


Thamiris Antonini Marçon; Beatrice Abdalla; Silvia Arroyo Rstom; Carlos D’Apparecida Santos Machado Filho; Francisco Macedo Paschoal
Received on: 09/12/2018
Approved on: 10/01/2019
Study conducted at the institution: Faculdade de Medicina do ABC - Santo André (SP), Brazil
Financial support: None
Conflict of interests: None
INTRODUCTION: Actinic keratosis (AK) is a pre-malignant lesion that can progress to squamous cell carcinoma. The diagnosis is through clinical, dermatoscopic and confocal microscopy assessment. Currently, the approach is the treatment of the field cancerization, comprising of clinically visible and subclinical AKs, for which photodynamic therapy (PDT) is a therapeutic option.
OBJECTIVE: To evaluate improvement of AKs and cancerization field in patients submitted to daylight PDT, with clinical, dermatoscopic and confocal microscopy assessment.
METHODS: Ten patients with multiple AKs on the face were selected. Daylight PDT was performed using methyl aminolevulinate and clinical, dermatoscopic and confocal microscopy photographic documentation was performed before and 60 days after the treatment.
RESULTS: Of the nine patients who completed the treatment, 8 (88.8%) showed clinical improvement and reduction in the severity of AK with one treatment. On dermatoscopy, 4 patients (44.4%) showed significant improvement, 3 patients (33.3%) showed partial improvement and 2 patients (22.2%) had no change. On confocal microscopy, 6 (66.6%) patients presented reduction in the severity of the lesion.
CONCLUSIONS: Daylight PDT proved to be effective for the treatment of AKs, with high tolerability and efficacy, besides a good safety profile.
Keywords: Dermoscopy; Keratosis, Actinic; Microscopy, Confocal; Photochemotherapy
Actinic keratosis (AK) is one of the cutaneous lesions that most commonly progresses to squamous cell carcinoma (SCC), being a result of excessive exposure to ultraviolet light.1-3 These lesions can undergo spontaneous regression, clinical stability or progression to SCC in a percentage ranging from 0.1 to 20% of cases in up to ten years.4 Its diagnosis is clinical, based on the presence of papules or erythematous plaques with white scales on photoexposed areas (face, scalp, chest and upper limbs).5 On dermoscopy, white scales and yellow follicular openings on an erythematous base can be seen, giving the aspect of pseudo-network or 'strawberry'.6 On confocal microscopy in vivo, an instrument of extensive applicability in the dermatological practice, that allows for the visualization on a cellular level with an almost histological resolution of cell and tissue features with a safe, noninvasive and real-time method,7,8 actinic keratoses can be seen by the hyperkeratosis (presence of white shiny scales on examination), irregular or atypical honeycomb pattern on the horny and granular layers of the epidermis and the presence of atypical keratinocytes.6
Treatment of actinic keratoses is important because it involves the prevention of progression of a pre-malignant lesion to squamous cell carcinoma, and many modalities can be used: cryotherapy with liquid nitrogen, surgical excision, curettage, topical medications (5-fluorouracil, trichloroacetic acid, imiquimod, ingenol mebutate and photodynamic therapy.2,4
Lately, the treatment of the cancerization field has been approached, defined as the presence of multiple actinic keratoses on photoexposed areas, associated to the presence of dysplastic keratinocytes on the adjacent skin (interlesional). Thus, treatment of these areas involves both clinically visible actinic keratosis and subclinical lesions.5
Photodynamic therapy (PDT) is a treatment where selective destruction of the target tissue takes place through a photochemical reaction using a photosensitizing substance, light and oxygen.9-11 This therapeutic modality can be used in the conventional form or with day light. In conventional PDT, the agents applied on the skin are later activated by specific light sources (broad spectrum lights, diode and laser lights) and are mainly employed for the treatment of actinic keratosis, low-risk basal cell carcinomas and Bowen's disease, with fast recovery and great cosmetic result.9,10 Daylight PDT is used for the treatment of grade I and II actinic keratoses, besides cancerization field. The substance applied is methyl aminolevulinate, that undergoes continuous metabolization into photoactive protoporphyrins, particularly protoporphyrin IX (PpIX), leading to an increased sensitivity to light only on the damaged cells.10 This way, with exposure to light, the molecules of activated porphyrins react with oxygen forming highly toxic reactive oxygen species (ROS), culminating in cell death.10,11
The objective of this study was to evaluate the improvement on actinic keratoses and cancerization field in patients submitted to daylight photodynamic therapy with methyl aminolevulinate through clinical, dermoscopic and confocal microscopy analysis.
