


Felipe Bochnia Cerci
Received on: 24/03/2018
Approved on: 27/09/2018
This study was performed at the Hospital Santa Casa de Curitiba and at the Hospital de Clínicas of the Universidade Federal do Paraná - Curitiba (PR), Brazil.
Financial support: None
Conflict of interests: None
INTRODUCTION: Interpolation flaps are well-established techniques for nasal reconstruction after the removal of skin cancers. Ideally, they should be performed after complete analysis of the surgical margins using Mohs micrographic surgery.
OBJECTIVE: To compare the paramedian forehead flap with the nasolabial interpolation flap for nasal reconstruction after Mohs surgery.
METHODS: Retrospective descriptive study of a consecutive sample of patients submitted to interpolation flaps for nasal reconstruction after Mohs surgery.
RESULTS: Twenty patients were included in the study, with 10 individuals undergoing each flap modality. Eighteen (90%) patients had defects involving multiple nasal anatomic subunits. The nasal tip (n = 10) and dorsum (n = 7) were the most affected areas in patients who underwent paramedian forehead flap, while the nasal ala (n = 10) and sidewall (n = 7) were the most affected in patients who underwent nasolabial interpolation flap. The removal of an additional portion of a subunit was performed in 15 (75%) patients. Complications were minimal and uncommon.
CONCLUSIONS: The paramedian forehead flap is more indicated for defects affecting the nasal tip and dorsum, while the nasolabial interpolation flap is more suitable for the restoration of the nasal ala. The subunit principle allowed incision lines to be camouflaged.
Keywords: Mohs surgery; Nose neoplasms; Surgical flaps
The nose's delicate anatomy, combined with its functional and aesthetic relevance, makes nasal reconstruction challenging and rewarding.1 A satisfactory outcome with functional preservation and restoration of the anatomy is crucial for different age groups, since a deformed nose has a significant psychological (and potentially physiological) impact on the patient.2
Repair options should be individualized according to the patient and surgical wound. Different options may be used, including second intention healing, primary closure, skin grafts, local flaps, interpolation flaps, and combined methods. For extensive nasal defects, however, interpolation flaps are capable of restoring the anatomy and nasal function in a superior manner, without distorting adjacent anatomical subunits.3-6
An interpolation flap can be defined as a flap that has a distal donor area which is not contiguous with the defect, a vascular pedicle with a specific artery and / or in its tributaries, and that needs more than one stage to be totally completed.7,8 This pedicle usually contains a muscle that ensures robust vascular survival, which allows it to support larger tissue volumes than those supported by local flaps' pedicles.9
The two most commonly used interpolation flaps for nasal reconstruction are the paramedian forehead flap (PFF) and the nasolabial interpolation flap (NIF). The main indications for PFF are extensive and deep wounds in the distal region of the nose (tip, ala and dorsum), whereas those for NIF are extensive and deep wounds in the nasal alae. The disadvantages of these flaps include the need for two or more stages and the scar in the donor area, which, however, generally becomes imperceptible, especially in the NIF (camouflaged in the nasolabial sulcus).7 A meticulous surgical technique and proper training are required for optimal results.
Prior to performing interpolation flaps, it is of paramount importance to develop a preoperative planning and discuss the procedure, post-operative care and possible outcomes with the patient (and family members). Although these techniques generally lead to better outcomes in extensive wounds, skin grafting can be a reasonable option for a patient whose primary goal is not aesthetics (as long as there is not functional impairment), who has multiple comorbidities, or preference for a single surgical time procedure. Nevertheless, it should be noted that despite the fact that the pedicle and replacement of dressings generates discomfort for three or four weeks, the results of the nasal restoration will remain for the rest of the patient's life.4
Surgical outcomes depend on accurate planning and execution. Well-executed interpolated flaps respect subunits and camouflage incisions whenever possible – even in extensive, complex cases. Nonetheless, it is critical to understand the underlying oncological principle prior to the reconstruction. Firstly, the entire tumor must be removed; secondly, the nose must be rebuilt. A well-executed reconstruction will be a failure if performed after an incomplete removal of the tumor.4 Ideally, interpolation flaps should only be performed after 100% of the surgical margins have been assessed and deemed free of tumor. The most used technique for checking the involvement of the margins is the Mohs micrographic surgery, which has the highest cure rates for basal cell carcinomas (BCCs) and squamous cell carcinomas (SCCs).10,11 In contrast, conventional surgery examines only roughly 1% of the surgical margins.12,13
Although there are several international publications on interpolation flaps for nasal reconstruction after Mohs micrographic surgery, the present study is the first comparing cases treated in Brazil. Thus, the objective of the present study is to compare the use of PFF and NIF for nasal reconstruction after Mohs micrographic surgery.
