


Célia Luiza Petersen Vitello Kalil1; Clarissa Prieto Herman Reinehr2; Laura de Mattos Milman3; Valéria Campos4
Received on: 20/07/17
Approved on: 07/03/18
This study was performed at the Clínica Dermatológica Célia Kalil - Porto Alegre (RS), Brazil.
Financial support: None
Conflict of interests: None
Both microneedling and ablative fractional laser can be used for the treatment of scars. The present article reports the case of a female patient who had the first half of a perioral scar treated with ablative fractional CO2 laser, and the second half treated with microneedling, using a 2mm roller. Outcomes were superior in the half treated with laser.
Keywords: Cicatrix; Collagen; Lasers
Both microneedling and fractional ablative laser are beneficial for the treatment of scars. A number of conditions involving fibrosis, contractures and scarring can be treated with CO2 ablative fractional laser.1 Similarly, microneedling can also be used to stimulate skin remodeling.2 In the present case report, the authors compare the use of CO2 laser with that of microneedling for the treatment of a traumatic scar located in the perioral region.
A 35-year-old female patient sought medical care related to a scar in the perioral region, caused in an automobile accident during childhood. The patient had undergone three previous reconstructive plastic surgeries at the site aimed at improving the appearance of the scar, nonetheless was still unsatisfied. Moreover, there were limitations in the mouth opening and smiling movements (Figure 1). The scar was divided into two areas, with one of them (located in the right hemiface) being treated with CO2 ablative fractional laser, and the other (located in the left hemiface) being treated with microneedling. Topical anesthetic (lidocaine hydrochloride – 40 mg/g Dermomax® cream, Biosintética, Guarulhos, SP, Brazil) was applied 30 minutes before the procedure and supplemented with injectable anesthesia containing 1% lidocaine hydrochloride with 1:200,000 epinephrine (Xylestesin®, Cristália Produtos Químicos Farmacêuticos Ltda, São Paulo, SP, Brazil). Fractional CO2 laser (Sculptor, Vydence Medical) was performed with a 120nm tip, first pass: random mode, 140mJ energy, 75 MTZ/cm² density; second pass: brush mode, 30mJ energy, 200 MTZ/cm² density. Microneedling was conducted with Dr.Roller® needled cylinders (Mooham Enterprise Co. Gyeonggi-do, South Korea / ANVISA 80669600001). Using 2mm long needles, the rolling movement was performed from 10 to 15 times in the four directions so that 250-300 punctures/cm² were inflicted, causing uniform punctate bleeding (Figure 2). A drug delivery formulation containing 4% Hydroxyprolisilane, 5% Omega active, 2% Regestril, 2% Matrixyl 3000 and 1.5% IGF fluid anhydrous serum (Dermogral Dispensing Pharmacy, Porto Alegre, RS, Brazil) was applied immediately after the procedure. The selected active principles, such as Hydroxyprolysilane and Matrixil 3000, act in the synthesis of collagen and elastin, while others, such as Regestril and Omega active, inhibit collagenase.3 Two sessions of the procedure were performed with a 20-day interval between them.
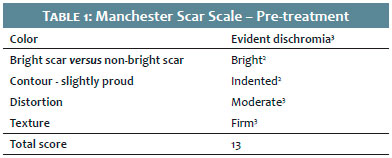
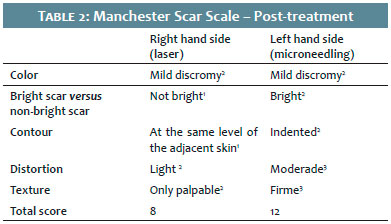
The improvement in scarring was evaluated using the Manchester Scar Scale (scores from 5 to 28, with higher scores indicating worse pictures).4 The right hand side of the scar, treated with CO2 laser, presented better outcomes (Figures 3A and B). The initial Manchester Scar Scale score for both sides was 13 points (Table 1). After the treatment, the area treated with laser improved by 5 points, while the area treated with microneedling improved by only 1 point (Table 2).
Both microneedling – also termed percutaneous collagen induction – and ablative fractional lasers are effective therapeutic options for the treatment of scars. In addition, both methods allow drug delivery processes, which optimize topical delivery of active principles.