From April 2016 to February 2017, 10 patients from the Outpatient Clinic of Dermatology from the Faculdade de Medicina do ABC, Santo André (SP), Fitzpatrick phototypes between I and III, older than 40 years, with multiple actinic keratoses (mostly grade I and II) on the face were selected; these patients signed the consent form and the study took place according to the ethical principles emanated from the Declaration of Helsinki. One lesion of actinic keratosis was selected on the face of each patient with clinical (Nikon DX AF-S Nikkor 18- 105mm), dermoscopic (Dermoscope 3Gen DermLite®, United States) and confocal microscopy (VivaScope 3000 Caliber ID®, United States) photographic record before treatment and after 60 days.
Treatment consisted in cleansing the skin to be treated with aqueous chlorhexidine, superficial curettage of the scales of actinic keratoses, application of sunscreen without physical filters (Actinica® FPS 50, Galderma) and subsequent application of a thin layer of 16% methyl aminolevulinate (Metvix®, Galderma - France) all over the face (as guided by the product information), followed by continuous sun exposure for two hours, followed by removal of the product with plain washing of the skin, and instruction to spend the rest of the day indoors, without sun exposure.
Sixty days after performing daylight PDT, the patients were re-evaluated and new photographic documentation was performed. One patient was excluded from the study because she did not attend the re-evaluation after 60 days as previously agreed upon.
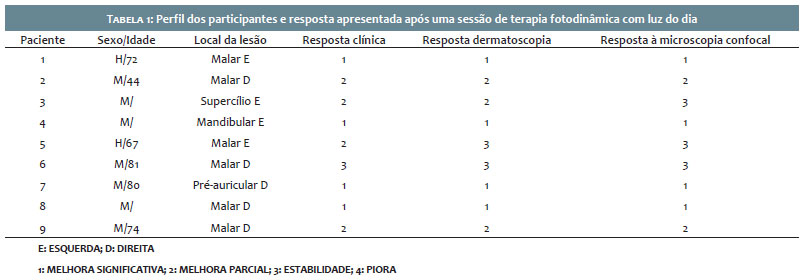
Response to treatment was graded from 1 to 4 (1: significant improvement; 2: partial improvement; 3: stable lesion; 4: worsening of the lesion) on three parameters evaluated: clinical aspect, dermoscopy and confocal microscopy.
Of the nine patients that completed the proposed treatment, four (44.4%) showed significant clinical improvement and four (44.4%) showed partial improvement. Therefore, eight of the nine patients (88.8%) improved the clinical aspect with regression of the grade of the actinic keratosis with one daylight PDT session.
Regarding dermoscopy, four patients (44.4%) showed significant improvement, being considered the improvement of the hyperkeratosis (scales) and the 'strawberry' pattern, and three patients (33.3%) showed partial improvement; this way, seven out of the nine patients (77.7%) showed improvement on the dermoscopic features. The two patients (22.2%) with stable lesion were graded like this, because even though they had initial improvement of the hyperkeratosis, there was early recurrence, determining a stable lesion.
Regarding confocal microscopy, four patients (44.4%) showed significant improvement, two patients (22.2%) showed partial improvement, so 66.6% of patients had regression on the grade of the lesion, evaluated by the improvement on the atypical honeycomb pattern, the hyperkeratosis and cell atypia.
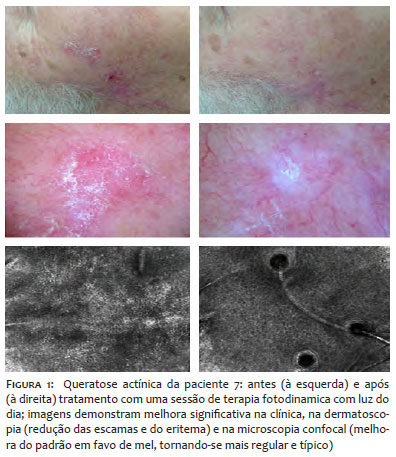
These results, as well as the characteristics of the patients and the area of the lesions, are represented on table 1 and in figure 1. It is important to highlight that, besides the improvement on actinic keratoses evaluated clinically and dermoscopically, and by Confocal microscopy, all nine patients showed improvement on the global quality of the facial skin, both in lightening of hyperpigmentation and in smoothening of fine wrinkles and skin laxity, corroborating the findings of other studies that indicate photodynamic therapy as having an effect in the improvement of cutaneous ageing (Figure 2).