A retrospective descriptive study was performed with consecutive patients who underwent nasal reconstruction with PFF or NIF performed by the author between August 2014 and December 2016. Prior to the reconstruction, all tumors were treated with Mohs surgery by the same author. The study was approved by the Institution's Ethics Committee, under the protocol Nº. 64573517.7.0000.0020.
All data were routinely entered into a database immediately after the surgeries and follow-up visits. Surgeries were performed under local anesthesia with lidocaine and bupivacaine with vasoconstrictor. Nerve blocks (supraorbital and supratrochlear or infraorbital) supplemented local anesthesia. When needed, oral benzodiazepine (lorazepam) was used for greater comfort. In order to prevent patients from becoming fatigued due to the long duration of the surgeries (Mohs + reconstruction procedure), those who had not used benzodiazepine could remain seated while waiting for the Mohs surgery's stages, when they were under local anesthesia and compressive dressings. A renewed antisepsis and the application of sterile fields were performed before each new Mohs surgery stage or prior to the reconstruction. Despite being a controversial procedure – nonetheless similar to publications on interpolation flaps –3-5 patients received antibiotics pre (2g cephalexin) and postoperatively (500mg cephalexin 6-6 hours for seven days) in the first surgery.
Based on the review of the database and photographic documentation, the following demographic and surgical data were analyzed: age, gender, tumor's characteristics, size of the surgical wound and affected anatomical subunits, number of Mohs stages, flap performed, supplementary measures for patient comfort, use of cartilage graft, complications, smoking habits, use of anticoagulant, follow-up and outcomes.
The nasal subunits were divided into tip, dorsum, columella, alae, nasal walls and soft triangles.14-16 If the surgical wound extended beyond the nose, these sites were repaired independently of the interpolation flap, including second intention healing, primary closure, or local flap. When cartilage grafting was required, grafts from the concha or scaphoid fossa / anti-helix were used. Short-term complications were defined as hematoma, persistent bleeding that required intervention, infection, partial (or total) flap necrosis, and dehiscence.
Long-term complications were defined as"thick" flap, nasal ala retraction and nasal obstruction.
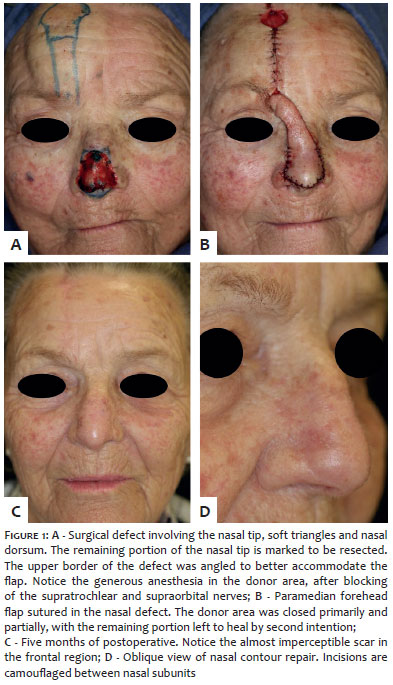
In PFF cases, the pedicle was based on the supratrochlear artery, which is situated at the medial border of the eyebrow, at between 1.7cm and 2.2cm from the midline of the face. Although Doppler can be used to locate the artery, this is usually not necessary since its location is very predictable. In addition, studies have shown that the medial forehead is a highly vascularized region supplied by the supraorbital, supratrochlear, infratrochlear, nasal dorsal, and angular arteries. These arteries form multiple anastomosis with each other and with their contralateral correspondents.17,18 To create the defect template, a suture pack was used and transferred to the frontal donor area connected to the pedicle. The flap was initially detached in the superficial subcutaneous plane, and progressively deepened to the deep subcutaneous and subgaleal planes, as the dissection approached the pedicle's base in the supraorbital rim. After having been detached, the flap was trimmed as needed and sutured with minimal tension in the nose. The donor areas were closed primarily whenever possible, leaving the remaining portions to heal by second intention (Figure 1).
