared between D0 (before) and D90 (after) by GEE and post hoc comparison of Bonferroni. To evaluate differences in qualitative variables, Fisher's exact test was performed. P < 0.05 was considered statistically significant.
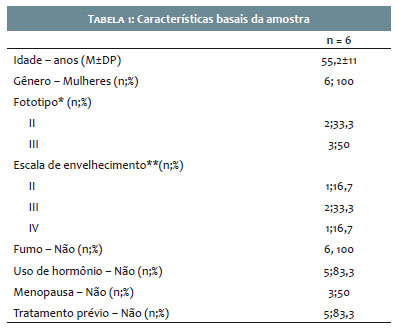
Six healthy Caucasian patients, with ages between 38 and 67 years, Fitzpatrick phototype II and III, and Glogau ageing scale between II and IV participated in the study (Table 1).
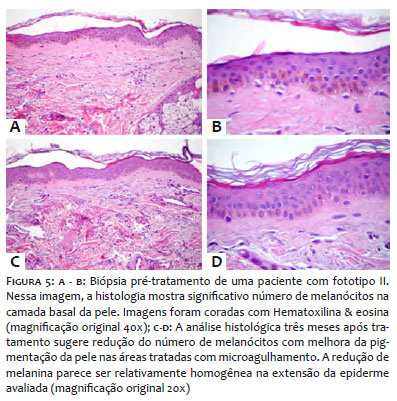
There was significant interaction between the effect of time and the type of dermis (p = 0.029), therefore, it was verified that three sessions of microneedling (D90) tend to reduce the mean melanin clusters (MC) in the reticular dermis in comparison to the baseline mean (D0) (6.4 ± 1.7 went down to 3,.1 ± 0.4, p = 0.05). Figure 5 shows histological images before (D0) and after (D90) treatment. There was no statistically significant difference regarding MC means in the papillary dermis in the two intervals (p = 0.47).
Of the six patients, three reported improvement of the skin on D90; however, this improvement was not statistically significant (p = 0.256) when compared to the results on D30. Two patients did not observe improvements on the area with treatment on D90 and one did not complete the questionnaire at the end of the study.
Three patients showed some kind of symptoms on the region soon after treatment with the roller, among them: erythema, erythema with burning sensation and excessive skin dryness with mild burning sensation.
Procedures that stimulate regenerative mechanisms of the body and activate injury healing in the treated skin without wound formation has been the focus of clinical research for a variety of skin conditions. The use of microneedles for percutaneous induction of collagen arises from microinjuries that reach the papillary and reticular dermis; to reach the dermis it is necessary a minimum length of the needles of 1.5mm.8 As final result, there is partial disruption of the skin barrier, and cytokines are released, as interleukin-1-alpha, interleukin-8, interleukin-6, TNF-alpha e GM-SCF. Five days after the injury, a fibronectin matrix is formed, and the deposition of collagen is initiated, initially composed of type III collagen, subsequently replaced by type I collagen.8,9
El-Domyati et al.10 studied the effect of microneedling with 1mm needles for facial rejuvenation in 10 patients submitted to 6 sessions of microneedling every 2 weeks, observing clinical improvement in skin ageing with correspondent histological improvement: statistically significant (p < 0.05) increase in epidermal thickening with better formation of the papillary dermis.10 After the sessions, the patients presented erythema and edema, that settled over two days.10
Results of another study, in which 22 patients with refractory melasma, unresponsive to topical bleaching agents and sunscreen were treated with two sessions of microneedling every 30 days, demonstrating that 100% of patients reported satisfaction with the area treated after the end of the treatment protocol.4 The author concluded that microneedling with 1.5mm length needles can lighten skin blotches in patients with refractory melasma and that the use of skin bleaching agents and e sunscreen is mandatory after the procedure.4 Another study by the same author conducted two monthly sessions of microneedling in six women with refractory facial melasma.7 The study demonstrated improvement of melasma in all patients, and histological analyses showed epithelial thickening, reduction of epithelial melanin pigmentation and densification of collagen in the upper dermis. The mechanism of action proposed, by which microneedling promotes improvement of hyperpigmentation such as melasma, includes fibroblast proliferation and neocollagenesis in the upper portion of the dermis.7 These events would restore the damage to the basement membrane and in the upper portion of the dermis, avoiding the contact of melanocytes with dermal melanogenic stimuli.11,12 Besides, once microneedling causes epidermal thickening, the procedure would promote an additional protection to UV radiation.7
Until now, evidence-based treatment protocols for microneedling are not available.13 However, microneedling is a safe option for the treatment of scars and wrinkles.13 Besides, its effects reach a maximum benefit between eight and 24 weeks, with variations observed between the authors.14,15
In a recent study, 12 patients were treated with three sessions of microneedle radiofrequency (Endymed Intensif, EndyMed Ltd., Cesarea, Israel) for rejuvenation of the chest region, performed every three weeks; clinical evaluation by two blinded dermatologists using the Global Aesthetic Improvement Scale demonstrated that 67% of the patients treated showed global improvement of the area, what included improvement in wrinkles, skin texture and firmness.16 Clinical information regarding improvement of dyspigmentation in the treated area were not mentioned by the authors.
This study endorses the literature particularly regarding the significant reduction in melanin clusters in the dermis with improved pigmentation of the skin treated with microneedling. Despite other parameters tested not showing statistical significance, the data are clinically relevant so that other studies with a larger sample can be conducted, with the aim to confirm the efficacy of this treatment. We acknowledge the small sample size as an important limitation of this study, as well as the number of treatment sessions. We identify the need for future studies with larger samples that can better represent a longer follow-up period so that it is possible to create and establish international treatment protocols for microneedling.
