


Sergio Schalka1; Patrícia Camarano Pinto Bombarda2; Camila Canale3
Received on: 18/12/2016
Approved on: 28/02/2018
Study conducted at Medcin Pesquisa – Osasco (SP), Brazil.
Financial support: Laboratório Cristália, Itapira – SP, Brazil
Conflict of interests: The authors confirm they have no interpersonal, academic, political or financial interests in this manuscript
Introduction: The use of nutraceutical products in the treatment of chronic telogen effluvium of non-specific cause – associated or not with signs and symptoms of nail plate frailty – has been proposed in the literature. Supplementation of nutrients and trace elements that are crucial to follicle’s metabolism seems to be linked to this effect.
Objective: To evaluate the efficacy of a nutraceutical containing vitamins A, C, E and B complex, folic acid, iron, niacin, biotin, zinc and calcium pantetonate, among others, in the treatment of telogen effluvium associated with the brittle nails syndrome.
Methods: A clinical, prospective, open and monocentric study was carried out with the evaluation of 62 volunteers. Clinical evaluation measurements – based on digital phototrichogram and imaging – were performed at the baseline, and at 45 and 90 days after the use of the studied product.
Results: At the end of the study, a statistically significant (p <0.05) reduction of 31.56% in the number of telogen strands could be observed, coupled with a significant improvement in clinical parameters related to hair and nails. The instrumental evaluation based on image analysis showed a 36.63% reduction in nail desquamation, which, although not statistically significant, has shown benefits in the absolute outcome.
Conclusions: The use of nutraceuticals was proven effective in the treatment of telogen effluvium associated with the brittle nails syndrome.
Keywords: Alopecia; Dietary supplements; Nails
We can define hair disorders as any condition in which the visible hair coverage does not represent the normal parameters of growth.1 Normal parameters of hair growth vary according to gender, ethnic group, age and/or local culture.1
Diffuse hair loss is a condition as common as challenging for the dermatologist.2 There are numerous causes for the disorder, being telogen effluvium (TE) one of the most common.2-4
TE is an abnormality of hair cycle that results in excessive shedding of telogen hair.3,4 It’s actual incidence is uncertain, since many cases are sub-clinical.3 Common causes of TE include the use of medications, thyroid disorders and post-partum period. However, in a large number of cases it is not possible to find a cause.3-5
The activity of the hair follicle is cyclical, and scalp hairs have 10 to 30 cycles throughout life.3 In healthy individuals, hair grows approximately 0.35mm/day.4,6 Scalp hair density varies, with most people having between 100.000 and 150.000 hairs.3,7 We can shed 40 to 100 hairs on an average day and 200 to 300 hairs when the hair is washed.6 Hair growth occurs during the anagen phase; involution in catagen phase; and rest in telogen phase.3,4 Shedding of “dead” hair through the follicle (exogenous phase) occurs at the end of telogen phase of beginning of anagen.3 At the beginning of each anagen phase, a new hair is produced.3 On the scalp, 86% of hair is in the anagen phase (that lasts two to six years) and up to 13% in the telogen phase (that lasts three to six months).6 Catagen phase is transient, lasting three to six weeks, and 1% of hairs are in this phase.3,4,6
In TE there is a disturbance in the hair cycle, where a trigger precipitates the simultaneous transition of a large amount of anagen hairs into telogen hairs, which shed at the same time.4
The main complaint is hair loss.4 In view of the shedding, a complete and detailed history should be taken, inquiring about family history, use of medications, previous illnesses, recent surgeries and restrictive diets.4,6 We should request a full blood count, urinalysis, ferritin, thyroid hormones, levels of vitamin D and other vitamins, according to the history.7 Of the ancillary diagnostic follow-up methods for TE, the one considered most appropriate is phototrichogram performed by the device Trichoscan (TRICHOLOG GmbH, Freiburg, GER).
It is a non-invasive method that combines epiluminescence microscopy with the analysis of automatic digital imaging for the study of important hair parameters.7,8 It can analyze: hair density (n per cm2), hair shaft diameter (µm), growth rate (mm per day) and anagen/telogen ration.7,8 It is a very useful option in cases of diffuse alopecia, when we need to identify and quantify the response to the treatments used.
For the treatment of TE, besides eliminating the cause, supplementation of substances involved in the production of the hair shaft is particularly important.9 Since the hair is among the most metabolically active tissues in the human body, stimulation of the follicular metabolism can increase hair resistance to external harmful agents, besides stimulating hair growth.9
Vitamin and mineral supplementation for hair disorders has been used for a long time and has many reports in the literature.9,10 Special attention is given to micronutrients, a term that encompasses trace elements, minerals, vitamins and amino acids. Since hair shafts are formed by 98% of proteins, it is assumed that a diet rich in proteins is essential for their health. Indeed, in nutritional states when there is a deficiency in protein intake, hair shafts are clearly affected.