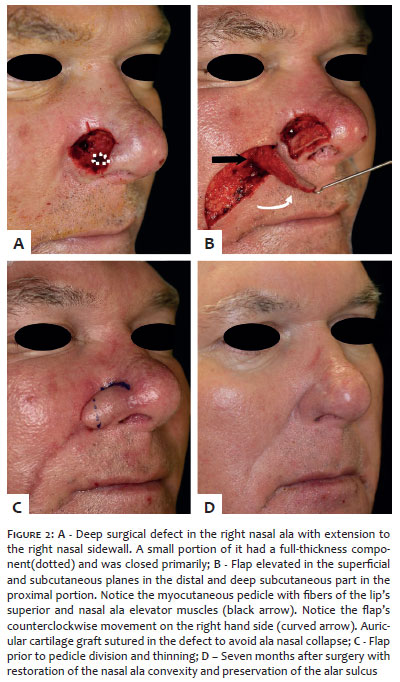
In the NIF cases, the flap was designed so as to camouflage the donor area's scar in the melolabial fold. The flap was elevated in the subcutaneous plane, preserving the muscle pedicle in an island in its proximal portion (Figure 2). The flap's thickness was adjusted for the surgical wound's depth. The donor areas were all primarily repaired.
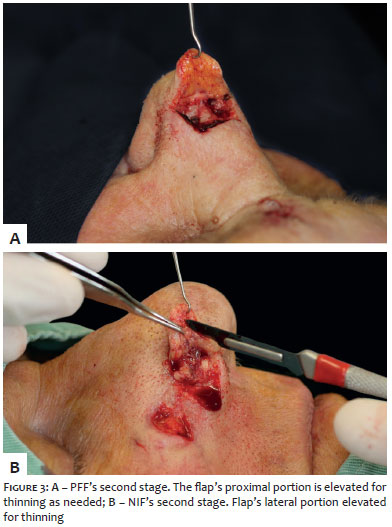
The second stage of the execution of the flaps was performed after a period ranging from three to four weeks and consisted in the sectioning of the pedicle followed by the thinning of the proximal portion of the flaps, as required (Figure 3). No further surgical revisions were performed.
For a better understanding, detailed descriptions of the execution of the PFF's and NIF's steps are available in the literature.8,19
Twenty patients were included in the study, with 10 (50%) undergoing PFF and 10 (50%) NIF, respectively. The age of the patients ranged from 38 to 77 years (mean = 64), with predominance of men (13 men / 7 women). All patients had BCC (n = 20), and 2 of them also had SCC. The most common histological subtype of BCC was the infiltrative variant. The number of Mohs surgery stages required to achieve free margins ranged from 1 to 4 (mean = 1.65). Only one patient had smoking habits, and 2 were under use of acetylsalicylic acid.
