


Erica Baptista Pinto1; Carla Andréa Avelar Pires1; Walter Refkalefsky Loureiro1; Patrícia Isabel Bahia Mendes2; Samira Oliveira Silveira1; Francisca Regina Oliveira Carneiro1
Received on: 24/03/2017
Approved on: 24/09/2018
This study was performed at the Dermatology Department, Universidade do Estado do Pará – UEPA, Belém (PA), Brazil.
Financial support: None
Conflict of interests: None
Cutaneous squamous cell carcinoma (SCC) results from malignant proliferation of keratinocytes. It usually arises from the development of precursor lesions, however it may grow spontaneously on normal or chronically inflamed skin. Invasive SCC is the second most common type of non-melanoma skin cancer and accounts for 20% of all cutaneous neoplasms. The present paper reports a clinical case of cutaneous SCC, rapidly progressive and with regional metastases, which, even after complete resection of the tumor and regional lymph nodes, showed little therapeutic response and evolved to death.
Keywords: Carcinoma, Squamous cell; Neoplasm metastasis; Pathology; Skin neoplasms
Non-melanoma skin cancer is the most incident tumor in the world. In Brazil, the National Cancer Institute (Instituto Nacional de Câncer) has estimated 175,760 new cases for the biennium 2016-2017.1 Cutaneous squamous cell carcinoma (SCC) results from the malignant proliferation of the epidermal keratinocytes or their appendages. It usually arises from precursor lesions (actinic keratosis, Bowen’s disease), however can also grow spontaneously on normal skin or that bearing chronic inflammatory disorders. Considering only invasive variants, SCC it is the second most frequent form of non-melanoma skin cancer, accounting for 20% of all cutaneous neoplasms.2
Squamous cell carcinomas might initially send implants to regional lymph nodes, and later on to more distant body sites. Despite the low metastatic potential, this fact is associated with a worse prognosis, with an average survival rate of less than two years.3
It has a multifactorial etiology, and chronic ultraviolet (UV) radiation is the most important risk factor, which explains the increased incidence with age and in low latitude locations, meaning there is strong correlation with a higher intensity of ambient light. In 90% of cases, the tumor occurs in areas chronically exposed to UV radiation, such as the head, neck, dorsum of the hands and forearms, being more common in patients who work outdoors. Other risk factors are: ionizing radiations, genodermatoses, oncogenic HPV infections, chemical agents and immunosuppression.4
Usually, SCCs begin as small, hard lesions that can infiltrate extensively and deeply due to its rapid growth. The lesion may be scaly, irregular, verrucous, crateriform (keratoacanthoma-like), ulcerated or necrotic.3 In the present paper the authors report a case of rapidly progressive and metastatic SCC.
A 50-year-old male patient, phototype IV, farmer, had an ulceration for approximately four months. It the first visit, the lesion extended from the posterior cervical region to the proximal third of the right scapula, measuring 9.8 x 14.1 cm. There was presence of a necrotic and vegetative, friable floor, with irregular, elevated, infiltrated and erythematous borders adhering to the deep planes, and purulent secretion (Figure 1). The patient reported severe local pain, night fever and weight loss.
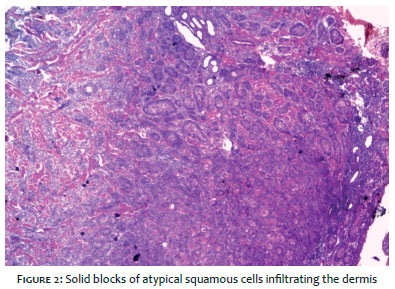
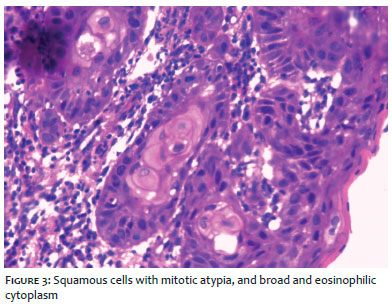
The lesion’s biopsy histology revealed the replacement of dermal structures by solid blocks consisting of atypical squamous cells with hyperchromatic nuclei containing two or more nucleoli, mitotic atypia and broad, eosinophilic cytoplasm, all of which features compatible with moderately differentiated SCC (Figures 2 and 3).
