


Mauricio de Quadros1; Mariana Silveira Ferreira Mylius2; Suelen Raquel Sebben1; Ana Paula Lodi1; Gabriela Mosena3; Analupe Webber4
Received on: 11/11/2018
Approved on: 30/11/2018
This study was performed at Serviço de Dermatologia da Universidade Federal de Ciências da Saúde de Porto Alegre – Porto Alegre (RS), Brasil.
Financial support: None.
Conflict of interests: None.
INTRODUCTION: The standard application of botulinum toxin for frontal wrinkles is at the intramuscular level. Some authors have suggested that the combination with intradermal application can bring about a more natural result, avoiding the paralyzing effect of the intramuscular application only. Objective: Establish if the paralyzing effect of type A onabotulinum toxin in the forehead, applied intradermally, is as effective as of the same toxin applied intramuscularly after: 48 hours, one, two, four, eight and 12 weeks for the treatment of frontal wrinkles.
MATERIAL AND METHODS: Sixteen patients with frontal wrinkles were randomized to receive intramuscular or intradermal onabotulinum toxin and were reevaluated after 48 hours, one and two weeks, one, two and three months.
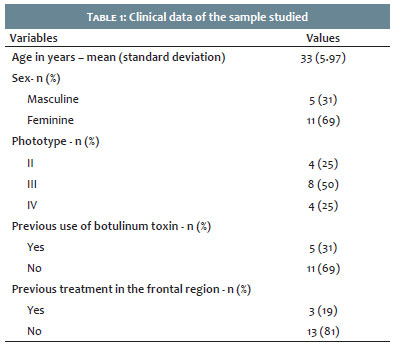
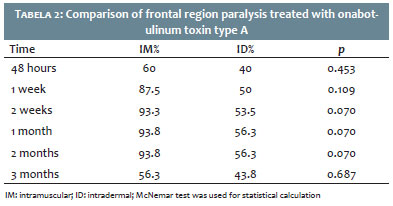
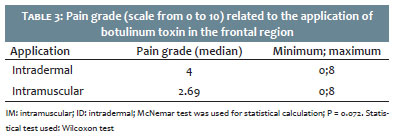
RESULTS: Data were collected from 16 patients. Mean age was 33 years (standard deviation 5.96). Paralysis occurred in 93.3% in the intramuscular side and in 53.5% in the intradermal side in two weeks (p= 0.07). Median pain grade was 2.69 in the intramuscular side and 4 in the intradermal side (p=0.072).
CONCLUSIONS: Despite the highest frequency of the presence of paralysis in the intramuscular side in all evaluations, there was no statistically significant difference between the sides.
Keywords: Botulinum toxins type A; Injections, intradermal; Injections, intramuscular
Type A botulinum toxin (BT) is a potent neurotoxin derived from the bacterium Clostridium botulinum, that has an effect in the neuromuscular junction through the inhibition of acetylcholine release, causing a temporary neuromuscular block.1 Many publications brought recommendations for the treatment of the frontal region with BT.2,3 The frontalis muscle originates in the galea aponeurotic, near the coronal suture, and is inserted in the ridge of the frontal bone in the area of the eyebrow, interlacing with fibers of the procerus, corrugator supercilli and orbicularis oculi muscles.4
It is recommended to always treat the frontalis muscle together with the glabella, since the frontalis muscle is responsible for the elevation of the upper third of the face and essential for positioning of the eyebrows.5 Treatment of the forehead can be done in the intramuscular (IM) level, but some experts recommend intradermal (ID) injection in the forehead, particularly near the eyebrows, in order to obtain a more superficial release of the toxin along the frontalis muscle with the aim of controlling the depth and extent of the effect, treating lines without lowering the eyebrow.3 Iozzo et al. suggested a combined application technique (ID and IM) according to the muscle strength and demonstrated that the level of injection regulates the potency of the effect in the muscle: the deeper the application, the stronger the effect. According to the authors, the association of different levels of BT injection (IM, subcutaneous or ID) yields natural aesthetic results, avoiding an excessively paralyzing result as what happens with only IM application.6
Jiang et al. demonstrated that the diffusion halo for BT in the frontal region is smaller when the application is performed ID in comparison to IM.7
Some studies demonstrate the benefits of the ID application of BT, such as loosening of the platysma bands and lateral fibers of the orbicularis oculi, leading to a facial lifting effect,8,9,10 reduction of sebum production, improved skin texture and erythema in patients with rosacea.11-15
The aim of this study is to compare the efficacy and durability, as well as symmetry, of the ID application of BT for the treatment of frontal dynamic wrinkles in comparison to its usual IM application. Patients will also be assessed regarding pain with both techniques.