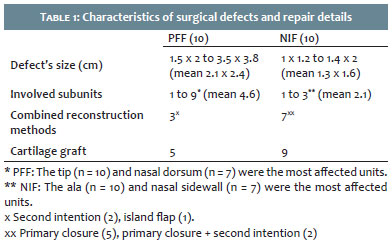
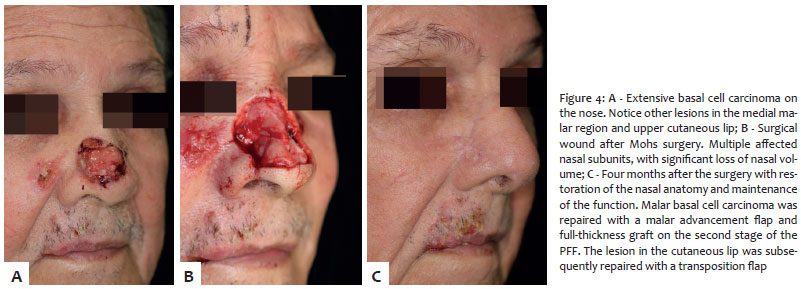
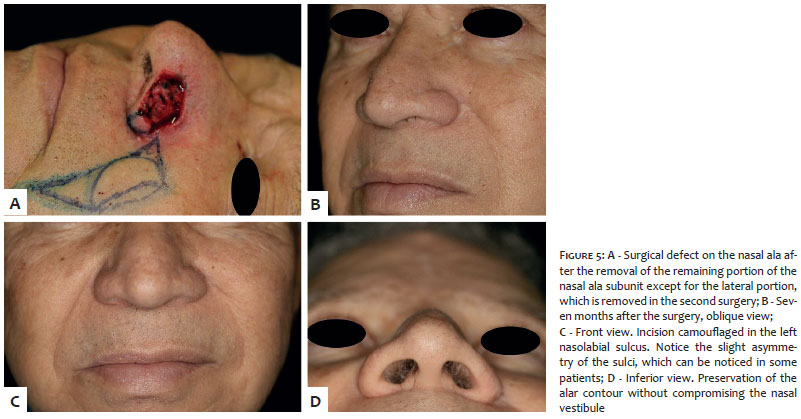
Table 1 compares Defect sizes ranged from 1.5 cm x 1.2 cm to 3.5 cm x 3.8 cm (mean = 2.1 cm x 2.4 cm) among patients submitted to PFF and from 1.0 cm x 1.2 cm to 1.4 cm x 2.0 cm (mean = 1.3 cm x 1.6 cm) in NIF cases. The mean number of anatomic subunits involved was 4.6 (n = 1 to 9) for PFF cases and 2.1 (n = 1 to 3) for NIF cases. Eighteen patients (90%) had wounds involving multiple subunits. The nasal tip (n = 10) and dorsum (n = 7) were the most affected in patients with PFF, whereas the nasal ala (n = 10) and sidewall (n = 7) were the most involved in NIF cases. Resection of an additional portion of a subunit was performed in 15 patients (75%) (Figures 4 and 5). The PFF was combined with other repair options in 3 patients, and NIF in seven. Seven patients (35%) received lorazepam as an adjuvant to local anesthesia and nerve blocks.
Restoration of the nasal mucosa was required for full-thickness defects in 4 patients (20%) and was obtained with primary closure (n = 3) or hinge flap (n = 1).
Structural support provided by auricular cartilage was necessary in 14 patients (70%) (5 (50%) in the PFF group and 9 (90%) in the NIF group). The cartilage was harvested from the scaphoid fossa / anti-helix (n = 8) or from the auricular concha (n = 6). The donor areas of the flap were completely primarily closed in all cases of NIF, however in only two cases of PFF. In all other cases, the remainder of the forehead healed by second intention (Figure 1).
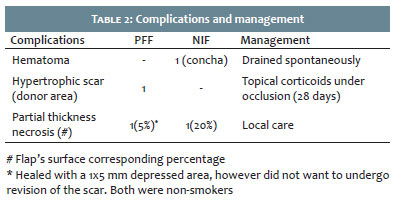
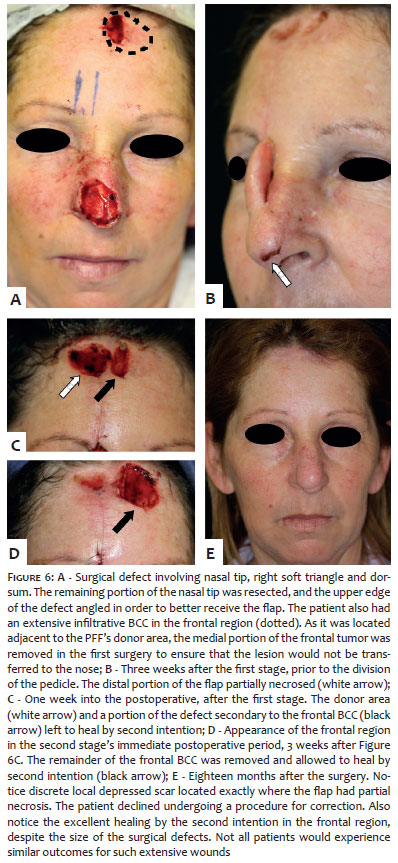
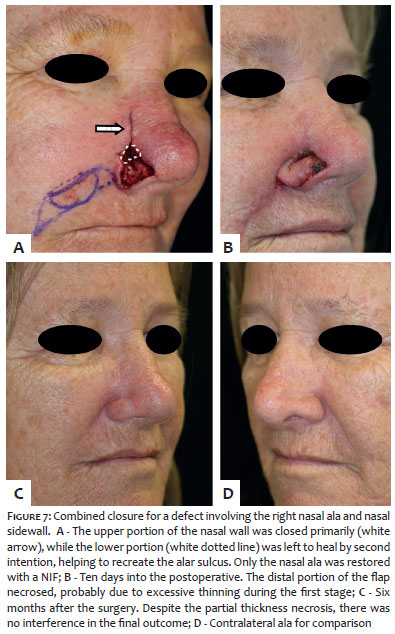
Complications were minimal, occurring in 4 out of 40 surgeries (Table 2). One patient developed hematoma in the cartilage donor area (concha) that drained spontaneously and healed without complications. Two female patients had partial distal necrosis of the flap (5% and 20% of the superficial flap respectively, Figures 6 and 7), having been treated with local wound care. One of them healed without intercurrence, while the other developed with depressed scar measuring 1mm x 5mm and chose not to undergo revision of the scar. Both were non-smokers. Another patient developed a hypertrophic scar on the forehead, treated with corticosteroid occlusion for 4 weeks. There were no cases of infection,"thick" flap or distortions of the nasal anatomy. In the long term, no patient complained of difficulty in breathing. All patients experienced excellent functional and aesthetic outcomes. After a mean follow-up of 23 months (9 to 35), there was no tumor recurrence.
The PFF and NIF are well-established techniques for nasal construction after skin cancer removal.9,20 Although the main indication for PFF is nasal tip repair, it is often used to repair surgical wounds that affect multiple nasal anatomical subunits.2,21 In the present study, the mean number of subunits involved in PFF cases was 4.6, with the nasal tip having been involved in all cases.
