


Livia Matida Gontijo; Carolina Ferraz do Amaral; Lissa Sabino de Matos; André Luiz Simião
Received on: 11/09/2017
Approved on: 04/04/2018
This study was performed at the Pontifícia Universidae Católica de Campinas, (PUC Campinas) – Campinas (SP), Brazil.
Financial support: None
Conflict of interests: None
Lower lip squamous cell carcinomas (SCC) correspond to 20-30% of all oral cavity cancers. It mainly affects men over 50 years of age who have previous history of smoking, alcoholism and exposure to the sunlight. The diagnosis is clinical, confirmed by histological analysis. The present paper describes a case of a patient with a SCC affecting more than 1/3 of the lower lip, who underwent resection of the primary lesion and a conservative reconstruction of the lesion’s region, due to the great local mobility, aimed at preserving the functionality without compromising the aesthetic outcome.
Keywords: Carcinoma, squamous cell; Mouth neoplasms; Reconstruction
Skin cancer is responsible for 25% of malignant tumors reported in Brazil. Of these, basal cell carcinoma (BCC) account for 70% of the cases, squamous cell carcinoma (SCC) account for 25%, cutaneous melanoma correspond to 4%, and less common types equate to the remaining 1%. Lip tumors, on the other hand, represent roughly 15% of all head and neck neoplasms, with the lower lip being the most affected.1,2 Squamous cell carcinomas of the lower lip represent between 20% and 30% of all cancers of the oral cavity.2 Labial SCC affects males, especially patients exposed to tobacco, alcohol, ultraviolet rays and those with 50 years of age or older, with a ratio of 5:1 regarding the female gender. Rare cases were seen in Afro descendants and in children.3,4
Labial SCC clinically begins as an erythematous and hyperkeratotic papule or nodule, developing with different morphological patterns, of which the verrucous variant is the less frequent, less aggressive and more likely to be cured. In contrast, the ulcerated variant is more prone to invasion of deeper structures, and the most prevalent is the vegetating type.3, 5 Lip tumors with less than 2cm have a protracted development, good prognosis, low malignancy degree and late lymph node spread. This results in a 13.7% incidence of lymph node metastases, which is considered to be low.3-4, 6-10 Diagnosis is clinical and confirmed by histological analysis, in which nests or blocks of squamous epithelial cells originate in the epidermis and invade the dermis and deep structures. The cells arise with eosinophilic cytoplasm and vesicular nucleus. Also, the presence of intercellular bridges and the formation of corneal pearls can be observed, depending on the tumor differentiation. The Broder’s histological classification is used to analyze the percentage degree of differentiation of the cells.11 When diagnosed early, the cure rate is roughly 90% in five years.12
The treatment of choice for lip neoplasms is surgical resection. Several techniques are described for the reconstruction of the lips and the two factors governing the choice for one of them are the primary defect’s size and the labial mobility that the patient will have after the lesion’s resection. Defects that affect up to 1/3 of the lower lip can be reconstructed with primary closure, using excisions in “V” or “M”, with a W-plasty, thus generating decreased loss of functionality.12-15 In 2016, Morais and Santos report a case in which the patient underwent W-plasty experiencing a reasonable postoperative aesthetic outcome, from both the patient’s and the dermatological surgeon’s points of view. More recently, Metsavaht emphasized the importance of proper indication for W-plasty and confirmed its advantages, quoting its easy planning as an example.16-18
A 84-year-old female patient, phototype III, sought care at the Dermatology Outpatient Clinic of PUC-Campinas, São Paulo, Brazil, describing a lesion in the lower lip that had emerged roughly one year and a half before. During that period, the lesion showed progressive growth. The patient had a personal history of hypertension, ischemic heart disease and previous stroke five years before, being in use of hydrochlorothiazide, enalapril, amlodipine, warfarin and clonazepam.
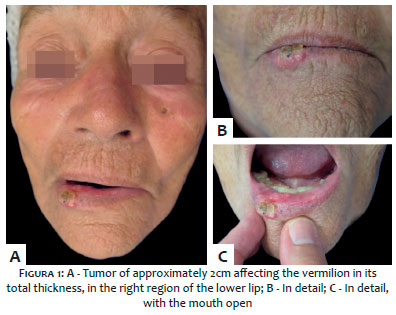
At the physical examination, the patient had a tumor of around 2cm, affecting the total thickness of the lower lip’s vermilion, on the right hand side (Figure 1).
