


Ada Regina Trindade de Almeida; Jaqueline Guerra; Marcelo Margarido Bellini; Alessandra Ribeiro Romiti; Maria Victoria Súarez Restrepo
Received on: 20/02/2019
Approved on: 15/03/2019
Study conducted at the Outpatient Department of Dermatology, Hospital do Servidor Público Municipal de São Paulo (HSPM-SP) - São Paulo (SP), Brazil
Financial support: None
Conflict of interests: None
INTRODUCTION: Hidrocystomas are skin-colored or translucent cysts, single or multiple, appearing on the face. They originate in the eccrine or apocrine sweat gland and are sometimes disfiguring. They can be excised by surgery, electrodissection, or by caustics, but are usually recurrent and the treatments can leave scars or dyschromia. Botulinum toxin A (BoNT-A) has been suggested as therapy in few cases in the literature.
OBJECTIVE: To analyze the effects of BoNT-A in cases of facial hidrocystomas.
METHODS: Retrospective observational study of case series. Patients with facial hidrocystomas treated with BoNT-A at the Cosmiatry Outpatient Dermatology Clinic of the Hospital do Servidor Público Municipal de São Paulo, were evaluated.
RESULTS: Of the 13 patients evaluated, 5 were included, the largest case series described so far. Of these, all lesions treated showed clinical improvement during the period evaluated. Four patients showed partial regression and one, total regression of the lesions.
CONCLUSION: In this series of cases, BoNT-A showed positive and long-lasting results in the treatment of facial hidrocytsomas, with no adverse effects.
Keywords: Botulinum toxins; Hidrocystoma; Therapeutics
Hidrocystomas are translucid or skin-colored cystic lesions, common on the face, particularly around the eyes. They arise from sweat glands, and can be eccrine or apocrine in origin.1 They are benign, single or multiple, relatively common and more frequent in middle-aged women.2
The cause for the appearance is still unclear. Occlusion or blockage of the sweat duct, resulting in sweat retention and consequent dilation of the cystic duct could be one of the possible causes.2,3 Some authors suggest that hot and humid environments could increase sweat production and act as aggravating factors.4,5
Clinically, they appear as one or more lesions of various sizes on the cephalic segment, preferentially on the forehead, malar and palpebral regions, being the external aspect of the lower eyelid the most common site.6
On histology, two different types can be seen: apocrine (or Moll's gland cyst) and eccrine, however, clinical differentiation is rarely made, except by the fact that Moll's gland cyst is solitary and preferentially located near the eyelashes and the tear drainage duct and eccrine hidrocystoma is located on the eyelid skin and can be single or multiple.7 They can still be associated to ectodermal dysplasia syndromes such as Schopf-Schulz-Passarge and Gorlin-Goltz.6-9
In the literature, multiple treatments are mentioned such as surgical excision, simple drainage with a needle, caustics as trichloroacetic acid or phenol, carbon dioxide laser and electrodessication.10 Due to the recurrent nature of the lesions, the risk of unsightly scars and/or dyspigmentation with surgical or ablative procedures is high.
Eccrine sweat glands are innervated by postganglionic sympathetic nerve fibers and regulated by mediators such as acetylcholine, pilocarpine and adrenaline, whereas apocrine glands are mediated by adrenaline, noradrenaline and methacholine.11 All these mediators can be blocked by botulinum toxin. For this reason, the neuromodulator arose as a therapeutic option, having the advantages of being non-invasive, not presenting risks for residual scarring or dyspigmentation.
BoNT-A is still little used for hidrocystomas as a therapeutic option. The application technique consists in the emptying of the cyst content of the lesion, immediately before the local injection of the drug, with the goal of blocking the stimulus to the production of sweat by sweat glands.12,13 The dose injected into each lesion is still not standardized and the duration of the effect produced by the toxin is still unclear.
The procedure is simple, well tolerated, with good course after the procedure, and has no risk of scarring.13 Pain is a transient adverse effect, usually present only during the injection. Headaches, nausea, palpebral ptosis and facial asymmetry are uncommon adverse effects.2
The objective of this study is to retrospectively analyze the efficacy and safety of cases of facial hidrocystomas treated with BoNT-A.