Computerized tomography scans of the neck and thorax demonstrated intense soft tissue involvement in the right posterior cervicothoracic transition, affecting the skin and subcutaneous, and loss of the cleavage plane with the trapezius muscle. Images suggestive of cervical lymph node enlargement, with necrotic center, bilaterally, measuring 3.8 x 3.4 cm to the right and 2.1 x 1.6 cm to the left, compatible with secondary implants of the disease.
Classified as T3N2M0, the patient was referred to a hospital specializing in oncologic surgery, where resection of the lesion and lymph nodes was performed and surgical wound culture was requested for graft programming (Figure 4).
The histological analysis of the surgical specimen suggested the presence of a well differentiated and ulcerated SCC, with a free, nevertheless exiguous, deep margin, with the remaining margins free of tumor. Cervical emptying level 2 revealed three lymph nodes free of neoplasia, however the axillary lymph node had three lymph nodes compromised by the neoplasia.
Subsequently, there was emergence of residual lesions and fistulization of axillary lymph nodes. After 25 days, the patient underwent a new surgery for bilateral axillary lymphadenectomy and resection of the area of recurrence in the neck.
The case coursed with purulent exudate drainage through the operative wound, with positive culture for Acinetobacter, and death due to septic shock.
The diagnosis of SCC is established histologically with the demonstration of atypical keratinocytes originating from the epidermis infiltrating the dermis. They can be well differentiated, presenting minimal pleomorphism and prominent keratinization with corneal pearls; or poorly differentiated, with pleomorphic nuclei with high degree of atypia, frequent mitoses and few corneal pearls. In rare cases of uncertain diagnosis, especially in non-keratinizing tumors, immunohistochemical differentiation markers such as cytokeratins or molecular biological markers can be applied.5
Early disease is often curable with local therapy. In a large prospective analysis of the outcomes in patients who underwent excision, the three-year survival rate was 100% for patients without adverse risk factors, nonetheless falling to 70% if at least one risk factor was present.6 A large study, with more than 900 patients with cutaneous SCC who were followed up for approximately 10 years showed recurrence rates of 4.6%, nodal disease incidence of 3.7% and mortality rate of 2.1%.7
Metastatic risk is low in most patients, remaining below 3-5% over a five-year follow-up. Approximately 85% of metastases involve regional lymph nodes, followed by distant metastases in the lungs, liver, brain, skin, and bones.3 Metastatic tumors of the trunk and extremities may sometimes involve the axillary and inguinal lymph nodes. In a study by Joseph et al.8 with 695 cases of cutaneous SCC, the mortality rate was 70.6% in the 34 cases of metastatic SCC, with almost half of these deaths due to inoperability or regional recurrence of the disease, with no evidence of distant metastases. Similarly, Oddone et al.9 observed that of 250 patients with regional head and neck metastatic disease, 70 developed recurrent regional disease, of which 73% died.
Several clinical and histological parameters have been established as prognostic factors with increased metastatic potential risk. They include tumor location (ear, lip and areas of chronic ulcers or chronic inflammation), clinical size (> 2cm), histological extension (beyond the subcutaneous tissue), histological type (acantholytic, fusiform and desmoplastic subtypes) and degree of differentiation (poorly differentiated or undifferentiated), recurrence and immunosuppression. The growth rate (fast-growing tumors versus slow-growing tumors) was also included in several risk stratification schemes. In addition, excision with positive margins is considered an independent risk for locoregional recurrence and should be classified as a high-risk tumor.4 In this manner, the present clinical case corroborates the literature findings, being classified as high risk.
