


John Verrinder Veasey; Nabila Scabine Pessotti
Received on: 20/08/2018
Approved on: 26/12/2018
This study was performed at the Dermatology Department, Hospital Santa Casa de São Paulo - São Paulo (SP), Brazil.
Financial support: None
Conflict of interestss: None
Scabies is a contagious cutaneous infection, caused by burrowing of the mite Sarcoptes scabiei var. hominis in the epidermis. The clinical suspicion is due to the history, clinical distribution of lesions and its aspect; however, the confirmation is with the detection of the parasite. We present the features of the diagnostic methods for scabies, from its detection through direct microscopy of skin scrapings from a lesion or with the use of an adhesive tape on the lesions, to its detection using the dermatoscope, a tool available in most dermatology clinics, which, even in unexperienced hands, has acceptable sensitivity and specificity.
Keywords: Dermoscopy; Diagnostic imaging; Microscopy; Scabies; Skin and connective tissue diseases; Skin diseases;
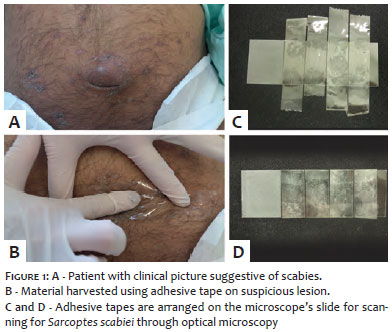
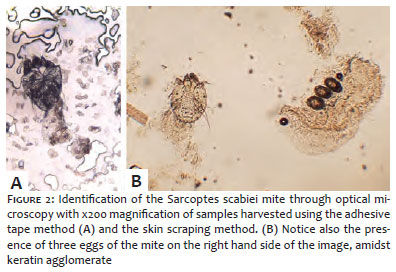
Scabies is a contagious skin infection caused by the penetration of the Sarcoptes scabiei var. hominis mite — a mandatory human parasite — in the stratum granulosum of the epidermis. It is clinically characterized by erythematous papular vesicular, and usually symmetrical lesions, with predilection for palmo-plantar and interdigital regions, armpits, nipples, periumbilical region, elbows, anterior aspect of the wrists, waist and genital area. It causes intense pruritus, especially at night. The diagnostic suspicion is based on the lesions’ history, clinical distribution and appearance.1 Scabies, however, can present atypical clinical patterns in certain circumstances, such as in patients who are on prolonged use of corticosteroids or immunosuppressed.2 The definitive diagnosis is based on the microscopic verification of the presence of mites, or their eggs or fecal fTagments. These ele-ments are classically identified by optical microscopy on samples of cutaneous scrapings harvested with a scalpel blade and placed on a glass slide with 10% potassium hydroxide. These elements can even be harvested by placing a piece of adhesive tape on the skin, slowly removing and attaching it to the microscope slides in order to allow visualization1 (Figures 1 and 2). These two methods of harvesting are also performed for the diagnosis of other parasitisms by mites, such as demodicidosis.2
In 1992, Kreusch suggested the use of dermatoscopes for in vivo detection of Sarcoptes scabiei, eliminating the need to harvest material for analysis under optical microscope.3 Since then, several authors have described the use of dermoscopes to determine the features found in this parasite, with either direct or indirect identification of the mite.3-5
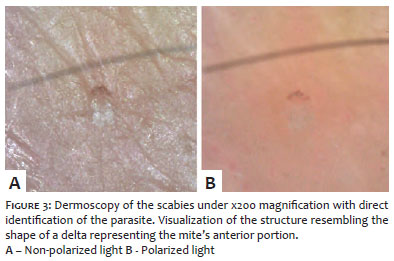
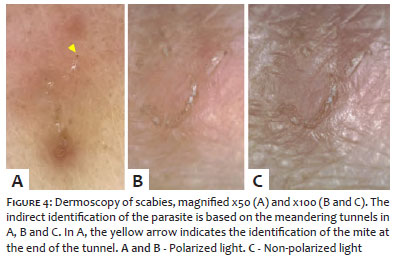
Dermoscopy enables direct visualization of the agent in the epidermis through the analysis of the most recent cutaneous lesions. In these cases, a triangular structure — corresponding to the head — and the two pairs of anterior limbs — corresponding to the anterior portion of the adult mite — can be observed (Figure 3). In addition to the benefit of being a non-invasive instrument — meaning it is well accepted by patients due to the diminished discomfort it causes — it is widely available in dermatological practices and have a further advantage as compared to the classical optical microscopy based direct methods of identification of the agent (mite): the dermoscopic analysis of the skin lesion makes it possible to indirectly evidence signs of the presence of the agent, specifically through structures resembling tunnels that correspond to the path taken by the mite in the moment of parasitism. Under dermoscopy, the tunneling structures, which are better evidenced when using nonpolarized lights, consist of a thin linear section, delimited by whitish scales. Identifying the tunnels also helps in the search for the mite, since it is at the end of this structure that Sarcoptes scabiei more frequently located (Figure 4).
There are several studies describing the experience of dermoscopic diagnoses of scabies. Dupuy et al.4 demonstrated that dermoscopy has 91% diagnostic sensitivity, as compared to 90% of skin scrapings. Likewise, dermoscopy has 86% specificity while that of skin scrapings is 100%. Another study demonstrated that skin scraping combined to dermoscopy provides more accurate and rapid diagnosis of scabies than using the first method isolatedly.5 Another noteworthy aspect in the use of the dermoscope is the absence of any risk to the patients integrity — unlike the classic harvesting performed with a scalpel blade, which can inflict cuts and abrasions on the patients skin and result in wounds in sensitive body regions, with risk of complications and unsightly scars.
The present study illustrates the importance of identifying the diagnostic aspects of scabies, facilitating the therapeutic decision in a highly contagious disease, whose delay in treatment can result in epidemic outbreaks and economic burden.
John Verrinder Veasey | ORCID 0000-0002-4256-5734
Approval of the manuscripts final version, study design and planning, manuscript preparation and drafting, effective participation in the guidance of the research, intellectual participation in the propaedeutic and / or treatment of the cases studied, critical review of the literature, critical review of the manuscript.
Nabila Scabine Pessotti | ORCID 0000-0003-0879-2981
Study design and planning; manuscript preparation and drafting; data collection, analysis and interpretation; intellectual participation in the propaedeutic and / or treatment of the cases studied, critical review of the literature, critical review of the manuscript
1. Hicks MI, Elston DM. Scabies. Dermatol Ther. 2009;22(4):279-92.
2. Veasey J, Framil V, Ribeiro A, Lellis R. Reflectance confocal microscopy use in one case of Pityriasis folliculorum: a Demodex folliculorum analysis and comparison to other diagnostic methods. Int J Dermatol. 2014;53(4):e254-7.
3. Kreusch J. Incident ligh microscopy: Reflections on microscopy of the living skin. Int J Dermatol. 1992;31(9):618-20.
4. Dupuy A, Dehen L, Bourrat E, Lacroix C, Benderdouche M, Dubertret L, et al. Accuracy of standard dermoscopy for diagnosing scabies. J Am Dermatol. 2007;56(1): 53-62.
5. Park JH, Kim CW, Kim SS. The diagnostic accuracy of dermoscopy for scabies. Ann Dermatol. 2012;24(2):194-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}