The remodeling that occurs after the use of CO2 laser is caused by the photomechanical effect, which removes the sclerotic scar bands containing thickened collagen and releases the contracted tissue through dermal remodeling. In the literature, the use of CO2 laser for the treatment of scars demonstrates the presence of improvement in texture and pigmentation. In the case described in the present report, improvement was observed in texture, pigmentation, contour, brightness and distortion. In addition, studies that have used higher densities led to better outcomes, which justifies the parameters chosen in the present case.5 Particularly for hypertrophic scars, positive outcomes can be observed in the reduction of scar’s firmness, and in the improvement of the surface and contractures.6
Likewise, microneedling stimulates the healing cascade, culminating with the formation of collagen type I. This purpose is achieved as long as the needles penetrate from 1-3 mm, in order to reach the dermis. Since only 50-70% of the total length of the needle penetrates during the rolling process, they should be at least 1.5mm long.2 Studies demonstrate that epidermal thickness can be increased by up to 205% by performing serial microneedling sessions. In addition, the dermal connective tissue becomes denser.7,8 The needle used in the present case (2mm long) was chosen aiming at inflicting deep injury to the dermis, which is indicated for the effective treatment of scars.2 Despite the length of needles was deemed adequate, the authors observed superior outcomes in the area treated with ablative fractional laser.
In the present case report, the authors observed superiority of outcomes with the use of CO2 fractional laser as compared with that of microneedling (2mm long needles) for treatment of a perioral traumatic scar. Nevertheless, this result requires further studies with a greater number of patients (randomized and blinded), as well as a great number of sessions, in order to ratify the findings. The authors also emphasize the possibility of performing drug delivery in the immediate post-procedure of both therapeutic modalities, provided that appropriate active principles and adequate formulation for the purpose are employed.
Célia Luiza Petersen Vitello Kalil | ORCID 0000-0002-1294-547x
Preparation of the manuscript, choice of procedures to be compared and of the laser’s parameters / needle length and roller. Revision of the written manuscript.
Clarissa Prieto Herman Reinehr | ORCID 0000-0003-1811-4519
Implementation of the laser and microneedling procedure, photographic records of the pre-treatment, immediate post- and late treatment. Literature review, writing of the manuscript.
Laura de Mattos Milman | ORCID 0000-0002-3249-0396
Literature review, writing of the manuscript.
Valéria Campos | ORCID 0000-0002-3350-8586
Preparation of the manuscript, choice of procedures to be compared and of the laser’s parameters / needle length and roller. Revision of the written manuscript.
1. Haedersdal M, Erlendsson AM, Paasch U, Anderson RR. Translational medicine in the field of ablative fractional laser (AFXL)-assisted drug delivery: A critical review from basics to current clinical status. J Am Acad Dermatol. 2016;74(5):981-1004.
2. Lima EVA, Lima MA, Takano D. Microneedling experimental study and classification of the resulting injury. Surg Cosmet Dermatol. 2013; 5(2):110-4.
3. Souza VM, Antunes JD. Ativos Dermatológicos: dermocosméticos e nutracêuticos. Ed. Especial 10 anos. São Paulo: Pharmabooks; 2013. vol. 1-8.
4. Beausang E, Floyd H, Dunn KW, Orton CI, Ferguson MW. A new quantitative scale for clinical scar assessment. Plast Reconstr Surg. 1998;102(6):1954-61.
5. Haedersdal M. Fractional ablative CO 2 laser resurfacing improves a thermal burn scar. J Eur Acad Dermatol Venereol. 2009;23(11):1340-1.
6. Poetschke J, Dornseifer U, Clementoni MT, Reinholz M, Schwaiger H, Steckmeier S, et al. Ultrapulsed fractional ablative carbon dioxide laser treatment of hypertrophic burn scars: evaluation of an in-patient controlled, standardized treatment approach. Lasers Med Sci. 2017;32(5):1031-40.
7. Zeitter S, Sikora Z, Jahn S, Stahl F, Strauß S, Lazaridis A, et al. Microneedling: Matching the results of medical needling and repetitive treatments to maximize potential for skin regeneration. Burns. 2014;40(5):966-73.
8. Aust MC, Reimers K, Kaplan HM, Stahl F, Repenning C, Scheper T, et al. Percutaneous collagen induction-regeneration in place of cicatrisation? J Plast Reconstr Aesthet Surg. 2011;64(1):97-107.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}