


Gabriela Momente Miquelin; Elizabeth Leocadia Fernandes; Mariana Morais Tavares Colferai; Camila Carneiro Marques; Eduardo Figueiredo Gatti; Denise Steiner; Luciana Couto e Silva
Received on: 24/11/2017
Approved on: 24/09/2018
This study was performed at the Dermatology Service of the Universidade de Mogi das Cruzes (UMC) - Mogi das Cruzes (SP), Brazil.
Financial support: None
Conflict of interests: None
Systemic sclerosis (SE) is an autoimmune disease of the connective tissue. Of unknown etiology, it is characterized by sclerosis (fibrosis), which affects the skin, blood vessels and internal organs. The diagnosis is confirmed by a compatible clinical picture, autoantibody research and capillaroscopy of the nail bed. The present report highlights the importance of the dermatologist physician in the diagnosis of systemic diseases. Based on the observation of the skin – which is visible and palpable in all of its dimensions – and in the interpretation of all its signs, it is possible to conclude that it can reveal early internal disorders that could develop unnoticeably.
Keywords: Scleroderma, systemic; Fibrosis; Autoantibodies
Systemic sclerosis (SS) is an autoimmune disease of the conjunctive tissue with unknown etiology. It is characterized by sclerosis (fibrosis), which affects the skin, blood vessels and internal organs.1,2 It has universal distribution and affects all races and age groups. Its incidence in women is three to four times greater than in men, and age of onset is between 30 and 50 years.2,3 The main pathogenic abnormalities are vascular dysfunction in small arteries and microvessels, that generate a state of chronic tissular ischemia; immune activation, with production of autoantibodies, which leads to the mobilization of inflammatory cells, fibroblasts and tissular fibrosis.4 Systemic scleroses can be classified into: limited systemic sclerosis, which includes the Crest syndrome (calcinosis, Raynaud, esophagopathy, sclerodactyly and telangiectasia); diffuse systemic sclerosis; and the visceral type.2 Among the cutaneous manifestations, the following stand out: sclerodactyly; cutaneous ulcers in the fingertips and in the interphalangeal joints; microstomy; leukomelanoderma; telangiectasia and cutaneous dystrophic calcinosis.
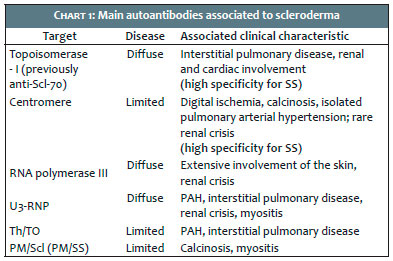
The Raynaud phenomenon is the main manifestation in the blood vessels, while esophagopathy, alveolitis with interstitial pulmonary fibrosis, pulmonary vasculopathy with pulmonary arterial hypertension (PAH) and scleroderma renal crisis are evidenced in the internal organs.1-3 Diagnosis is based on a compatible clinical picture, autoantibodies research and capillaroscopy of the nail bed. There can be positivity for the anti-nuclear and rheumatoid factors.1,3 The main autoantibodies associated to scleroderma are listed in Chart 1. The capillaroscopy of nail bed reflects the characteristic involvement of small vessels, with a 98% sensitivity for diagnosis. It is one of the several non-invasive bioengineering methods used for investigating the skin’s microcirculation, being effective for evaluating microvascular changes in the peripheral circulation, therefore having a significant role in the diagnosis of systemic sclerosis.5 Histology evidences dense sclerosis in the dermis, with compact or hyalinized collagen, atrophic eccrine and pilosebaceous glands, loss of subcutaneous fat and sparse lymphocytic infiltrate in the dermis and hypodermis; adnexal structures can be confined by the excessive deposition of collagen.1 The differential diagnoses are the scleroderma, scleromyxedema, nephrogenic fibrosing dermopathy, amyloidosis, eosinophilic fasciitis, porphyria cutanea tarda, chronic graft-versus-host disease.1,3 Treatment is challenging and comprises prevention of vasospasm and debridement of cutaneous ulcers. D-penicillamine, methotrexate and PUVA can be used for the cutaneous sclerosis, in addition to a long list of other tested agents, most of which showing ineffective.3
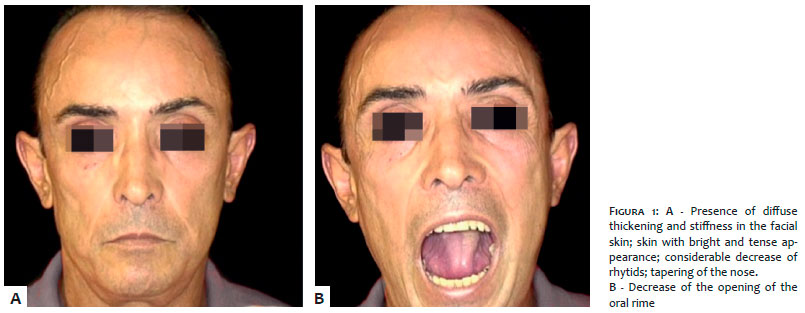
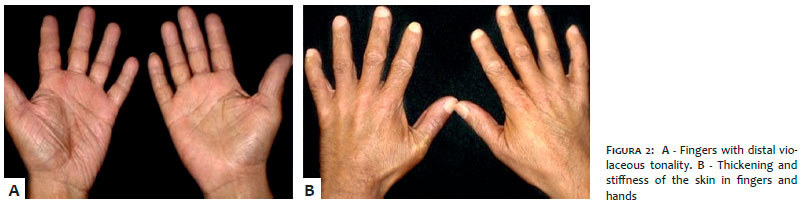
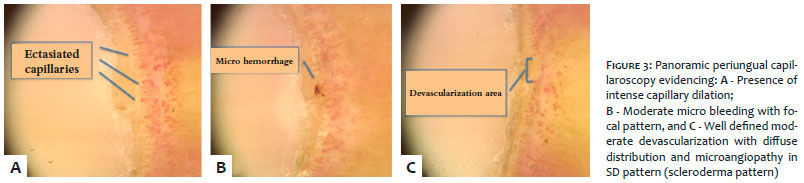
