


Daniel Nunes e Silva1; Marcelo Rosseto1; Cíntia Gründler2; Géssica de Macedo Braga Potrich1; Maurício José Scapin1
Received on: 30/01/2018
Approved on: 08/12/2018
This study was performed at Universidade Federal de Mato Grosso do Sul - Campo Grande (MS), Brazil.
Financial support: None
Conflict of interests: None
Facial hemiatrophy, or Parry-Romberg syndrome, is characterized by the progressive atrophy of the tissues of half of the face, affecting skin and subcutaneous tissue. Its clinical manifestations are very varied. Preferred therapeutic strategies for the treatment of the syndrome were not yet completely established. The authors describe a case of mild facial hemiatrophy, in which the patient underwent lipofilling (autologous fat grafting), progressing with satisfactory result. Treatment alternatives, its advantages and disadvantages are widely discussed in the study, with fat grafting emerging as an excellent therapeutic option due to its safety, low cost and replicability.
Keywords: Face; Facial hemiatrophy; Transplantation, autologous
Despite the fact it is a rare condition, with an incidence of 1:700,000 births, facial hemiatrophy is to a certain extent recurrent in dermatology and plastic surgery practices.1-3 According to the literature, it was described by Parry in 1825 and complemented by Romberg in 1846, becoming known as Parry-Romberg syndrome.1-4
The syndrome is characterized by slow and progressive atrophy of the soft tissues of the face, which may compromise osseous tissue at a later stage.2,5 It is usually unilateral, with the left side being the most affected.2-4 Facial asymmetry is the main reason for seeking medical attention, however other complaints, such as migraine, localized facial pain, eye disorders and alopecia, are also common.2,4
Its etiology is still unknown, and many possibilities are discussed in the literature: autoimmune diseases, endocrine disorders, local facial trauma, heredity, hyper or hypoactivity of the sympathetic nervous system, trigeminal nerve abnormalities and viral infections, among many others.1,4 In general, atrophy begins in childhood or puberty and continues to develop into adulthood, compromising facial aesthetics and dynamics.3 Its development is usually self-limiting; nevertheless the disease may persist for long periods in some cases, often with a disfiguring character.5
In the current literature there is no specific treatment for this syndrome. Several therapeutic options are considered, however a gold standard method has not yet been completely established.5 Interventions are usually indicated after stabilization of the atrophy process, which is often not simple to determine, and may prolong the patients suffering. For milder cases, less invasive treatments — such as cutaneous fillers, for instance with hyaluronic acid — are the most commonly mentioned options.5,6
Surgical options are usually reserved for more severe cases.3,5
The present study was aimed at describing the approach recommended by the discipline of Plastic Surgery, taught at the Universidade Federal de Mato Grosso do Sul (UFMS) for mild cases of hemifacial atrophy, describing a case treated with lipofilling (autologous lipografting). The advantages of the technique are discussed comparatively to non-surgical alternatives currently available.
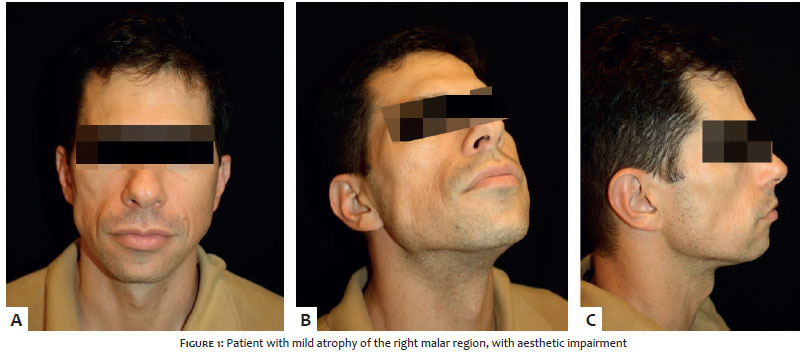
TBC, a 38-year old, white male patient, a military police officer by profession, sought medical care with the specific complaint of facial asymmetry, describing the presence of a progressive atrophy in the right malar region that had its onset roughly three years before. The patient denied other symptoms or alterations. At examination, right hemiface atrophy was observed, especially in the central and lateral portions of the right malar region. Sensitivity, strength and mobility were preserved. The diagnosis of Parry-Romberg syndrome was established (Figure 1).