A randomized, blind clinical trial was conducted between November 2017 and May 2018. Patients between 25 and 55 years old with symmetrical frontal wrinkles, seen at the Outpatient Department of Dermatology of the Santa Casa de Porto Alegre, RG, Brazil, were invited to participate in the study. Using the convenience sampling method, 16 patients were selected, who signed the consent form, and all completed the study. The patients that had neuromuscular disease, allergy to type A BT, facial paralysis, asymmetrical frontalis, history of BT application less than 12 months prior, history of facial lifting and use of medications that interfere in the neuromuscular junction (aminoglycosides and calcium channel blockers) were excluded. BT was reconstituted in 1ml 0.9% saline and the application was performed with 0.3ml BD Ultra-fineTM syringes with a connected 30G½ needle.
A single researcher injected in all patients participating 4U (2 points) to 6U (3 points) of BT in the frontal region intramuscularly in one side and the same amount of the substance on the other side, intradermally. The patients were instructed to avoid handling or massaging the area treated, to lie horizontally for four hours and to exercise in the following 24 hours.
To evaluate the presence of muscle paralysis and symmetry, photographic and video records were made of the faces of the patients at rest and with maximum contraction of the muscles in the frontal region, before and after the procedure, and in the six subsequent assessments (48 hours, 1, 2, 4, 8 and 12 weeks). The patients answered to questionnaires throughout the research to evaluate satisfaction, adverse effects, pain and treatment durability. After the procedure, three examiners blinded in regards to which side was treated IM or ID analyzed the videos, photographs, and the questionnaires answers for each step. In case of disagreement, photographs and videos were reassessed as a group until consensus was achieved.
Data were typed into Excel and subsequently exported to SPSS v. 20.0 for statistical analysis. Categorical variables were described by frequencies and percentages. Quantitative variables were described by the median, minimum and maximum when asymmetrical or mean and standard deviation when symmetrical. The categorical variables were compared between the treatments by the McNemar test and the quantitative by the Wilcoxon test. A level of significance of 5% was considered for the established comparisons. The project was approved by the ethics committee of the Santa Casa de Porto Alegre (CAAE number 73221517.5.0000.5335), and the study is in accordance to the Declaration of Helsinki.
Data of 16 patients were collected. The mean age was 33 years (standard deviation of 5.97), with minimum age of 25 and maximum of 45 years (Table 1).
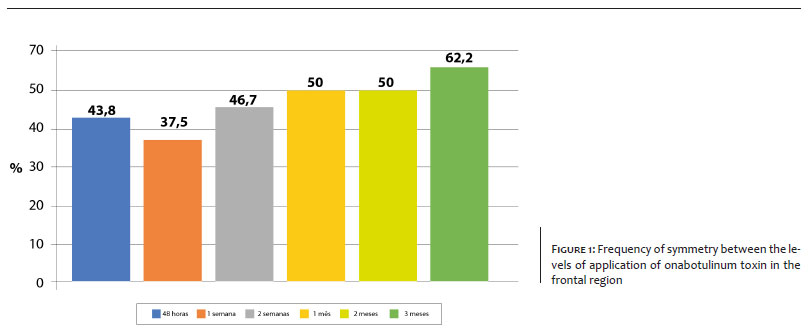
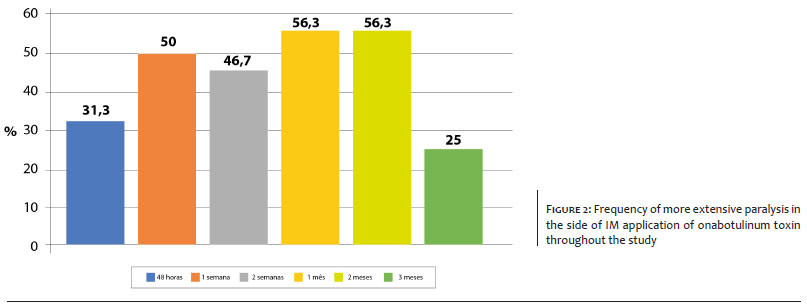
At 1 and 2 months, only 50% of the patients had symmetry with paralyzing effect (Graph 1) and between 1 week and 2 months, half the patients showed increased paralysis on side of the intramuscular injection (Graph 2). Paralysis was more frequent in the intramuscular group in all reassessments (Table 2). There was more report of pain in the side were the toxin was applied ID than in the IM side (Table 3).
