


Bianca De Franco Marques Ferreira; Guilherme Bezerra da Silva Modesto; Carolina Santos de Oliveira; Mário Chaves Loureiro do Carmo; Solange Cardoso Maciel Costa Silva
Received on: 05/10/2017
Approved on: 08/12/2018
This study was performed at the Hospital Universitário Pedro Ernesto (HUPE) - Universidade do Esatdo do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
Financial support: None
Conflict of interests: None
Non-melanoma skin cancer is the most common neoplasia in humans, and basal cell carcinomas (BCC) account for approximately 80% of cases. Cumulative exposure to ultraviolet radiation (UV) is the main risk factor associated to BCC, with a higher incidence in photoexposed areas, including the auricular region. The auricular region is a noble cosmetic unit, with anatomical peculiarities that lead surgeries to require the excision of a large amount of tissue, presenting a challenge for the dermatological surgeon. The authors present a case of helix reconstruction with a triple transposition flap.
Keywords: Carcinoma, basal cell; Dermatologic surgical procedures; Dermatology; Ear neoplasms; Ear, external
Non-melanoma skin cancer is the most common malignancy in humans, with basal cell carcinomas (BCC) accounting for about 80% of cases.1 Cumulative exposure to UV radiation, with intermittent and intense burn episodes, is the main risk factor associated with the genesis of BCC, evidenced by the higher incidence of this neoplasia in the photoexposed areas, such as the face and auricular region.1 Basal cell carcinoma frequently affects the head and neck of both genders and has local invasive behavior, with low metastatic potential. Complete surgical excision of the lesion is the main therapeutic approach leading to the cure.1
The auricular region is a noble cosmetic unit, whose an-atomical peculiarities demand the excision of large amounts of tissue in surgical procedures, meaning most cases are challeng-ing. The authors of the present study describe a case of a defect originated from the complete excision of a neoplastic lesion in which the ear helix was reconstructed through a triple transpo-sition flap, without complications in the peri- and postoperative periods, and with a harmonious aesthetic outcome.
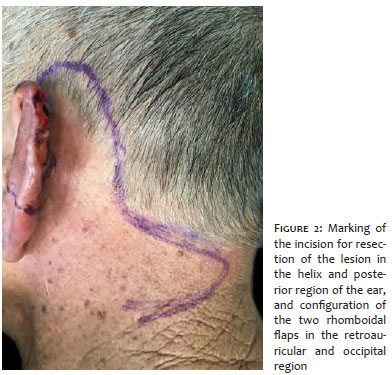
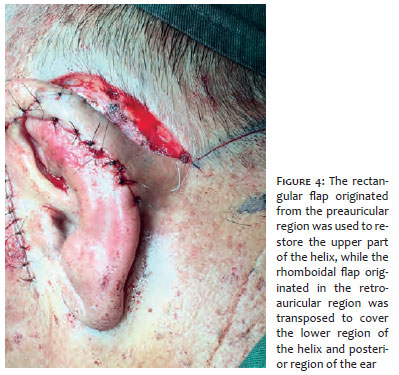
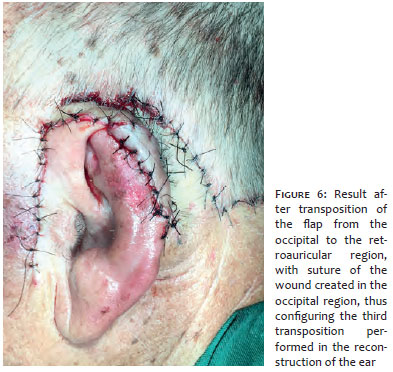
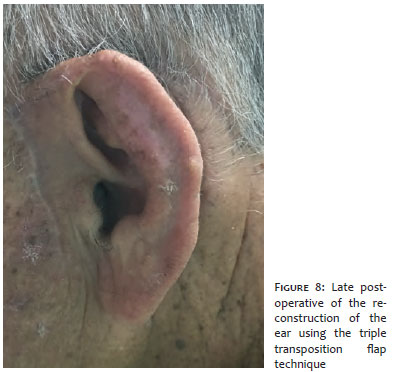
An elderly male patient, phototype II, without comorbidities, presented an ulcerated lesion on the clinicai examina-tion. The lesion was 5.5 cm in size and affected the ear helix and the posterior region of the left ear (Figure 1). The histological analysis of the previous biopsy was compatible with micronodular BCC. Due to the large size of the affected area and aiming at maintaining the symmetry of the ears, the authors of the present paper chose to perform a triple transposition flap. After delimiting the area and applying anesthetic injections circumferentially (Figure 2), the excision was performed observing margins of 5 mm (Figure 3). A rectangular pre-auricular flap was prepared and laterally rotated so as to cover the upper third of the ear helix and a small posterior area of the left auricular pavilion (Figure 4). Next, two rhomboidal flaps were cut in the retroauricular and occipital regions, the first being laterally directed to cover the posterior region of the ear (Figure 4), and the second being positioned to cover the defect created with the transposition of the first flap (Figure 5). The secondary defect was closed by direct suture (Figure 6). Two weeks later, once the vascularization had been reestablished, the retroauricular region flap’s pedicle was sectioned. As a result, the defect of the ear was completely restored by the implementation of the three flaps that were transposed (Figure 7). The patient did not have complications in the immediate or late postoperative periods, and a satisfactory aesthetic outcome was observed with the complete excision of the lesion, confirmed by the histological report (Figure 8).