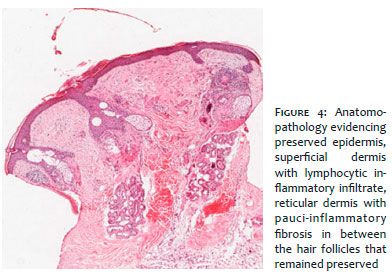
A 47-year-old, Caucasian male patient with complaints of arthralgia and edema in the hands since 2013, and weight loss. The patient denied experiencing fever, other systemic symptoms, chronic use of medicaments or other comorbidities. The dermatological examination evidenced diffuse thickening and stiffening of the skin in the face, fingers and hands; skin with bright and tense appearance in the face with considerable decrease of rhytids; decrease of the oral rime opening; tapering of the nose; violaceous tonality in the distal fingers of the hands (Figures 1 and 2). The diagnostic hypothesis of systemic sclerosis was considered. Laboratory tests evidenced: ANA positive 1/320 with mixed pattern of the thin dotted nucleolar and nuclear type; and negatives anti-Scl-70, anticentromere, anti-Ro, anti-La, anti double stranded-DNA and anti-Jo-1. The periungual panoramic capillaroscopy evidenced the presence of intense capillary dilation and moderate devascularization with diffuse distribution, moderate microhemorrhage with focal pattern, well defined SD pattern microangiopathy (scleroderma pattern) (Figure 3). The CT scan of the chest demonstrated opacities with frosted glass attenuations at the base of the lungs, poorly defined nodular images with centrilobular distribution and tree-in-budding pattern – findings that can be related to a non-specific interstitial pneumonia. The proof of pulmonary function characterized a discreet ventilatory obstructive disturb. Anatomopathology evidenced: preserved epidermis, superficial dermis with lymphocytic inflammatory infiltrate, reticular dermis with pauci-inflammatory fibrosis between the hair follicles that remained preserved; also, there is presence of numerous eosinophils in the infiltrate inflammatory; a hyaline paucicellular layer extends from the reticular dermis up until the subcutaneous and underlying fascia, with hyalinization of the vessels’ walls, compatible with scleroderma (Figure 4). Methotrexate was introduced at a 15mg/week dose; with joint follow up with a rheumatologist and a pulmonologist physician.
Systemic sclerosis is a typical idiopathic autoimmune disease, characterized by the activation of the immune system, chronic inflammation and, finally, fibrosis.6 The importance of the dermatologist physician regarding the diagnosis of systemic diseases stands out in this case report, for this specialist can interpret the skin, that is visible in all its dimensions and is directly palpable, favoring early detection of internal conditions that could evolve in a hidden way.
Gabriela Momente Miquelin | ORCID 0000-0002-8247-321X
Literature review, manuscript preparation, photographic records, article submission
Elizabeth Leocadia Fernandes | ORCID 0000-0002-2681-6775
Guidance, discussion, correction and review of the final version of the manuscript
Mariana Morais Tavares Colferai | ORCID 0000-0002-1667-4988
Literature review, manuscript preparation
Camila Carneiro Marques | ORCID 0000-0002-1905-088X
Literature review, photographs editing
Eduardo Figueiredo Gatti | ORCID 0000-0001-9544-500X
Literature review, orthographic review
Denise Steiner | ORCID 0000-0001-6450-9234
Guidance and discussion about the manuscript
Luciana Couto e Silva | ORCID 0000-0002-0516-1300
Literature review and photographic records
1. Sampaio SAP, Rivitti EA. Dermatologia. 3.ed.rev. e ampl. São Paulo: Artes médicas, 2007.
2. Belda Junior W, Di Chiacchio N, Criado PR. Tratado de Dermatologia. 2 ed. São Paulo: Atheneu,2014.
3. Azulay RD, Azulay DR. Dermatologia. 4.ed. Rio de Janeiro: Guanabara Koogan, 2006.
4. Manetti M, Guiducci S, Matucci-Cerinic M. The crowded crossroad to angiogenesis in systemic sclerosis: where is the key to the problem? Arthritis Res Ther. 2016;18(2):36-8.
5. Emrani Z, Karbalaie A, Fatemi A, Etehadtavakol M, Erlandsson BE. Capillary density: An important parameter in nailfold capillaroscopy. Microvasc Res. 2017; 109:7-18.
6. O'Reilly S, van Laar JM. Connective tissue diseases: nucleosomes and systemic sclerosis. Nat Rev Rheumatol. 2016;12(3):138-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}