Botulinum toxin acts in the neuromuscular junction, inhibits the release of acetylcholine, leading to muscle weakness or paralysis. The use of type A BT for the treatment of dynamic wrinkles is the most commonly used cosmetic procedure all over the world. This toxin can yield natural aesthetic results, maintaining to the maximum facial expressions, avoiding the 'frozen' aspect of the face.3,6 In the study by Lozzo et al., the combined technique of different levels of injection (ID, SC and IM) was demonstrated, according to the muscle strength, allowing for a better regulation of the degree of effect in the muscle: the deeper, the stronger the effect.6
The main objective of this study was to establish of the paralyzing effect of the onabotulinum toxin type A applied ID is as effective as the same toxin applied IM in 48 hours and 1, 2, 4, 8 and 12 weeks for the treatment of dynamic frontal lines. Despite of the increased frequency of muscle paralysis found in the IM side (difference above 30% in 2 weeks, 1 and 2 months after the application), it was not enough to be statistically significant. Gordin et al compared the subcutaneous (SC) application of type A botulinum toxin to the intramuscular (IM) application in the frontalis muscle of 19 patients and described that there was no statistically significant difference between the two techniques when muscle activity was evaluated.16 A study performed by Campos et al used rabbits as experimental models that received intramuscular and perimuscular botulinum toxin type A. The groups were compared with electroneuromyography and did not show statistically significant difference regarding the neuromuscular block induced by botulinum toxin in both sites of application.17
In this study, the durability of application and symmetry were also assessed. We observed that more than 90% of patients showed paralysis in the IM side of application between 2 weeks and 2 months; on the other hand, in the IM side, near 50% showed paralysis, but this difference was not statistically significant. In the third month of follow-up, 62.2% of the patients showed symmetry between the levels of application. The durability of the effect of the BT vary in different patients and can be influenced by low doses, antibody formation and muscle anatomy differences (age, sex, different patterns of frontalis muscle). One of the factors that could influence the durability is the more superficial use of the toxin, making it last for not so long.18 In relation to pain tolerance with both techniques, a higher grade was seen in the side of ID application, yet, it was not enough to show a statistically significant difference. However, in the study conducted by Gordin et al., a higher grade of pain was observed for the IM application in comparison to the SC application.16
The main imitation for the results of this study are the small sample size. Thus, a non-significant value allowed us to state that there was no difference, or that the sample was too small to detect any difference. The aim of the study was not to evaluate the necessary doses to obtain best clinical results in the frontal region, because we used the same dose for all the patients, with the objective to verify paralysis and symmetry related to the two different routes of application. Finally, the blinded evaluators conducted a subjective evaluation of photographs and videos since there was no objective measurement scale.
Despite the increased frequency of paralysis found at 2 weeks, 1 and 2 months in the IM side, there was no statistically significant difference in the efficacy and durability of the application of BT when the IM and ID levels were compared for the treatment of the frontal dynamic lines, as well as for symmetry. Data indicate that durability was similar in both groups. There was no statistically significant difference in the intensity of pain when comparing both routes of application.
Mauricio de Quadros | ORCID 0000-0003-1824-1729
Statistical analysis, approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, active role in guiding the study, intellectual participation in propaedeutics and/or treatment of studied cases, critical literature review, critical review of the original
Mariana Silveira Ferreira Mylius | ORCID 0000-0002-1741-8652
Approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, critical literature review, critical review of the manuscript
Suelen Raquel Sebben | ORCID 0000-0003-2867-1642
Approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, intellectual participation in propaedeutics and/or treatment of studied cases, critical literature review
Ana Paula Lodi | ORCID 0000-0002-9468-1366
Approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, critical literature review
Gabriela Mosena | ORCID 0000-0002-4907-2713
Approval of the final version of the original, design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation, critical literature review
Analupe Webber | ORCID 0000-0002-8781-743X
Approval of the final version of the original, design and planning of the study, preparation and writing of the original, data collection, analysis and interpretation, intellectual participation in propaedeutics and/or treatment of studied cases, critical literature review, critical review of the manuscript
1. Wohlfarth K, Muller C, Sassin I, Comes G, Grafe S. Neurophysiological double-blind trial of a botulinum neurotoxin type a free of complexing proteins. Clin Neuropharmacol. 2007;30(2):86-94.
