


Raíssa Rigo Garbin; Giovana Binda; Fernando Eibs Cafrune
Received on: 20/05/2018
Approved on: 08/12/2018
This study was performed at the Irmandade Santa Casa de Misericórdia de Porto Alegre - Porto Alegre (RS), Brazil.
Financial support: None
Conflict of interests: None
Complete surgical removal of lentigo maligna is challenging due to the difficulty in determining margins, subclinical spread and frequent facial location. In this article, we report the surgical approach of an extensive facial lentigo maligna with the "spaghetti" technique, with free margins in the third surgical step. This technique consists in the resection of a circular margin surrounding the clinical boundaries of the tumor, with histological evaluation, without removing the lesion. New steps include widening of the affected margins until the whole area is free, when tumor resection and reconstruction of the surgical defect take place simultaneously. The aim is to reach the free margins, preserving tissue in aesthetic and functional areas.
Keywords: Bloodless medical and surgical procedures; Melanoma; Skin neoplasms
In the in situ melanoma spectrum, lentigo maligna (LM) are slow growth lesions in the photoexposed areas of the elderly, especially the face. It clinically arises as irregular and poorly delimited pigmented spots. It corresponds to junctional hyperplasia of atypical melanocytes and can progress into invasive lesions. Surgical treatment is usually challenging. Due to the preference for aesthetic and functional areas, large dimensions and imprecise limits, the condition demands techniques that can provide free margins, sparing as much tissue as possible. Surgeries with margin control – such as Mohs micrographic surgery – lead to the best cure rates, however often require a long learning curve and specialized training. A technically simpler option is the spaghetti technique or perimeter staging procedure.1,2 The present paper is aimed at reporting a case of facial LM surgically approached using the spaghetti technique.
An 86-year old female patient presented to the medical visit with a brownish, irregular and asymmetric spot (3 cm in its longest diameter) in the right malar region. The spot had arisen one year before. Dermoscopy evidenced a granular grayish pigmentation area with perifollicular rhomboidal structures in the upper portion, and a hypochromic area without structures located more inferiorly, fluorescent when examined with Wood's lamp (Figure 1). After an incisional biopsy, the diagnostic suspicion of LM was confirmed. Due to the large size of the lesion, its proximity to the lower eyelid, as well as the need for a lesion-free margin of safety, a decision was made to perform its excision using the spaghetti technique.
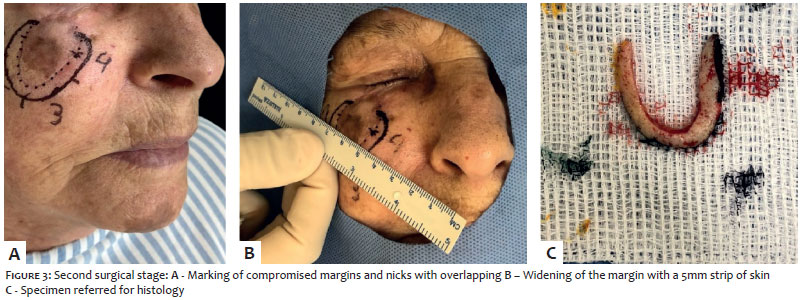
In the first surgical stage, a 5-mm perilesional skin band was excised with its histology identifying tumor cells throughout the medial, inferior and lateral segments, with free upper margin (Figure 2). In the second stage, it was possible to observe involvement of 2/3 of the inferomedial portion of the excised margin (Figure 3). In the third stage, excision of the entire lesion was performed including a new 5mm skin band in the areas that were not free of tumor. The reconstruction of the defect was carried out with a full thickness skin graft harvested from the right clavicular region (Figure 4). The final anatomopathological examination showed tumor-free margins. The postoperative period was uneventful, with no signs of infection of the operative wound (Figure 5). The aesthetic and functional outcomes were favorable.
The spaghetti technique is an alternative in the surgical treatment of LM that allows a complete analysis of the surgical margins and preservation of healthy tissue. After establishing the clinical limits of the lesion assisted by dermoscopy and Wood's lamp, a 3-5 mm skin strip is resected along the tumor's perimeter. The central island containing the macroscopic tumor is kept untouched, and the marginal defect is sutured. Despite the theoretical possibility of tumor implantation in adjacent tissues, there is no evidence to support this risk. The excised specimen is marked at cardinal points and referred for histology. In areas with persistent neoplastic cell positivity, a new skin strip is excised and subsequently analyzed, up until all margins evaluated are free of tumor. In the final stage, the lesion is completely removed, and the surgical defect is reconstructed with a skin flap or graft, or primary closure.1-4
A study carried out in France1 reviewed 16 LM cases and 5 acral lentiginous melanoma cases treated using the spaghetti technique, with a mean of 1.55 stage (1-4) and local control rate of 95.24% in two years.
A study carried out in Ontario2 with 11 patients who underwent surgery due to LM yielded a mean of 1.9 stage, with no recurrence after five months of follow-up.
Another French study3 associated the evaluation of margins by in vivo reflectance confocal microscopy in 33 patients with LM who underwent excision based on the spaghetti technique. The mean number of stages was 1.2, with 28 cases free of tumor already in the first stage. No recurrences were observed during the 10-month postoperative follow-up.
The spaghetti technique is a reliable option for treating LM. Although it requires several surggical sessions to complete the procedure, it is technically more straightforward than other surgical methods with margin control, and does not require specific training – as is the case with Mohs surgery – and yields similar cure rates.
Raíssa Rigo Garbin | ORCID 0000-0002-9771-1209
Approval of the final version of the manuscript; Study design and planning; Preparation and drafting of the manuscript; Critical review of the literature; Critical review of the manuscript; Intellectual participation in propaedeutic and / or therapeutic approach of the studied cases.
Giovana Binda | ORCID 0000-0002-9127-6736
Approval of the final version of the manuscript; Preparation and drafting of the manuscript; Critical review of the manuscript.
Fernando Eibs Cafrune | ORCID 0000-0002-6645-0122
Approval of the final version of the manuscript; Study design and planning; Intellectual participation in propaedeutic and / or therapeutic approach of the studied cases; Research guidance; Preparation and drafting of the manuscript; Critical review of the literature; Critical review of the manuscript.
1. Gaudy-Marqueste C, Perchenet AS, Taséi AM, Magalon G, Richard MA. The "spaghetti technique": an alternative to Mohs surgery or staged surgery for problematic lentiginous melanoma (lentigo maligna and acral lentiginous melanoma). J Am Acad Dermatol. 2011;64(1):113-8.
2. Mahoney M-H, Joseph M, Temple CLF. The Perimeter Technique for Lentigo Maligna: an Alternative to Mohs Micrographic Surgery. J Surg Oncol. 2005;91(2):120-5.
3. Champin J, Perror J-L, Cinotti E, Labeille B, Douchet C, Parrau G, et al. In Vivo Reflectance Confocal Microscopy to Optimize the Spaghetti Technique for Defining Surgical Margins of Lentigo Maligna. Dermatol Surg. 2014;40(3):247-56.
4. Stonecipher MR, Leshin B, Patrick J, White WL. Management of lentigo maligna and lentigo maligna melanoma with paraffin-embedded tangential sections: utility of immunoperoxidase staining and supplemental vertical sections. J Am Acad Dermatol. 1993;29(4):589-94.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}