On the other hand, NIF is practically used for isolatedly repairing the alar subunit.6,19,22 Although patients submitted to NLIF had an average of 2.1 subunits affected, involvement of these adjacent subunits were small, and were left to heal by second intention in most cases. This detail is critical due to the fact that attempting to restore the nasal ala and sidewall with NIF alone can result in a larger nasal ala and blunting of the alar sulcus. This means that if other subunits are affected, nasal sidewall for instance, another repair method must be associated with NIF. Small adjacent defects in these areas may be left to heal by second intention.19 Following this principle, it was possible to recreate the alar sulcus and restore alar symmetry as shown in Figures 2 and 5. For medium to large defects of adjacent subunits, primary closure or cheek advancement flap are options to reduce the area left to heal by second intention, as shown in Figure 7.
Fifteen patients (75%) had the remaining portion of some subunit resected in order to allow that the same subunit was fully restored (Figures 1, 4 and 5). This is consistent with similar studies (74%8 and 78%19), and it is the essence of the nasal subunit principle, a crucial concept in reconstruction. If a defect involves more than 50% of a subunit, excising the remainder and restoring it entirely may provide better outcomes. In this manner, the incisions can be camouflaged between the subunits.15 This principle, nevertheless, is not absolute.1 Excellent outcomes can be obtained with partial replacement of the subunit. In addition, despite the nasal subunit principle's importance, other variables are determinant for the outcomes of nasal reconstructions: adequate thinning of the flap, promotion of the adequate coaptation of the flap's borders with those of the defect, similarity of the donor's skin, and flap's contour, the latter possibly being influenced by the presence of the underlying cartilage graft.23
Before executing the interpolation flap, it should be assessed whether nasal mucosa (nasal lining) is intact or should be restored. There are different options for the repair of small mucosal defects (< 1cm), among them the primary closure of the mucosa, the hinge cutaneous flap, folded PFF, full-thickness skin graft or bi-pedicled vestibular advancement flap.8,24-26 Larger mucosal defects can be restored with full-thickness skin grafts with an overlapping PFF or intranasal flaps (septal mucoperichondrial hinge flap, septal mucochondrial composed flap). When these mucosal flaps are needed, a multidisciplinary approach, with an otolaryngologist, a plastic surgeon, or head and neck surgeon is indispensable. In the present study, of the 4 patients with a full-thickness component, 3 were repaired with primary closure due to the small area involved (Figure 2), while 1 required a hinge flap of the nasal sidewall to restore the nasal lining.