Retrospective observational study of case series. Patients with facial hidrocystomas were selected from the Sector of Cosmiatry of the Outpatient Department of Dermatology of the Hospital do Servidor Público Municipal, treated with botulinum toxin between January 2014 and December 2015.
Inclusion criteria: Patients from both genders, between 18 and 80 years of age, with at least one hidrocystoma on the face treated with BoNT-A and with clinical and photographic follow-up on the day of the application of the neuromodulator (D0) and 14 (D14), 30 (D30), and between 90 and 120 days (D90 and D120) after the procedure.
Variables analyzed: Demographic data (age and gender of the patient), location and number of lesions (single or multiple), dose (per lesion and total), number of sessions performed and efficacy of the therapy applied. The evaluation of the clinical response to the treatment was performed by an observer not involved in the treatment, through photographic records as follows:
Complete regression of the lesions; disappearance of the lesions;
Partial regression of the lesions: reduction in the size of the lesions and/or the number of lesions;
No response: unchanged lesions.
Adverse events: the identification of adverse events was performed through data obtained by reviewing the medical records.
Statistical analysis: Because it is a retrospective observational study, statistical analysis was performed through the description of the findings reported in the medical records.
Thirteen individuals with hidrocystomas on the face treated with BoNT-A were selected in this study. Of these, only five fulfilled the inclusion criteria. The age ranged between 45 and 73 years, the mean being 57.8 years. Four cases were in females (80%) and the phototype ranged from I to VI, with the latter being the most common (40% of the sample). Data on family history of facial hidrocystomas were not found in the medical records analyzed. Most cases (60%) presented a single lesion, and the most common location was on the lateral aspect of the lower eyelid, followed by ocular epicanthus. Histologic differentiation between eccrine and apocrine hidrocystomas was not made.
Botulinum toxin A was reconstituted with 2ml of saline for each vial with 100U. the total dose used in each patient ranged from 5U to 33U, two patients (2 and 4) were treated in only one session, while in three (1, 3 and 5) the second session took place between 15 to 30 days after the first (Table 1).
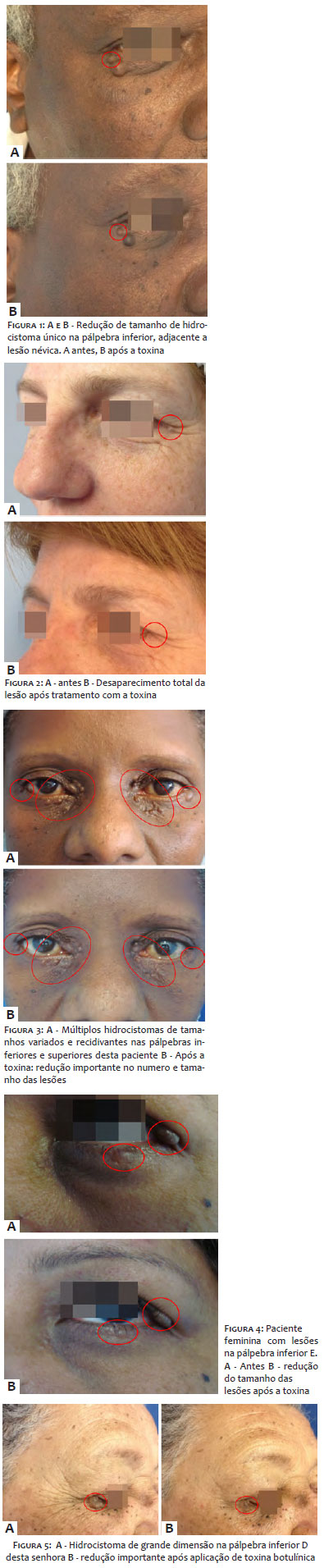
At the end of the 120 days of follow-up, all patients showed some degree of clinical improvement. Complete regression of the lesions occurred in one case (2), and partial regression (reduction in size and/or number of lesions) was seen in four patients (80%), as seen on the corresponding figures (Figures 1A and 1B up to 5A and 5B).