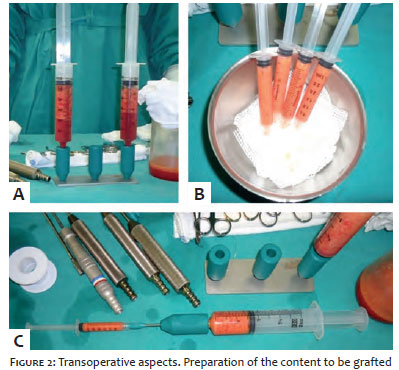
After analyzing a number of possible therapeutic alternatives, the patient chose to undergo lipofilling. The harvesting of fat (approx. 100 ml) was performed by liposuction in the lumbar region, under local anesthesia and sedation, using 60 ml syringes and 3 mm cannulas. The graft sedimented in around 30 minutes, having then been washed with 0.9% saline and transferred to 3 ml syringes (Figure 2).
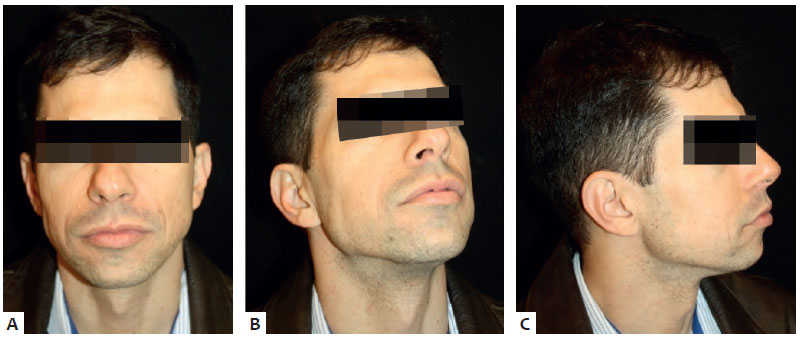
Approximately 35ml were injected into the graft recipient area, using 2mm microcannulas. The grafting was performed in tunnels, with spacing of approximately 3mm, in the patients atrophic hemiface (Figure 3).
The patient was followed up for four years. The late outcome is shown in Figure 4.
Mild cases of Parry-Romberg syndrome are usually treated with cutaneous filling due to the non-surgical and less invasive character of the technique, which is easily accepted by patients.6,7 In this context, facial filling with non-autologous material, such as hyaluronic acid, is the most commonly used option.8,9 The literature abounds with articles that report the use of filling techniques, emphasizing its straightforwardness, absence of morbidity in the donor region and, in special, the predictability of the results.7,8 Nevertheless, its high cost, especially when using larger volumes, and its short durability, have been stimulating the search for better alternatives.
The ideal cutaneous filling substance should be autologous, long lasting, without adverse effects and cost effective, being efficacious in decreasing or eliminating the patients facial volumetric loss and asymmetry.6-8 Regarding this point, lipofilling stands out as an excellent option, especially for the treatment of Parry-Romberg syndrome.
Autologous lipografting has been used in liposculpture for many years.6 Authors like Pitanguy,7 Neuber,10 Illouz11 and Coleman12 described progressive improvements in the technique, reporting excellent results. Currently, it emerges as one of the most indicated treatments for mild facial hemiatrophy, due to its advantages and low complication rates.13 With the patient under local anesthesia and sedation, the fat is usually obtained by aspiration with syringes, under low negative pressure, on an ambulatorial setting. The aspirate content sediments in the syringe and is grafted into the indicated areas.14 The surgical material required is simple, cost-effective and largely available. This method is deemed as lipopreservative and provides an adequate and efficient implantation of the grafted contents, improving the procedures outcomes.14 With the development of the technique, lipofilling has been showing excellent results, offering the main advantages the safety of being autologous, and the possibility of being used in larger volumes as compared to other cutaneous fillers.3,6,8,13,14 In addition, benefits in the donor area, such as improved body contour, are also frequently mentioned by patients.6-8 Among the main disadvantages of the procedure are the need for it to be performed in a surgical environment and the unpredictability of the integration of the lipografted content in the donor area. Complications that are common to all surgical procedures, such as infections and asymmetries, though rare, cannot be completely ruled out.6-8
When specifically addressing the treatment of patients with Parry-Romberg syndrome, fibrosis and deficiency of vascularization in the region being treated are seen as concerns regarding the viability of grafted fat cells.3 Nevertheless, for mild cases of the syndrome — such as the one presented in this paper — this aspect does not usually hampers the integration of the graft and the quality of the outcomes in the long run.13,14 The use of lipofilling in Parry-Romberg syndrome also has the theoretical advantage of offering a natural final outcome, especially regarding facial tissue texture, contour and expressions — both resting and in motion — therefore meaning that this technique is, in general, an excellent alternative to synthetic implants.13
Lipofilling has been shown to be safe and effective for the treatment of mild cases of Parry-Romberg syndrome, while its usefulness in face repair surgery has also been reaffirmed.