2. Carruthers J, Fagien S, Matarasso SL; Botox Consensus Group. Consensus recommendations on the use of botulinum toxin type a in facial aesthetics. Plast Reconstr Surg. 2004;114(6 Suppl):1S-22S.
3. Sundaram H, Signorini M, Liew S,Trindade de Almeida AR, Wu Y, Braz AV, et al. Global Aesthetics Consensus: Botulinum toxin type A-evidence- based review, emerging concepts, and Consensus recommendations for aesthetic use, including updates on complications. Plast Reconstr Surg. 2016; 137(3):518e-529e.
4. Wieder JM, Moy RL. Understanding botulinum toxin. Surgical anatomy of the frown, forehead, and periocular region. Dermatol Surg. 1998;24(11):1172-4.
5. Braz AV, Sakuma TH. Frontalis muscle contraction patterns. Surg Cosmet Dermatol. 2010;2(3):191-4.
6. Iozzo I, Tengattini V, Antonucci VA. Multipoint and multilevel injection technique of botulinum toxin A in facial aesthetics. J Cosmet Dermatol. 2014; 13(2):135-42.
7. Jiang H, Shujun C, Zhou J, Leung KK, Yu P. Diffusion of two botulinum toxins type A on the forehead: double-blinded, randomized, controlled study. Dermatol Surg. 2014;40:184-192.
8. Wanitphakdeedecha R, Ungaksornpairote C, Kaewkes A, Rojanavanich V, Phothong W, Manuskiatti W.The comparison between intradermal injection of abobotulinumtoxinA and normal saline for face-lifting: a split- face randomized controlled trial. J Cosm Dermatol. 2016;15(4):452-57.
9. Petchngaovilai C. Midface lifting with botulinum toxin: intradermal technique. J Cosmet Dermatol. 2009;8(4):312-6.
10. Sapra P, Demay S, Sapra S, Khanna J, Mraud K, Bonadonna J. A Single- blind, Split-face, Randomized, pilot study comparing the effects of in-tradermal and intramuscular injection of two commercially available botulinum toxin a formulas to reduce signs of facial aging. J Clin Aesthet Dermatol. 2017;10(2):34-44.
11. Bloom BS, Payongayong L, Mourin A, Goldberg DJ. Impact of intradermal abobotulinum toxin A on facial erythema of rosacea. Dermatol Surg. 2015;41(Suppl 1):S9-S16.
12. Chang SP, Tsai HH, Chen WY, Lee WR, Chen PL, Tsai TH. The wrinkles soothing effect on the middle and lower face by intradermal injection of botulinum toxin type A. Int J Dermatol. 2008;47(12):1287-94.
13. Rose AE, Goldberg DJ. Safety and efficacy of intradermal injection of botulinum toxin for the treatment of oily skin. Dermatol Surg. 39(3 Pt 1):443-48.
14. Jeon IK, Chang SE, Park GH, Roh MR. Comparison of microneedle fractional radiofrequency therapy with intradermal botulinum toxin a injection for periorbital rejuvenation. Dermatology. 2013;227(4):367-72.
15. Zhu J, Ji X, Xu Y, Liu J, Miao YY, Zhang JA, et al.The efficacy of intradermal injection of type A botulinum toxin for facial rejuvenation. Dermatol Ther 2016; 30(1):1-4.
16. Gordin EA, Luginbuhl AL. Ortlip T, Heffelfinger RN, Krein H. Subcutaneous vs intramuscular botulinum toxin: split-face randomized study. JAMA Facial Plast Surg. 2014; 16(3): 193-98.
17. Campos JH, Oliveira LB, Queiroz TO, Santos KP, Freitas FM. Comparison between intramuscular and perimuscular injections of botulinum toxin type A. Aesth Plast Surg 2006;30(6):700-03.
18. Ahn KY, Park MY, Park DH, Han DG: Botulinum toxin A for the treatment of facial hyperkinetic wrinkle lines in Koreans. Plast Reconstr Surg. 2000; 105(2):778-84.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}