After the restoration of the mucosa (when necessary), the need for a cartilage graft should be assessed. In dermatologic surgery, the ear is the most common donor area.27,28 When selecting the donor area, the scaphoid / anti-helix fossa, or concha should be considered. The following aspects should be taken into account: differences in the cartilage of these sites, morbidity and ease of removal.27,29 When native cartilage is not removed, but there is need for additional cartilage for support, the graft is called structural. In cases where cartilage has been removed, the graft is called restorative. In cases of NIF, cartilage grafts are usually structural, since there is no cartilage in most of the nasal ala, but rather fibrous tissue. Cartilage grafts in PFF can be structural or restorative, depending on the operative wound. Among cartilage's structural functions, it is possible to quote: prevention of tissue contraction and distortion, support of the flap to avoid collapse of the nasal ala, maintenance of patency of the nasal valve, and provide mechanical support for a better contour.7,8,20,27,28 In a study with 48 NIF cases, there was a high frequency of subjective nasal obstruction when cartilage grafts were not employed.6 In the present study, an auricular cartilage graft was used in 50% and 90% of PFF and RISN cases, respectively, percentages similar to those described in previous studies (67% for PFF and 94% for NIF).8,19 Among patients submitted to NIF, 1 had not undergone cartilage graft, since the defect predominantly involved the nasal tip's lateral portion. Regarding the 10 patients in the PFF group, half received cartilage grafts – 4 due to extensive involvement of the nasal ala and 1 for a better projection of the nasal tip.
The safety of performing Mohs surgery and subsequent reconstructions under local anesthesia is well established in the literature.30-32 Regarding interpolation flaps, although traditionally performed under general anesthesia or intravenous sedation, the safety of performing them under local anesthesia has been demonstrated in a study with the largest ever-published case series of interpolation flaps.3 Cook, the senior author, performed 653 interpolation flaps under local anesthesia in an outpatient setting with a low incidence of complications. In addition, the authors also reported that the procedures were well tolerated, with high patient acceptance. Nevertheless, the authors suggested that a prospective study would be important to better understand the patients' experiences and their needs. In the same study, 67% of PFF cases and 46% of NIF cases received oral diazepam during Mohs surgery or during the first stage of the reconstruction, as an adjuvant to anesthesia and nerve blocks, aiming at increasing patient comfort. The safety of oral benzodiazepines (midazolam) in healthy patients who underwent Mohs surgery was well documented by Ravitskiy et al. Midazolam offers the benefits of amnesia, reduced anxiety and alertness, and has discreetly reduced blood pressure (probably by reducing anxiety) without adverse clinical effects.34 In previous studies performed by Cerci and Nguyen, 58% (PFF) and 33% (NIF) of the patients received oral lorazepam without adverse effects.8,19 In the present study, patients without contraindications to lorazepam were informed that the medication was available for use during the surgery in case they experienced considerable anxiety or discomfort. Four patients who underwent PFF and 3 who underwent NIF made use of it. It is important to note that well-established techniques for reducing discomfort during local anesthesia were applied in all patients.
At first glance, to perform an interpolation flap under local anesthesia, with nerve blocks and oral benzodiazepine is intimidating. However, local flaps commonly performed under local anesthesia, such as nasal dorsum rotation flaps or large bilobed flaps, require significant undermining, many times of most of the nose, for adequate tissue mobilization. On the other hand, in PFF and NIF there is no need to undermine the nose, however the mobilization of tissue from the donor area might impress those who are not familiarized with the procedure. It is important to mention that supraorbital nerve and supratrochlear nerve blocks in PFF minimize or cancel the discomfort from the local anesthesia in the frontal donor area. In the case of NIF, infraorbital nerve block minimizes the discomfort on the nasal ala and nasolabial fold. Another block that was also performed was the external nasal branch of the anterior ethmoid nerve, to reduce nasal tip's anesthetic discomfort (frequently used by the author in surgeries of the nasal tip and dorsum). Through careful patient selection and adequate techniques, patients tolerate well interpolation flaps.3 However, the method of anesthesia depends on some factors, including indication, the surgeon's preference, profile and risk for the patient, availability and cost.