More recently, the tumor’s vertical thickness has been considered, since evidence shows that tumors with < 2mm have 0% metastatic rate compared to tumors > 2mm thick, which have a metastatic rate of > 4%. Tumors in immunosuppressed patients have faster growth, greater likelihood of local recurrence, and a 5x to 10x increased risk for metastases.10
The first-line treatment is complete excision with histological control of the surgical margins. This can be performed in two ways: standard surgical excision followed by postoperative pathological evaluation of margins and micrographic surgery and its variants.10 In the case of involvement of the lymph nodes by the SCC, the preferred treatment is the dissection of regional lymph nodes.
For cutaneous SCC with a clinical diameter greater than 2cm or for tumors over 6mm thick, or tumors with other prognostic features of high risk, a margin of at least 6mm is considered mandatory.1 The European Consensus on the Diagnosis and Treatment of Invasive Cutaneous Squamous Cell Carcinoma 3 recommends a standardized minimum margin of 5mm for low risk tumors and an extended margin of 10mm or greater for high risk tumors.
Erica Baptista Pinto | ORCID 0000-0001-7568-0205
Elaboration and drafting of the manuscript, critical review of the literature, critical revision of the manuscript
Carla Andréa Avelar Pires | ORCID 0000-0002-3405-0386
Revision and approval of the final version of the original, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
Walter Refkalefsky Loureiro | ORCID 0000-0002-4957-9215
Revision and approval of the final version, intellectual participation in propaedeutic and / or therapeutic approach of the cases studied
Patrícia Isabel Bahia Mendes | ORCID 0000-0002-9678-9709
Review and approval of the final version, intellectual participation in propaedeutic and / or therapeutic approach of the cases studied
Samira Oliveira Silveira | ORCID 0000-0001-9872-1786
Review and approval of the final version, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
Francisca Regina Oliveira Carneiro | ORCID 0000-0001-6735-4004
Revision and approval of the final version, intellectual participation in the propaedeutic and / or therapeutic approach of the cases studied
1. Ministério da Saúde do Brasil, Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Estimativa 2016: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2015. 122 p.
2. Rogers HW, Weinstock MA, Harris AR, Hinckley MR, Feldman SR, Fleischer AB, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol. 2010;146(3):283-7.
3. Stratigos A, Garbe C, Lebbe C, Malvehy J, Del MV, Pehamberger H, et al. Diagnosis and treatment of invasive squamous cell carcinoma of the skin: European consensus-based interdisciplinary guideline. Eur J Cancer. 2015;51(14): 1989-2007.
4. Kyle A, Kurt AA, Amor K. Cutaneous Squamous Cell Carcinoma: A Review of High-Risk and Metastatic Disease. Am J Clin Dermatol. 2016;17(5):491-508.
5. PetterG, Haustein UF. Squamous cell carcinoma of the skin: histopathologic features and their significance for the clinical outcome. J Eur Acad Dermatol Venereol. 1998;11(1):37-44.
6. Clayman GL, Lee JJ, Holsinger FC, Zhou X, Duvic M, El-Naggar Ak, et al. Mortality risk from squamous cell skin cancer. J Clin Oncol. 2005;23(4):759-65.
7. Schmults CD, Karia PS, Carter JB, Han J, Qureshi AA. Factors predictive of recurrence and death from cutaneous squamous cell carcinoma: a 10-year, single-institution cohort study. JAMA Dermatol. 2013;149(5):541-7.
8. Joseph MG, Zulueta WP, Kennedy PJ. Squamous cell carcinoma of the skin of the trunk and limbs: the incidence of metastases and their outcome. Aust N Z J Surg. 1992;62(9):697-701.
9. Oddone N, Morgan GJ, Palme CE, Perera L, Shannon J, Wong E, et al. Metastatic cutaneous squamous cell carcinoma of the head and neck: the Immunosuppression, Treatment, Extranodal spread, and Margin status (ITEM) prognostic score to predict outcome and the need to improve survival. Cancer. 2009;115(9):1883-91.
10. Breuninger H, Eigentler T, Bootz F, Hauschild A, Kortmann RD, Wolff K, et al. Brief S2k guidelines - cutaneous squamous cell carcinoma. J Dtsch Dermatol Ges. 2013;11(Suppl) 3:37-45.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}