Daniel Nunes e Silva | ORCID 0000-0003-3050-5838
Study conception and design. Data collection, analysis and interpretation. Preparation, critical review and final approval of the manuscript. Administrative, technical and material support. Project oversight.
Marcelo Rosseto | ORCID 0000-0002-4111-9791
Data collection, analysis and interpretation. Preparation, critical review and final approval of the manuscript. Administrative, technical and material support. Project oversight.
Cíntia Gründler | ORCID 0000-0002-7416-1144
Data analysis and interpretation. Critical review and final approval of the manuscript. Administrative, technical and material support. Project oversight.
Géssica de Macedo Braga Potrich | ORCID 0000-0002-8155-371X
Data analysis and interpretation. Preparation of the manuscript, critical review and final approval of the manuscript.
Maurício José Scapin | ORCID 0000-0002-0874-0041
Data analysis and interpretation. Preparation, critical review and final approval of the manuscript
7. Vargas AF, Amorim NG, Pintaguy I. Complicações tardias dos preenchimentos permanentes. Rev Bras Cir Plást. 2009;24(1):71-81.
8. Salles AG, Remigio AFN, Zacchi VBL, Saito OC, Ferreira MC. Avaliação clínica e da espessura cutânea um ano após preenchimento de ácido hialurônico. Rev Bras Cir Plást. 2011;26(1):66-9.
9. Smith KC. Reversible vs. nonreversible fillers in facial aesthetics: Concerns and considerations. Dermatol Online J. 2008;14(8):3.
10. Wolfenson M, Santos Filho FCN. Lipoenxertia guiada por ultrassonografia. Rev Bras Cir Plást.2009;24(4):538-43.
11. Illouz YG. Illouz s technique of body contouring by lipolysis. Clin Plast Surg. 1984;11(3):409-17.
12. Coleman SR. Facial recontouring with lipostructure. Clin Plast Surg. 1997;24(2):347-67.
13. Alencar JCG, Andrade SHC, Pessoa SGP, Dias IS. Lipoenxertia autóloga no tratamento da atrofia hemifacial progressiva (síndrome de Parry-Romberg): relato de caso e revisão da literatura. An Bras Dermatol. 2011;86(4Supl1):85-8.
14. Amarante MTJ. Análise da lipoenxertia estruturada na redefinição do contorno facial. Rev Bras Cir Plást. 2013;28(1):49-54.
1. Nasser IJG,Balbinot P,Ascenço ASK, Maluf JI, Berri DT,Lopes MC,et al .Síndrome de Romberg: uma série de casos. Bras Cir Plást. 2013;28(2):201-4.
2. Guo ZN, Zhang HL, Zhou HW, Lan WJ, Wu J, Yang Y. Progressive facial hemiatrophy revisited: a role for sympathetic dysfunction. Arch Neurol. 2011;68(9):1195-7.
3. Bouchama A, Raad BF, Pitanguy I, Holanda TA, Correa WEM. Atrofia hemifacial progressiva (Síndrome de Parry-Romberg): analise de 12 anos de tratamento no instituto Ivo Pitanguy. Boletim de Cirurgia Plástica [Internet]. Nov-Dez 2013 [citado em 25 jan. 2018]; Boletim 161. Disponível em: <http://boletim.med.br/cirurgia-reparadora/atrofia-hemifacialprogressiva-sindrome-de-parry-romberg-analise-de-12-anos-de-tratamento-no-instituto-ivo-pitanguy/>.
4. Ribeiro FM, Mangilli LD, Sassi FC, Andrade CRF. Alterações do sistema miofuncional orofacial na síndrome de Parry-Romberg: revisão crítica da literatura. Rev Bras Cir Plást . 2015;30(1):114-122.
5. Cardoso LA, Carvalho PM, Kohatsu EM, Cardoso KT, Alves KV, Souza TL.
Uma nova opção cirúrgica para a Síndrome de Romberg. Acta Med Misericordiae. 2000;3(1):32-5.
6. Monteiro EO, Parada MOB. Preenchimentos faciais - parte um. RBM. 2010;67(1):6-14.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}