Potential complications of PFF and NIF include postoperative pedicle bleeding, pain, inadequate healing, infection, dehiscence, free margin distortion, flap necrosis, nasal obstruction, and"thick" flap.35 In a recent study performed by Newlove et al.,3 the complication rates of PFF and NIF that were performed by a dermatologic surgeon in an outpatient setting under local anesthesia was equal to or less than those of other surgical specialties described in other studies. It is important to note that the study's senior author (Cook) has extensive experience with interpolation flaps, being entirely dedicated to Mohs micrographic surgery and reconstruction. In a study by Padack et al., the success rate was 94.4% in 107 cases of NIFs and PFFs. The defect's thickness (partial x total), cartilage graft use, flap performed, and presence of comorbidities did not affect the results for the complications. Although not statistically significant, flap necrosis was more common in smokers.20 In the present study, the incidence of superficial necrosis of the flap (10%) was in between rates reported by the literature,8,20,35 despite the fact that it did not significantly influenced the final outcome in both cases (Figures 6 and 7).
One limitation of the present study is its retrospective character. Nonetheless, the author entered data from each surgery into the database immediately after the end of the procedure; follow-up data was entered after the return for the reassessment visits. These measurements minimize possible biases of a retrospective study.
The PFF and the NIF are fundamental and safe options for repairing nasal surgical defects after Mohs micrographic surgery. The PFF was more indicated for more extensive defects affecting the nasal tip and dorsum, while the NIF was more indicated for restoring the nasal ala. The combination with another reconstruction method was more frequent in NIF, for the repair of wounds that extended beyond the nasal ala. Auricular cartilage graft was more commonly used in cases of NIF, in order to avoid collapse of the nasal ala and resulting aesthetic and functional impairment. The detailed execution of the technique and proper planning are crucial for obtaining good outcomes.
Felipe Bochnia Cerci | ORCID 0000-0001-9605-0798
Planning, drafting, analysis and review of the study
1. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasal reconstruction--beyond aesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg. 2004;114(6):1405-16; discussion 17-9.
2. Jellinek NJ, Nguyen TH, Albertini JG. Paramedian forehead flap: advances, procedural nuances, and variations in technique. Dermatol Surg. 2014;40(Suppl 9):S30-42.
3. Newlove T, Cook J. Safety of staged interpolation flaps after Mohs micrographic surgery in an outpatient setting: a single-center experience. Dermatol Surg. 2013;39(11):1671-82.
4. Boyd CM, Baker SR, Fader DJ, Wang TS, Johnson TM. The forehead flap for nasal reconstruction. Arch Dermatol. 2000;136(11):1365-70.
5. Brodland DG. Paramedian forehead flap reconstruction for nasal defects. Dermatol Surg. 2005;31(8 Pt 2):1046-52.
6. Griffin GR, Chepeha DB, Moyer JS. Interpolated subcutaneous fat pedicle melolabial flap for large nasal lining defects. Laryngoscope. 2013;123(2):356-9.
7. Nguyen TH. Stage interpolation flaps. In: TE. Roher, JL Cook, TH Nguyen, JR Mellette Jr, editors. Flaps and grafts in dermatologic surgery. New York: Elsevier; 2007. p. 91-105.
8. Cerci FB, Nguyen TH. Paramedian forehead flap for complex nasal defects following Mohs micrographic surgery. Surg Cosmet Dermatol. 2014;6(1):17-24.
9. Mellette JR, Ho DQ. Interpolation flaps. Dermatol Clin. 2005;23(1):87-112.
10. Rowe DE, Carroll RJ, Day CL, Jr. Long-term recurrence rates in previously untreated (primary) basal cell carcinoma: implications for patient follow-up. J Dermatol Surg Oncol. 1989;15(3):315-28.
11. Alam M, Ratner D. Cutaneous squamous-cell carcinoma. N Engl J Med. 2001;344(13):975-83.
12. Shriner DL, McCoy DK, Goldberg DJ, Wagner RF, Jr. Mohs micrographic surgery. J Am Acad Dermatol. 1998;39(1):79-97.
13. Rigel DS. Cancer of the Skin. In: Stockfleth E, Rigel DS, editors. Cancer of the Skin. Philadelphia: Elsevier: New York; 2005. p. 167-73.
