


Guilherme Moraes Kruger1; Gabriela Kimie Aseka1; Carlos Alberto Ferreira de Freitas2; Günter Hans Filho1
Received on: 07/07/2017
Approved on: 11/03/2018
This study was performed at the Dermatology Ambulatory of the Hospital Universitário Maria Aparecida Pedrossian, Universidade Federal do Mato Grosso do Sul (UFMS) - Campo Grande (MS), Brazil.
Financial support: None
Conflict of interests: None
Basal cell carcinoma (BCC), also known as basal cell epithelioma, is the most frequent epithelial neoplasm in the dermatological practice, being more common in men. The authors report the case of a 75-year-old female patient with a BCC in the concha, anti-helix and triangular fossa regions of the right ear. The lesion was completely excised, including the cartilage. The surgical defect was repaired by means of a "saloon door" flap, which yields good aesthetic and functional outcomes. The posterior auricular flap is a versatile option for partial reconstruction of defects in the ear.
Keywords: Carcinoma, basal cell; Skin neoplasms; Surgical flaps
Basal cell carcinoma (BCC), also known as basal cell epithelioma, is the most frequent epithelial neoplasm in Brazil, being more common in men. Its incidence increases in higher age groups, and it is estimated that in the last 30 years it has increased from 20% to 80%. The mean age at diagnosis is 68.1
Masson introduced the retroauricular island flap – also known as “saloon door” flap, revolving door flap, or flip flop flap – in 1972. Several authors later on modified the technique, and the indication for its use was extended for extensive auricular defects.
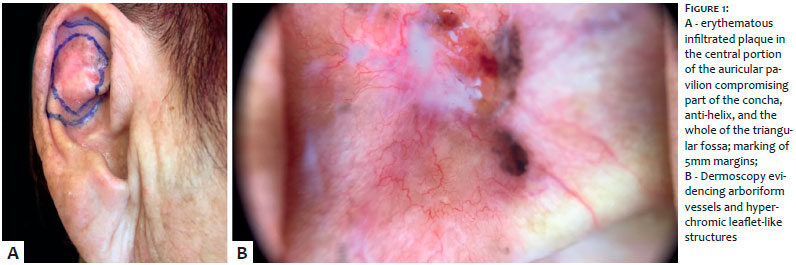
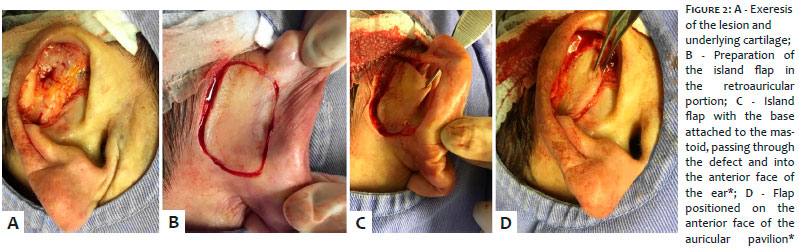
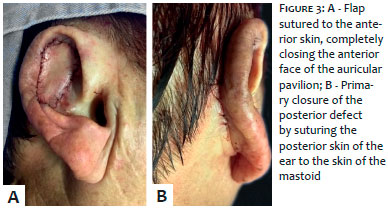
A 75-year-old female patient sought care describing the emergence of a lesion in the right ear’s concha roughly one year before. Physical examination showed an erythematous, infiltrated plaque in the central portion adhered to the cartilage. Dermoscopic examination revealed arboriform vessels and hyperchromic leaflet-like structures (Figure 1). A previous biopsy indicated the presence of BCC, nodular subtype. During surgery planning the lesion was marked using dermoscopy, with a 5mm margin. The flap was also marked in the retroauricular region. Local infiltrative anesthesia was used. The exeresis of the lesion and underlying cartilage were performed, followed by the creation of the island flap in the retroauricular portion and the rotation of the skin to the anterior portion (Figure 2). The flap was positioned and sutured. Subsequently, the posterior defect was closed (Figure 3). The sutures were performed in a single plane, with nylon thread and single stitches, which were removed 15 days later. Anatomopathological examination results confirmed that it was a nodular BCC with free margins. Healing occurred without intercurrences and good aesthetic and functional outcomes were observed after three weeks (Figure 4).
To reconstruct partial defects of the ear while preserving decreasing its size and changing its natural contour and shape has always been a challenge. In this location, in addition to the cure, it is necessary to attempt to preserve facial aesthetics. Alternatives to the reconstruction of the defects are: second intention closure, skin grafts, and wedge excision – all of which entailing the reduction of the auricular height.
Some studies have shown that when dermoscopy is used for demarcating the margins, there is a high rate of complete excision of the BCC (95% - 98.5%).6 Thus, it is critically important to demarcate the lesion’s margins via dermoscopy when micrographic Mohs surgery is not available.
The posterior auricular flap is a versatile option for the partial reconstruction of the ear defect. Planning, choosing an appropriate and individualized technique depending on the type of tumor, the location of the lesion and conditions of the patient are key to achieving a good aesthetic outcome.
Guilherme Moraes Kruger | ORCID 0000-0003-1296-2103
Design and planning of the study, intellectual participation in the propaedeutic and/or therapeutic approach of the case, revision of the manuscript, literature review and approval of the final version of the manuscript.
Gabriela Kimie Aseka | ORCID 0000-0002-5573-2378
Critical review of the manuscript.
Carlos Alberto Ferreira de Freitas | ORCID 0000-0003-2501-0128
Intellectual participation in the propaedeutic and / or therapeutic approach of the case, revision of the manuscript, literature review and approval of the final version of the manuscript.
Günter Hans Filho | ORCID 0000-0001-9324-3703
Critical review and approval of the final version of the manuscript.
1. Bolognia JL, Jorizzo JL, Schaffer JV. Dermatology. 3rd ed. Philadelphia: Elsevier; 2012. 1774 p.
2. Masson Jk. A simple island ap for reconstruction of concha-helix defects. Br J Plast Surg. 1972; 25(4): 399-403.
3. Talmi YP, Horowitz Z, Bedrin L, Kronenberg J. Auricular reconstruction with a postauricular myocutaneous island flap: flip-flop flap. Plast Reconstr Surg. 1996;98(7):1191-9.
4. Redondo P, Lloret P, Sierra A, Gil P. Aggressive tumors of the concha: treatment with postauricular island pedicle flap. J Cutan Med Surg. 2003;7(4):339-43.
5. Jackson T, Milligan I, Agrawal K. The versatile revolving door ap in the reconstruction of ear defects. Eur J Plast Surg. 1994;17:131-33.
6. Comparin C, Freitas CAF, Hans-Filho G. Dermatoscopy as a tool in the detection of presurgical margins of basal cell carcinomas. Rev Bras Cir. Cabeça Pescoço. 2013;42(1):47-52
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}