


Gustavo Martins; Gabriel Fachini
Received on: 25/06/2018
Approved on: 15/08/2018
Trabalho realizado na Clínica Dr. Gustavo Martins - Transplante Capilar, Uberlândia (MG), Brazil
Financial support: None
Conflict of interests: None
INTRODUCTION: Hair transplantations promote the redistribution of hair strands on the scalp, aiming at covering the bald area. Hair transplantation using the FUE technique (Follicular Unit Extraction) usually occurs after the harvesting of the grafts. However, the earlier the grafts are implanted, the better the integration with the receiving area.
OBJECTIVE: Increase transplanted hair strands integration in the receiving area by leaving the grafts outside the body for the shortest time possible, during the implementation of hair transplantation using the FUE technique.
METHODS: An electronic chair and a litter (also electronic) were designed aiming at allowing that the harvesting and implantation of hair follicles be performed concomitantly.
RESULTS: The devices allowed modifying the surgical field, resulting in the possibility of concomitant harvesting and implantation.
CONCLUSIONS: Termed FAST FUE, this methodology provides allows simultaneous harvesting and implantation, reducing surgery time and leaving the grafts for a shorter time outside of the body.
Keywords: Alopecia; Hair; Hair/transplantation
Hair transplantation promotes redistribution of the hair on the scalp by removing grafts from the donor area and placing them in the recipient area, in which there is a lack of hair.
The FUE technique (Follicular Unit Extraction) is traditionally divided into: Extraction phase (in which the grafts are removed) and the Implantation phase (in which the grafts are implanted in the recipient area). One of the mainstays of hair transplantation is the hydration of the follicular units.1,2 In the absence of hydration, the grafts survive only for a short time.
Even when kept hydrated, the shorter the grafts are left out of the body, the better will be their integration into the recipient area3 – and fewer grafts will be lost as a consequence.
In the FUT technique (Follicular Unit Transplantation) a strip containing skin and hair is removed. The follicular units are obtained by microscopic dissection of the grafts. In this technique, the implantation is already initiated during the separation of the grafts.
In the FUE technique, extraction is carried out graft-by-graft, with hollow cylindrical instruments called punchs. The implantation is performed after the collection of grafts4, in general leaving the grafts outside the body for longer than they are left in the FUT technique.
It is recommended that the extraction period does not exceed four hours5 in order for the graft survival time is not reduced.
Aiming at leaving the grafts outside the body for the shortest time possible – consequently increasing their survival rate and integration index in the recipient area – the authors have developed the Fast FUE technique, based on the methodology used in FUE surgery, in which the grafts implantation takes place concomitantly to the follicular units extraction process.
The production line described by Henry Ford6,7 in 1913 promotes the rationalization of manufacturing based on technical and organizational changes applied to sequential activities. It has since been implemented in many situations, accelerating processes and increasing productivity.
Applying the production line methodology to the hair transplant process, the authors of the present article identified an obstacle that hampered the activity flow and potentially reduced the traditional FUE technique’s effectiveness.
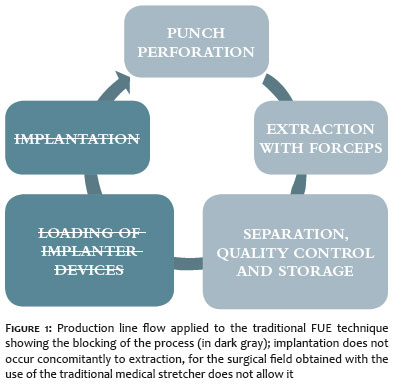
The stages of a FUE hair transplantation process can be described as follows:
Perforating with assistance of punchs;
Extraction with forceps;
Separation, quality control and storage;
Loading of implants;
Implantation.