In the mucosal region, the lesion had a verrucous surface and in the semimucosa region it had an erythematous-keratotic appearance, with crusts.
Although the lesion seemingly affected only 1/3 of the lip, palpation suggested approximately 2/3 of the lower lip were affected, with a much larger involvement having been confirmed. No palpable lymph nodes were detected in the cervical, supraclavicular and axillary chains.
The clinical diagnosis of SCC was confirmed by incisional biopsy, which revealed a well-differentiated squamous cell neoplasia. The authors of the present article chose to completely excise the lesion, considering its pattern of growth, histological type and location, which favored metastases.
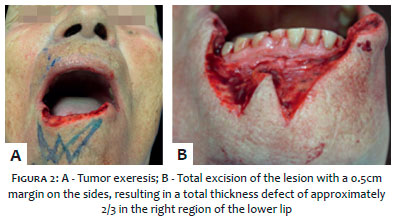
In an outpatient setting and under local anesthesia, the patient underwent the total excision of the lesion with a 0.5cm margin, resulting in a total thickness defect of approximately 2/3 of the lower right lip (Figure 2). Although there was no specific indication for the reconstruction of defects greater than 1/3 of the lip, W-plasty was chosen due to the fact that after the excision of the tumor, it was possible to observe that the patient had good elasticity and mobility of the region and could undergo a simpler technique that would preserve the lip’s motor functions without significant aesthetic loss. The W-plasty was performed beginning with the excision of a set of subsequent small triangles from the oral rhyme and oral mucosa up until the upper third of the mentum, in the portion below the anatomical defect, thus giving rise to a “W”. The procedure was performed without intercurrences.
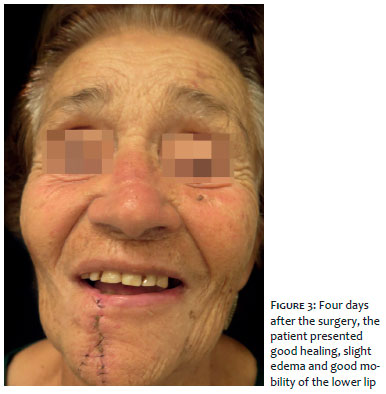
Hemostasis and suture were initially performed on the muscle plane with Vycril® 40 thread (Ethicon, New Jersey, USA), in the skin with nylon 5.0 thread, and finally, in the mucosa with catgut 5.0 thread. The edges were re-approximated in a way that the tips of the triangular flaps interdigitated, thus forming an inverse single line in “Y”. The dressing was applied with gauze and micropore, with the patient having been instructed to cleanse with water, soap and Vaseline gel twice a day at home. The patient returned to the clinic four days after presenting good healing, mild edema and satisfactory mobility of the lower lip (Figure 3).
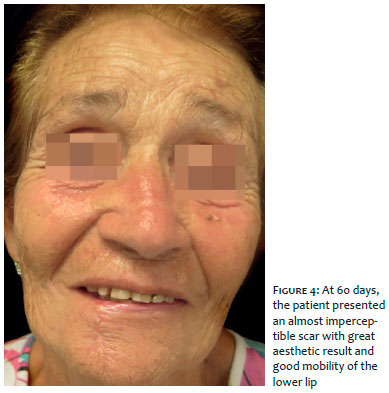
The stitches were removed after 12 days. After 60 days, the patient was satisfied with the aesthetic and functional outcomes, with an almost imperceptible scar (Figure 4).
The authors of the present article presented a case of SCC involving approximately 2/3 of the right region of lower lip. Although the W-plasty technique is not recommended for defects greater than 1/3 of the lower lip, this technique was chosen due to its low potential for loss of functionality. It is important to note that in the described case, the patient had good mobility of the region, which enabled this type of reconstruction. Therefore it is possible to conclude that the specific evaluation of each case and the experience of the dermatologic surgeon are crucial conditions for good functional and aesthetic outcomes.