According to Correia et al2, hidrocystoma is more common in middle-aged women, epidemiology consistent with the patients in this study.
The clinical picture can be composed by single or multiple lesions.6 In this sample, single and multiple lesions were found, however, most cases (three) had a single lesion. The most frequent location was on the lower eyelids, mainly in the external aspect, which is in accordance with the findings by Couto Junior et al1 and Yaghoobi et al.6 Of the five patients studied, all had at least one lesion located on the lower eyelid.
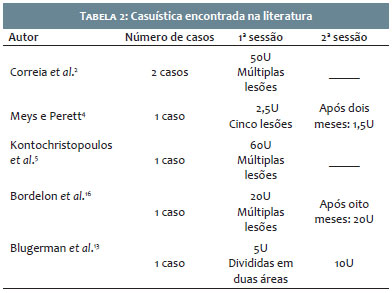
Despite the small number, our case series was larger than the articles on hidrocystoma treated with BoNT-A found in the literature. Of the 13 cases treated, only five were included for fulfilling the inclusion criteria, whereas except by Correia et al2, who reported their experience with two patients, most articles report only one case treated with this method.4,5,12,13
Due to the lack of consensus regarding the dose to be applied, the patients did not receive standardized doses, ranging from 5U to 33U of the substance according to the number of lesions. In the literature, the total dose of botulinum toxin ranged from 4U4 to 60U5 (Table 2). All cases were of multiple (more than five) and small hidrocystomas. The mean dose applied was 1-4U per lesion. In this study, the cumulative dose applied of the neuromodulator did not go beyond 33U, and the mean units per lesion was around 3U, but only one patient had more than five lesions (case 3).
The procedure was well tolerated by all patients and, regarding possible side effects, pain was the transient side effect present only during the injection.
At the end of the 120 days of follow-up, the result found was complete improvement of the lesions in one case and partial improvement in four cases (80%). These results are similar to those described in the literature cited.2,4-5,12,13
Regarding duration of effect, in the cases described by Correia et al2 and Blugerman et al,13 it was of six months, and for Kontochristopoulos et al,5 the time of clinical response was four months. Since the follow-up of the patients in this study was only of 120 days (16 weeks), the precise durability of the effect of the neurotoxin could not be determined, and a longer follow-up is needed according to the literature, recurrence already takes place between two to six weeks after the application.4,11,15,16
Differently to the cases of complete resolution described in the literature, most individuals in this study achieved partial improvement of the lesions. However, a detailed observation of the clinical photographs of the references cited shows that the size of the lesions in this sample was much larger than the cases described in the literature (Figures 6A and 6B).
The main limitation of this article was not having a precise measurement of the diameter of each lesion identified. Thus, it is not possible to correlate the dose of toxin per millimeter of lesion, and not possible to estimate the ideal dose for each size of hidrocystoma. However, it is worth highlighting that the precise size of the lesions was also not specified in the articles here mentioned. When compared to other available treatment modalities (surgical excision, electrodessication, carbon dioxide laser, caustics), the toxin has advantages: besides good healing post-procedure, has no risk of unsightly scars or dyspigmentation. This is extremely important because hidrocystomas are mainly localized on the face, and a scar on that part of the body can be more disfiguring than the lesion itself, affecting the patient's quality of life.
Despite being benign, the disfiguring and recurrent nature of hidrocystomas are elements that need to be pondered in the therapeutic choice. Botulinum toxin is an outpatient procedure, was well tolerated and However, it is worth highlighting that along this period there were no new lesions nor increase in the size of the lesions treated, what already shows superiority of the toxin over emptying the lesions with a needle. In these cases, proved capable of reducing the size and number of hidrocystoma lesions in this case series. It can be considered as a treatment option when compared to traditional methods that present risks for scarring and/or dyspigmentation. Considering there is no standard dose in the literature for the application of this neuromodulator, nor the number of sessions needed, patients should be evaluated individually considering the location, size, number and aesthetic impact of each lesion.