Microneedling has been shown as a minimally invasive treatment to promote clinical and histological improvement of melasma. Histological results obtained in this study support what was previously described in the literature and are promising regarding the efficacy of the treatment.
Luiza Helena Urso Pitassi | ORCID 0000-0001-6646-4391
Statistical analysis, approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, active participation in the mentoring of the research, intellectual participation in propaedeutics and/or therapeutics of the cases studied, critical review of the literature, critical review of the original.
Célia Luiza Petersen Vitello Kalil | ORCID 0000-0002-1294-547x
Approval of the final version of the original, design and planning of the study, data collection, analysis and interpretation, active participation in the mentoring of the research, intellectual participation in propaedeutics and/or therapeutics of the cases studied, critical review of the literature, critical review of the manuscript.
Clarissa Prieto Herman Reinehr | ORCID 0000-0003-1811-4519
Approval of the final version of the original, design and planning of the study, preparation and writing of the manuscript, , intellectual participation in propaedeutics and/or therapeutics of the cases studied, critical review of the literature, critical review of the manuscript.
Valéria Barreto Campos | ORCID 0000-0002-3350-8586
Approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, active participation in the mentoring of the research, intellectual participation in propaedeutics and/or therapeutics of the cases studied, critical review of the original.
Christine Chaves | ORCID 0000-0001-8861-6499
Statistical analysis, approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, active participation in the mentoring of the research, intellectual participation in propaedeutics and/or therapeutics of the cases studied, critical review of the literature, critical review of the original.
Stela Cignachi | ORCID 0000-0003-3667-3197
Approval of the final version of the original, design and planning of the study, data collection, analysis and interpretation, intellectual participation in propaedeutics and/or therapeutics of the cases studied.
1. Montagna W, Carlisle K. Structural changes in ageing skin. Br J Dermatol. 1990;122(SUPPL 35):61-70.
2. Kalil CLPV, Campos VB, Chaves CRP, Pitassi LHU, Cignach S. Comparative, randomized, double-blind study of microneedling associated with drug delivery for rejuvenating the skin of the anterior thorax region. Surg Cosmet Dermatol. 2015;7(3):211-6.
3. Budamakuntla L, Loganathan E, Suresh D, Shanmugam S, Suryanarayan S, Dongare A, et al. A randomised, open-label, comparative study of tranexamic acid microinjections and tranexamic acid with microneedling in patients with melasma. J Cutan Aesthetic Surg. 2013;6(3):139-43.
4. Lima E de A. Microneedling in facial recalcitrant melasma: report of a series of 22 cases. An Bras Dermatol. 2015;90(6):919-21.
5. Fabbrocini G, De Vita V, Fardella N, Pastore F, Annunziata MC, Mauriello MC, et al. Skin Needling to Enhance Depigmenting Serum Penetration in the Treatment of Melasma. Plast Surg Int. 2011;2011:158241.
6. Ustuner P, Balevi A, Ozdemir M. A split-face, investigator-blinded comparative study on the efficacy and safety of Q-switched Nd:YAG laser plus microneedling with vitamin C versus Q-switched Nd:YAG laser for the treatment of recalcitrant melasma. J Cosmet Laser Ther. 2017;19(7):383-90.
7. Lima EVA, Lima MMDA, Paixão MP, Miot HA. Assessment of the effects of skin microneedling as adjuvant therapy for facial melasma: a pilot study. BMC Dermatol. 2017;17(1):14.
8. Lima EVA, Lima MA, Takano D. Microneedling experimental study and classification of the resulting injury. Surg Cosmet Dermatol. 2013;5(2):110-4.
9. Kalluri H, Kolli CS, Banga AK. Characterization of Microchannels Created by Metal Microneedles: Formation and Closure. AAPS J. 2011;13(3):473- 81.
10. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahany H, Farag H. Multiple microneedling sessions for minimally invasive facial rejuvenation: an objective assessment. Int J Dermatol. 2015;54(12):1361-9.
11. Tamega A de A, Miot HA, Moço NP, Silva MG, Marques ME, Miot LD. Gene and protein expression of oestrogen- β and progesterone receptors in facial melasma and adjacent healthy skin in women. Int J Cosmet Sci. 2015;37(2):222-8.
12. Lee DJ, Park K-C, Ortonne JP, Kang HY. Pendulous melanocytes: a characteristic feature of melasma and how it may occur: Correspondence. Br J Dermatol. 2012;166(3):684-6.
13. Ramaut L, Hoeksema H, Pirayesh A, Stillaert F, Monstrey S. Microneedling: Where do we stand now? A systematic review of the literature. J Plast Reconstr Aesthet Surg. 2018;71(1):1-14.
14. Fabbrocini G, De Vita V, Monfrecola A, De Padova MP, Brazzine B, Teixeira F, et al. Percutaneous collagen induction: an effective and safe treatment for post-acne scarring in different skin phototypes. J Dermatol Treat. 2014;25(2):147-52.
15. Fabbrocini G, De Vita V, Pastore F, Annunziata MC, Cacciapuoti S, Monfrecola A, et al. Collagen induction therapy for the treatment of upper lip wrinkles. J Dermatol Treat. 2012;23(2):144-52.
16. Lyons A, Roy J, Herrmann J, Chipps L. Treatment of Décolletage Photoaging With Fractional Microneedling Radiofrequency. J Drugs Dermatol. 2018;17(1):74-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}