14. Burget GC. Aesthetic restoration of the nose. Clin Plast Surg. 1985;12(3):463-80.
15. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985;76(2):239-47.
16. Menick FJ. Aesthetic refinements in use of forehead for nasal reconstruction: the paramedian forehead flap. Clin Plast Surg. 1990;17(4):607-22.
17. Stigall LE, Bramlette TB, Zitelli JA, Brodland DG. The Paramidline Forehead Flap: A Clinical and Microanatomic Study. Dermatol Surg. 2016;42(6):764-71.
18. Reece EM, Schaverien M, Rohrich RJ. The paramedian forehead flap: a dynamic anatomical vascular study verifying safety and clinical implications. Plast Reconstr Surg. 2008;121(6):1956-63.
19. Cerci FB, Nguyen TH. Nasolabial interpolation flap for alar reconstruction after Mohs micrographic surgery Surg Cosmet Dermatol. 2014;6(2):113-20.
20. Paddack AC, Frank RW, Spencer HJ, Key JM, Vural E. Outcomes of paramedian forehead and nasolabial interpolation flaps in nasal reconstruction. Arch Otolaryngol Head Neck Surg. 2012;138(4):367-71.
21. Menick FJ. Complex nasal reconstruction: a case study: composite defect. Facial Plast Surg Clin North Am. 2011;19(1):197-211.
22. Nguyen TH. Staged cheek-to-nose and auricular interpolation flaps. Dermatol Surg. 2005;31(8 Pt 2):1034-45.
23. Shumrick KA, Campbell A, Becker FF, Papel ID. Modification of the subunit principle for reconstruction of nasal tip and dorsum defects. Arch Facial Plast Surg. 1999;1(1):9-15.
24. Pantalena L, Bordeaux JS. Reconstruction of a Multi-Subunit Defect on the Lip, Nose, and Cheek. Dermatol Surg. 2017;43(2):293-6.
25. Menick FJ. The evolution of lining in nasal reconstruction. Clin Plast Surg. 2009;36(3):421-41.
26. Menick FJ. A new modified method for nasal lining: the Menick technique for folded lining. J Surg Oncol. 2006;94(6):509-14.
27. Sage RJ, Leach BC, Cook J. Antihelical cartilage grafts for reconstruction of mohs micrographic surgery defects. Dermatol Surg. 2012;38(12):1930-7.
28. Cerci FB. Auricular cartilage graft for nasal reconstruction after Mohs micrographic surgery. Surg Cosmet Dermatol. 2015;7(2):109-15.
29. Byrd DR, Otley CC, Nguyen TH. Alar batten cartilage grafting in nasal reconstruction: functional and cosmetic results. J Am Acad Dermatol. 2000;43(5 Pt 1):833-6.
30. Alam M, Ibrahim O, Nodzenski M, Strasswimmer JM, Jiang SI, Cohen JL, et al. Adverse events associated with mohs micrographic surgery: multicenter prospective cohort study of 20,821 cases at 23 centers. JAMA Dermatol. 2013;149(12):1378-85.
31. Hussain W, Affleck A, Al-Niaimi F, Cooper A, Craythorne E, Fleming C, et al. Safety, complications and patients' acceptance of Mohs micrographic surgery under local anaesthesia: results from the U.K. MAPS (Mohs Acceptance and Patient Safety) Collaboration Group. Br J Dermatol. 2017;176(3):806-8.
32. Merritt BG, Lee NY, Brodland DG, Zitelli JA, Cook J. The safety of Mohs surgery: a prospective multicenter cohort study. J Am Acad Dermatol. 2012;67(6):1302-9.
33. Jewett BS. Interpolated forehead and melolabial flaps. Facial Plast Surg Clin North Am. 2009;17(3):361-77.
34. Ravitskiy L, Phillips PK, Roenigk RK, Weaver AL, Killian JM, Hoverson Schott A, et al. The use of oral midazolam for perioperative anxiolysis of healthy patients undergoing Mohs surgery: conclusions from randomized controlled and prospective studies. J Am Acad Dermatol. 2011;64(2):310-22.
35. Little SC, Hughley BB, Park SS. Complications with forehead flaps in nasal reconstruction. Laryngoscope. 2009;119(6):1093-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}