During the procedure, all patients classified the treatment as painless, attributing zero (ranging from zero to ten) to pain during sun exposure. The patients developed erythema after treatment, that ranged from 1 to 4 days, and 2 patients had edema for 2 days.
Actinic keratoses represent the initial stage in the development of a squamous cell carcinoma and represent important markers for patients at risk of developing skin cancer.6 Multiple treatments are proposed aiming at regression and non-progression of these lesions to SCC, besides improvement in the cancerization field such as cryotherapy with liquid nitrogen, 5-Fluoruracil, Imiquimod and Ingenol Mebutate.4,5 Photodynamic therapy, both conventional and daylight, has been widely used for the treatment of actinic keratoses and cancerization field, demonstrating similar efficacy between both modalities confirmed by randomized, multicentric studies like those by Wiegell,13,15,16,18 Rubel3 and Lacour et al.17 This study corroborates the efficacy of daylight photodynamic therapy for the treatment of AKs, since there was improvement of the lesions, with regression on their grade in most patients.
We also highlight the importance of the evaluation of these lesions with the aid of complementary diagnostic tools, such as dermoscopy and confocal microscopy. There are few studies using these methods to compare pre- and post-treatment lesions. Jafari et al studied 40 AKs with daylight PDT by clinical response and confocal microscopy and concluded that 80% of the lesions (n = 32) showed complete regression, 17.5% (n = 7) showed partial response and only one lesion remained unchanged; with confocal microscopy, they concluded that 57.5% (n = 23) of the lesions did not show cellular atypia and 40% (n = 16) showed little atypia, when compared to the pre-treatment assessment; they also observed improvement of the honeycomb pattern hyperkeratosis, which became more regular and typical.
Most patients of this study showed clinical (88.8%), dermoscopic (77.7%) and confocal microscopy (66.6%) improvement; however, we cannot state that there was total regression of the lesions, a result that is not in keeping with the previous studies mentioned.
We also highlight that all patients were satisfied with the treatment, considered it painless and showed improvement on the overall quality of the facial skin, with smoother fine wrinkles, telangiectasias and erythema, results already previously seen when treating AKs and cancerization field with daylight PDT.19
This study has limitations such as small sample of patients (n = 9), lack of a control group and subjectivity in the exact qualification of diagnostic improvement, for example, for determining the grade of cellular atypia with confocal microscopy; however, the efficacy of the proposed treatment is certain.
Daylight photodynamic therapy proved to be effective for the treatment of actinic keratoses on the face, with improvement seen clinically, dermoscopically and on confocal microscopy. It is a treatment that represents an excellent option for the treatment of these lesions since it is well-tolerated by patients, highly effective, and has a good safety profile.
To the mentors, Prof. Francisco Macedo Paschoal and Carlos D'Apparecida S. Machado Filho, and to the collaborators in the article.
Thamiris Antonini Marçon | ORCID 0000-0002-7568-5230
Statistical analysis, approval of the final version of the original, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation, active participation on mentoring the research, intellectual participation in propaedeutics and/or therapeutics in the cases studied, critical review of the literature, critical review of the original.
Beatrice Abdalla | ORCID 0000-0003-4586-1915
Preparation and writing of the original, critical review of the original.
Silvia Arroyo Rstom | ORCID 0000-0001-89754148
Approval of the final version of the original, design and planning of the study, critical review of the original.
Carlos D'Apparecida Santos Machado Filho | ORCID 0000-0003-4362-1563
Approval of the final version of the original, critical review of the original.
Francisco Macedo Paschoal | ORCID 0000-0002-6264-1538
Design and planning of the study, active participation on mentoring the research, critical review of the original.
1. Salasche SJ. Epidemiology of actinic keratoses and squamous cell carcinoma. J Am Acad Dermatol. 2000;42(1Pt 2):4-7.
2. Wiegell SR. Daylight photodynamic therapy for actinic keratosis: an international consensus: International Society for Photodynamic Therapy in Dermatology. J Eur Acad Dermatol Venereol. 2012;26(6):673-679.