The external ear is a noble cosmetic unit, as is the case of other regions such as the lips, nose and eyelids. It has a peculiar anatomical structure, with its cartilage consisting of protrusions and recesses, in addition to being lined by skin with low distension potential in certain areas. Due to this particularity, and aiming at preventing deformities and unsightly appearance, the surgical defect should be rebuilt with tissue from adjacent areas.1-2 Flaps originated in the posterior auricular region are important options, there are a number of techniques described, and the skin has a similar appearance, providing excellent esthetic and functional outcomes that are superior to those of grafts from distant sites.2 The most common head and neck region cancer is BCC, and due to its location and exposure to the sun, the ear is frequently affected,1,3 with surgical excision being the definitive treatment for these occurrences.1 Although BCC metastases are rare, the infiltrative character of the tumor can cause extensive local destruction.3 Surgical reconstruction techniques used in the auricular pavilion vary according to the location and extent of the lesion, and regional flaps or grafts may be used.1 In case of small defects in the helix, primary closure is an option, while in larger defects, advancement flaps are indicated. Transposition flaps are particularly useful for lesions in the intermediate and superior regions of the helix, and pre-auricular or retroauricular areas can be donor areas.4
Since each defect that is originated with the excision of auricular lesions has singular characteristics, dermatological surgeons face a challenge with each reconstruction. In defects located in the helix and posterior region of the external ear, where a large amount of tissue would be needed to cover the area, a combination of three transposition type flaps may be used. In this technique, a rectangular flap is prepared in the preauricu-lar region, and two other flaps rhomboidal in shape are prepared in the retroauricular and occipital regions. By transposing the flaps to cover the adjacent defects, it is possible to completely rebuild the helix and the retroauricular region, thus preserving the auricular anatomy. The method described in the present paper did not present complications during the procedure or in the postoperative period, allowed the maintenance of the peculiar structure of the region and provided a favorable aesthetic result, constituting, therefore, a relevant option for the correction of extensive lesions in the ear. The described procedure is innovative, and relatively easy and practical to perform, for it uses already established flap techniques in a, nevertheless, unusual combination: triple transposition.
Bianca De Franco Marques Ferreira | ORCID 0000-0001-5997-4246
Conception and drafting of the manuscript, literature review, photographs of the procedure and development.
Guilherme Bezerra da Silva Modesto | ORCID 0000-0002-5756-5622
Literature review, preparation of the manuscript.
Carolina Santos de Oliveira | ORCID 0000-0002-5083-5466
Literature review.
Mário Chaves Loureiro do Carmo | ORCID 0000-0003-2943-0322
Participation in the procedure and patient follow-up.
Solange Cardoso Maciel Costa Silva | ORCID 0000-0003-0812-908X
Conception of the technique, participation in the procedure and patient follow-up.
1. Kolk A, Wolff KD, Smeets R, Kesting M, Hein R, Eckert AW. Melanotic and non-melanotic malignancies of the face and external ear - A review of current treatment concepts and future options. Cancer Treat Rev. 2014;40(7):819-37.
2. Basu I, Way B, Al-Basri I. A novel lobule rotation flap for the reconstruction of middle third auricular defects. Int J Dermatol. 2013;52(12):1544-6.
3. Sand M, Sand D, Brors D, Altmeyer P, Mann B, Bechara FG. Cutaneous lesions of the external ear. Head Face Med. 2008;4(2):1-13.
4. Brodland DG. Advanced reconstruction of the ear: a framework for successful wound closure. Dermatol Surg. 2014;40 Suppl 9: S71-85.
5. Reddy LV, Zide MF. Reconstruction of skin cancer defects of the auricle. J Oral Maxillofac Surg. 2004;62(12):1457-71.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}