(Figure 1)
The inability to harvest and implant at the same time arises when the patient is resting on a traditional electric medical stretcher, where the up and down adjustment movements (vertical axis) happens en bloc, meaning the patient’s complete body is ascended or descended. Some stretchers can be adjusted to the normal and inverted Tredelemburg positions, and have lateral inclination, nevertheless, these adjustments have limited amplitudes and angles in order to avoid that patients fall from the stretcher. In this kind of stretcher, all team members work on the same level. With the patient in the prone position, the surgeon’s palms and those of the assistant who is removing the units are facing downwards (Figure 2).
When the patient is in the prone position during implantation in the frontal region (the location of the majority of transplants), the implanter physician’s hands move in the opposite direction to that of the surgeon’s hands.
In order for three people to jointly work on the patient’s head, perforating (surgeon), harvesting grafts (assistant) and implanting (implanter physician), the authors of the present article have developed the appropriate equipment: an electric medical chair and an electric stretcher, both designed and manufactured aiming at providing the ideal positioning for the patient undergoing hair transplantation surgery with the FUE technique.
Both the chair and the stretcher allow the team to work on two different planes or heights: standing (surgeon and extraction assistant) and sitting (implanter physician), offering accessibility around the 360º of the patient’s skull’s circumference (Figure 3).
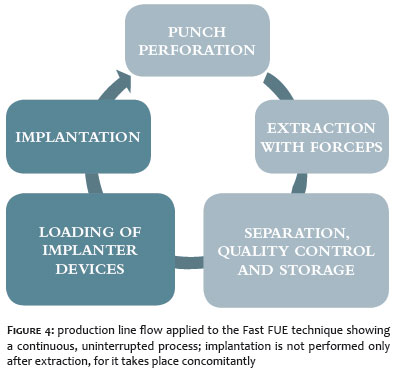
With assistance of this equipment, it was possible to carry out implants throughout the extraction period in a continuous manner, accelerating the implantation process (Figure 4).
Description of the Fast FUE technique
1) Marking of the donor and recipient areas (shaving is optional).
2) Local anesthesia of the recipient and donor area with anesthetic solution containing saline, lidocaine, ropivacaine and adrenaline.
3) Implementation of previous incisions: the dull needle implanter and premade incisions technique described by Mauro Speranzini,8 is carried out with 0.9 to 1.1mm custom blades prior to the extraction. When using sharp implanter devices, there is no need for prior incisions.
4) Comfortable positioning of the patient and surgeon, who places himself behind the patient’s left arm.
5) Motorized FUE is carried out with suction without pedal and punchs with real diameters of 0.85 to 0.95mm.
6) The assistant who removes the grafts positions him/herself behind the patient’s right arm.
7) Inspection, count, separation and storage of grafts observing the extraction time order.
8) Loading of implanters with grafts.
9) The implanter physician position him/herself in front of the patient’s head.
10) After the extraction is completed, the patient is placed in dorsal decubitus on a traditional medical stretcher, and the implantation of grafts is completed with two implanter devices at the same time.
11) Application of dressing only in the donor area.
In addition to the three people who work directly on the patient’s head, the team is composed of other people: one assistant who counts, separates and checks the quality of the follicular units; one assistant who loads the implanter devices; and one assistant who provides assistance to the team, adjusting positions and providing materials.
During the extraction process, it is possible to carry out implants with two implanter physicians at the same time, which further accelerates the implantation activity and the procedure as a whole.
By modifying the implantation area’s field, the equipment allowed to carry out implantation concomitant to extraction.
The isometric contraction of the sternocleidomastoid, scalene, and trapezius muscles is the major cause of discomfort if the headrest is inadequate or not well adapted to the patient.
The equipment developers initially designed a chair, which nevertheless it presented some limitations – in special for obese patients and those with orthopedic and rheumatologic problems, who had difficulty in remain sit. Then a stretcher was developed aimed at overcoming those limitations, providing a positioning for the head similar as that offered by the chair.
The elevation offered by both the chair and the stretcher for the head allows the surgeon and the assistant who remove the grafts to perform their task while standing, while the implanter physician can work either standing or sit, depending on his/her height and on the area to be implanted.
It was necessary to educate the team in modus operandi that was totally different from the one previously used to perform implantation procedures.