Ada Regina Trindade de Almeida | ORCID 0000-0002-4054-2344
Treatment and follow-up of patients. Data collection, literature review and preparation of the written text.
Jaqueline Guerra | ORCID 0000-0002-7837-9685
Data collection, literature review and preparation of the written text.
Marcelo Bellini | ORCID 0000-0002-8138-715X
Treatment and follow-up of patients.
Alessandra Romiti | ORCID 0000-0002-2231-0232
Treatment and follow-up of patients.
Maria Victoria Súarez Restrepo | ORCID 0000-0002-2614-6011
Data collection, literature review and preparation of the written text.
1. Couto Júnior AS, Batista GM, Calafiori IG, Radael VC, Mendes WB. Hidrocystoma: surgical management of cystic lesions of the eyelid. An Bras Dermatol. 2010;85(3):368-71.
2. Correia O, Duarte AF, Barros AM, Rocha N. Multiple eccrine hidrocystomas – from diagnosis to treatment: the role of dermatoscopy and botulinum toxin. Dermatology. 2009;219(1):77-9.
3. Vani D, Dayananda TR, Bharathi M, Hareesh RSK, Ravikumar V. Multiple apocrine hidrocystomas: a case report. J Clin Diagn Res. 2013; 7(1): 171-2.
4. Meys R, Perrett CM. Treatment of multiple periocular eccrine hidrocystoma: is botulinum toxin or electrocautery more effective? Clin Exp Dermatol. 2015;40(1):101-3.
5. Kontochristopoulos G, Markantoni V, Stefanaki C, Kanelleas A, Rigopoulos D, Gregoriou S. Multiple eccrine hidrocystomas treated with botulinum toxin A. Clin Exp Dermatol. 2010;36(1):95-6.
6. Yaghoobi R, Saboktain M, Feily A, Mehri M. Bilateral multiple apocrine hidrocystoma of the eyelids. Acta Dermatovenerol Alp Pannonica Adriat. 2009;18(3):138-40.
7. Schellini AS, Pinto APC, Marques MEA, Castilho CN, Achilles AB, Padovani CR. Eyelid eccrine and apocrine hidrocystoma – Occurrence at the “Faculdade de Medicina de Botucatu - São Paulo. An Bras Dermatol. 2001;76(3):283-8.
8. Verma SB. Multiple apocrine hidrocystomas: a confusing clinical diagnosis. An Bras Dermatol. 2010;85(2):260-3.
9. Sarabi K, Khachemoune A. Hidrocystomas – A Brief Review. MedGen- Med. 2006;8(3):57.
10. Sampaio SA. Definição, características, tipos e subtipos. In: Almeida ART, Hexsel DM, editors. Hiperidrose e toxina Botulínica. São Paulo: Oesp Gráfica; 2003. P. 41-45.
11. Osaki TH, Osaki MH, Osaki T, Viana GA. A Minimally Invasive Approach for Apocrine Hidrocystomas of the Eyelid. Dermatol Surg. 2016;42(1):134-6.
12. Bordelon JR, Tang N, Elston D, Niedt G, Lazic Strugar T. Multiple apocrine hidrocystomas successfully treated with botulinum toxin A. Br J Dermatol. 2016;176(2):488-90.
13. Blugerman G, Schavelzon D, D' Angelo S. Hidrocistomas écrinos Múltiplos. In: Almeida ART, Hexsel DM, editors. Hiperidrose e toxina Botulínica. São Paulo: Oesp Gráfica; 2003. P. 295-8.
14. Lee MR, Ryman W. Multiple eccrine hidrocystomas. Australas J Dermatol. 2004;45(3);178-80.
15. Gupta S, Handa U, Handa S, Mohan H. The efficacy of electrosurgery and excision in treating patients with multiple apocrine hidrocystomas. Dermatol Surg. 2001;27(4):382-4.
16. Simpson LL. The origin, structure and pharmacological activity of botulinum toxin. Pharmacol Rev. 1981;33(3):155-88.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}