Livia Matida Gontijo | ORCID 0000-0003-0130-7525
Literature review, article preparation, surgery execution
Carolina Ferraz do Amaral | ORCID 0000-0001-7102-3873
Literature review, surgery assistant
Lissa Sabino de Matos | ORCID 0000-0002323393
Final review of the article, surgery guidance
André Luiz Simião | ORCID 0000-0002-0246-2001
Article conception, final Review, surgery guidance
1. Andra C, Rauch J, Li M, Ganswindt U, Belka C, Saleh Ebrahimi L, et al. Excellent local control and survival after postoperative or definitive radiation therapy for sarcomas of the head and neck. Radiat Oncol. 2015;10:140.
2. Inca.gov.br [Internet]. Rio de Janeiro: Instituto Nacional de Câncer José Alencar Gomes da Silva; c1996-2018 [atualizado 1 out 2018; citado set 2017]. Disponível em: http://www2.inca.gov.br/.
3. Abreu MAMM, Pimentel DRN, Silva OMP, Blachman IT, Michalany NS, Hirata CHW, et al. Alchorne Carcinoma espinocelular do lábio: avaliação de fatores prognósticos. Rev Bras Otorrinolaringol. 2004;70(6):765-770.
4. Luce EA. Carcinoma of the lower lip. Surg Clin North Am. 1986;66(1):3-11
5. Ackerman LV, Del Regato JA. Cancer: diagnosis, treatment and prognosis. 4th ed. St. Louis: Mosby; 1970.
6. Baker SR. Malignant neoplasms of the oral cavity. In: Cummings CW, Fredrickson JM, Harker LA, Krause CJ, Schuller DE. Otolaryngology Head and Neck Surgery. 2ª ed. St. Louis: Mosby Year Book; 1993. p.1248-305
7. Gonzáles-Guerra HE, Calderaro-di-Ruggiero FJ, Troconis-Elorga JR, Castro-Garcia J. Carcinoma epidermóide del labio inferior: consideraciones prognósticas. Centro Med. 1991;37(2)53-8.
8. American Joint Comittee on Cancer. Lip and Oral Cavity. In: American Joint Comittee on Cancer. Manual for Staging of Cancer. 3rd ed. Philadelphia: JB Lippincott Company; 1988. p.27-32
9. Zitsch RP. Carcinoma of the lip. Otolaryngol Clin North Am. 1993;26(2):265-77.
10. Rowe DE, Carroll RJ, Day CL. Prognostic factors for local recurrence, metastasis and survival rates in squamous cell carcinoma of the skin, ear and lip. J Am Acad Dermatol 1992;26(6):976-90
11. Nuno-gonzalez A,Vicente-Martín FJ, Pinedo-Moraleda F,López-Estebaranza JL.High risk cutaneous squamous cell carcinoma. Actas Dermosifiliogr. 2012;103(7):567-78
12. Contin LA, CarvalhoMM, Machado Filho CDAS, Hayashida ME, Ferraz TS, Gonçalves Jr BF. Reconstruction of the lower lip using Karapandzic and Gilles flaps after the excision of squamous cell carcinoma. Surg Cosmet Dermatol. 2012;4(2):195-9.
13. Siqueira EJ, Alvarez GS, Laitano FL, Martins PDE, Oliveira MP. Estratégias em reconstrução do lábio inferior. Rev Bras Cir Plást. 2012;27(4):536-41.
14. Neligan PC. Strategies in lip reconstruction. Clin Plast Surg. 2009;36(3):477-85.
15. Anvar BA, Evans BC, Evans GR. Lip Reconstruction. Plast Reconstr Surg. 2007;120(4):57e-64.
16. Sbalchiero JC, Anlicoara R, Cammarota MC, Leal PRA. Reconstrução labial: abordagem funcional e estética após ressecção tumoral. Rev Soc Bras Cir Plást. 2005;20(1):40-5.
17. Baumann D, Robb G. Lip reconstruction. Semin Plast Surg. 2008;22(4):269-80.
18. Pepper JP, Baker SR. Local flaps: cheek and lips reconstruction. JAMA Facial Plast Surg. 2013;15(5):374-82
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}