3. Rubel DM. Daylight PDT with methyl aminolevulinate cream as a convenient, similarly effective, nearly painless alternative to conventional PDT in actinic keratosis treatment: a randomised controlled trial. Br J Dermatol. 2014;171(5):1164-1171.
4. Costa C, Scalvenzi M, Ayala F, Fabbrocini G, Monfrecola G. How to treat actinic keratosis? An update. J Dermatol Case Rep. 2015;9(2):29-35.
5. Stockfleth E, Ortonne J-P, Alomar A. Actinic keratosis and field cancerisation. Eur J Dermatol 2011; 21: 1-12.
6. Zalaudek I, Piana S, Moscarella E, Longo C, Zendri E, Castagnetti F, et al . Morphologic grading and treatment of facial actinic keratosis. Clin Dermatol. 2014;32(1):80-7.
7. Selkin B, Rajadhyaksha M, Gonzalez S, Langley RG. In vivo confocal microscopy in dermatology. Dermatol Clin. 2001;19(2):369-77.
8. Aghassi D, Anderson R, Gonzalez S. Confocal laser microscopic imaging of actinic keratoses in vivo: a preliminary report. J Am Acad Dermatol. 2000;43(1 Pt 1):42-8.
9. Issa MCA, Manela-Azulay M. Terapia fotodinâmica: revisão da literatura e documentação iconográfica. An Bras Dermatol. 2010;85(4):501-11.
10. Torezan L, Niwa ABM, Festa Neto C. Photodynamic therapy in dermatology: basic principles. An Bras Dermatol. 2009;84(5):445-5.
11. Rubel DM, Spelman L, Murrell DF, See JA, Hewitt D, Foley P, et al. Daylight photodynamic therapy with methyl aminolevulinate cream as a con-venient, similarly effective, nearly painless alternative to conventional photodynamic therapy in actinic keratosis treatment: a randomized controlled trial. Br J Dermatol. 2014;171(5):1164-71.
12. Braathen LR, Szeimies RM, Basset-Seguin N, Bissonnette R, Foley P, Pariser D, et al. Guidelines on the use of photodynamic therapy for nonmelanoma skin cancer: an international consensus. International Society for Photodynamic Therapy in Dermatology, 2005. J Am Acad Dermatol. 2007;56(1):125-43.
13. Wiegell SR, Fabricius S, Stender IM, Berne B, Kroon S, Andersen BL, et al. A randomized, multicentre study of directed daylight exposure times of 1½ vs. 2½ h in daylight-mediated photodynamic therapy with methyl aminolaevulinate in patients with multiple thin actinic keratoses of the face and scalp. Br J Dermatol. 2011;164(5):1083-90.
14. Jafari SMS, Timchik T, Hunger RE. In vivo confocal microscopy efficacy assessment of daylight photodynamic therapy in actinic keratosis patients. Br J Dermatol. 2016;175(2):375-381.
15. Wiegell SR, Fabricius S, Gniadecka M, Stender IM, Berne B, Kroon S, et al. Daylight-mediated photodynamic therapy of moderate to thick actinic keratoses of the face and scalp: a randomized multicentre study. Br J Dermatol. 2012;166(6):1327-32.
16. Wiegell SR, Haedersdal M, Philipsen PA, Enk CD, Wulf HC. Continuous activation of PpIX by daylight is as effective as and less painful than conventional photodynamic therapy for actinic keratoses; a randomized, controlled, single-blinded study. Br J Dermatol. 2008;158(4):740-746.
17. Lacour JP, Ulrich C, Gilaberte Y, Von Felbert V, Basset-Seguin N, Dreno B, et al. Daylight photodynamic therapy with methyl aminolevulinate cream is effective and nearly painless in treating actinic keratoses: a randomised, investigator-blinded, controlled, phase III study throughout Europe. J Eur Acad Dermatol Venereol. 2015;29(12):2342-8.
18. Wiegell SR, Haedersdal M, Eriksen P, Wulf HC. Photodynamic therapy of actinic keratoses with 8% and 16% methyl aminolaevulinate and home-based daylight exposure: a double-blinded randomized clinical trial. Br J Dermatol. 2009;160(6):1308-14.
19. Morton CA, McKenna KE, Rhodes LE, British Association of Dermatologists Therapy Guidelines and Audit Subcommittee and the British Photodermatology Group. Guidelines for topical photodynamic therapy: update. Br J Dermatol. 2008;159(6):1246-66.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}