The various adjustments, the reinforced structure, in addition to the anchorage to the floor, allowed the authors of the present article to adapt the equipment to patients of different physical complexion.
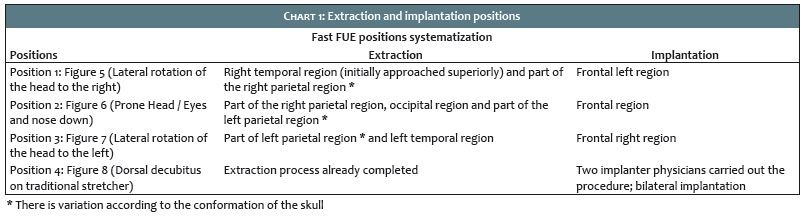
Chart 1 summarizes the extraction and implantation positions.
Position 1, which corresponds to the lateral rotation of the head to the right, was defined as the initial position (Figure 5).
Position 2, which corresponds to the occipital extraction and frontal implantation, is assumed after the extraction from the right parietal region (Figure 6).
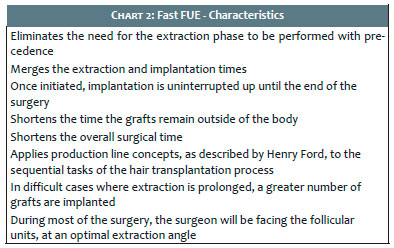
A summary of the characteristics of the Fast FUE technique is shown in Chart 2. The difficulties of preforming it include:
- a delay in one of the processes compromises the development of others in a cascade effect, which precludes the attainment of the technique’s advantages;
- to carry out the procedure in morbid obese patients with orthopedic or rheumatologic problems.
When implementing this technique, it is possible to carrying out extraction and implantation concomitantly. The mean implantation rate was 300 to 350 grafts per hour during the extraction period, when performing previous incisions. With new (and sharpened) implanters, that rate increased to 400 - 500 grafts per hour during the extraction process (with an implanter device).
In general, the surgical time is shorter than that when the implantation is performed only after extraction. The grafts are implanted more rapidly, remaining for a shorter period outside the body.
The Fast FUE methodology makes concomitant processes of extraction and implantation possible, allowing the shortening of the surgical time and of the time during which the grafts remain outside of the body.
Dr. Gustavo Martins | ORCID 0000-0001-9749-9407
Ideia original, supervisão do desenvolvimento da pesquisa e elaboração do texto final.
Dr. Gabriel Fachini | ORCID 0000-0001-5344-4850
Supervisão do desenvolvimento.
1. Limmer R. Micrograft survival. In: Stough DB, Haber RS, editors. Hair replacement : surgical and medical. St. Louis: Mosby; 1996. p. 147–9.
2. Kim JC, Hwang S. The effects of dehydration, preservation temperature and time, and hydrogen peroxide on hair grafts. In: Unger WP, Shapiro R, editors. Hair Transplantation. New York: Marcel Dekker; 200. p.285-6.
3. Kurata S, Ezaki T, Itami S, Terashi H, Takayushu S. Viability of isolatated single hair folicles preserved at 4°C. Dermatol Surg. 1999;25(1):26-9.
4. Bernstein RM, Rassman WR. Follicular unit transplantation. In: Haber RS, Stough DB, editors. Hair Transplantation. Philadelphia: Elsevier Saunders; 2006. p. 91–8.
5. Rassman WR, Bernstein RM, McClellan R, Jones R, Worton E, Uyttendaele H. Follicular unit extraction: minimally invasive surgery for hair transplantation. Dermatol Surg. 2002;28(8):720-8.
6. Womack JP, Jones DT, Roos D. The machine that changed the world. 19. ed. Rio de Janeiro: Campus; 1992.
7. PINTO GA. A organização do trabalho no século 20: taylorismo, fordismo e toyotismo. 2. ed. São Paulo: Expressão Popular; 2010.
8. Speranzini, M. FUE graft placement with dull needle implanters into premade sites. Hair Transplant Forum Int’l. 2016;26(2):49,53-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}