The use of vitamins, particularly of the B complex, is also described and there are many reports in the literature, with evidences of benefit in hair growth. Thiamine (vitamin B1) deficiency leads to beriberi, and one of the consequences is the production of fine hair. Vitamin B5 (pantothenic acid) is considered to be an ingredient that gives strength and flexibility to hair.9 It is suggested that zinc is one of the minerals responsible for the repercussion of hair fragility, subsequent to changes with protein deficiency,9 being also essential for the growth of annexes (hair and nails) since hair follicles maintain a significant metabolism with higher demand of nutrients. Biotin, or vitamin H, is a cofactor for many metabolic enzymes and has been used successfully for the treatment of animals with hair growth deficiencies.9 Even though the daily recommended dose is still unknown, there are reports that its supplementation provides benefits for the treatment of brittle nails and hair loss.9
Different studies evaluated the benefit of the use of vitamin supplementation in the treatment of telogen effluvium, with positive results.9,10
On the other hand, brittle nail syndrome (BNS) is a heterogeneous disorder, characterized by increased fragility of the nail plate. Nearly 20% of the population is affected, women twice as men.11-13 Association between TE and BNS is frequent, and it usually requires a combined approach from the dermatologist.
Most patients experience brittle nails as a significant cosmetic problem and a significant number report that these disorders are painful, affect daily activities and can have a negative impact on professional abilities.11-13
Hydration and delamination of the nail plate can change according to the seasons and play a significant role in certain occupations such as housewives, nursing and hairdressers, for whom repetitive immersion and drying of hands result in contraction and expansion of the nail, leading to splitting. In particular, occupational exposure to chemical products such as thioglycolates, cement, solvents, acids, alkalis, anilines, salt and sugar solution can dissolve intercellular lipids and damage intercellular adhesion, leading to splitting.11-13 Besides, cosmetic products, particularly nail polish and cuticle removers and procedures such as excessive use of manicure instruments can cause intercellular fractures. The interactive trauma of the nails (for example typing, dial phones, inadequate nail clipping and long duration of nails) can damage the nail plate and cause fractures.11-13
BNS treatment should take into consideration removal of the causal factors and use of nutraceuticals, that have been frequently advocated with good results.
This study evaluated the benefits of the use of a nutritional supplement (nutraceutical) for the treatment and TE and nail fortification.
The objective of this study was to evaluate in an open, non-comparative fashion the efficacy and safety of a nutraceutical compound for the treatment of chronic TE associated to BNS.
After approval by the Committee of Ethics in Research (CER), from May to October 2016, 68 female volunteers, aged between 18 and 45 years, with the complaint of diffuse and non-specific hair loss associated to brittle nails were recruited and included. All volunteers expressed their desire of participating in the study by signing a consent form before undergoing any of the procedures envisaged in the clinical protocol.
To assure the eligibility of the volunteers, besides populational characteristics they should also present, as a primary criterion for inclusion, rates of telogen hair on the centroparietal region higher than or equal to 20% determined by phototrichogram and could not meet any of the following criteria: pregnancy or risk of pregnancy, lactation, presence of alopecia areata or androgenetic alopecia, signs of specific nail disorders, history of nutritional deficiencies or hormonal disorders or any other systemic condition that could affect the hair and nails. No restrictive diet could have been commenced up to three months before the study. Hair treatments such as hair straightening and coloring in the previous three months would also be considered exclusion criteria.
Clinical evaluations were performed in the beginning (T0), in 45 days after beginning (T45) and in 90 days after beginning (T90), through a standardized scale to evaluate hair loss, density (scalp coverage), hair quality (flexibility, resistance to traction, tip breakage) and signs of nail fragility (plate splitting, diagonal splitting, ridges and furrows, longitudinal splitting and nail plate thinning). A four-point scale was used, where zero represented absence of abnormality and three maximum abnormality in each criterion.
The evaluation with phototrichogram is non-invasive and consists in capturing standardized images for the evaluation of hair growth.
Once the experimental area is defined, the device allows capturing micro images, with a standardized lens magnification of 20x of a 2cm diameter area, with the hair shaved. Reading of the micro image is performed by the software Trichoscan® Fotofinder (TRICHO- LOG GmbH, Freiburg, GER), device that issues reports with the following information:
Hair density: number of hairs per millimeter square;
Anagen hairs: indicates the percentage of growing hairs;
Telogen hairs: indicates the percentage of shedding hairs.
Nail images were registered using a specific support. Each image contains nails from the 3rd, 2nd and 4th fingers of both hands. Only one nail was chosen for the analysis.
Images were captured on the initial visit (before using the product being investigated) and after 90 days of the study (T90), from which the software Image Pro Plus® version 6 (Media Cybernetics, Rockville, EUA) analyzed the nail images, quantifying clear pixels and correlating them with the degree of desquamation.
The software calculated the accumulated histogram of the image with desquamation. The subsequent step was calculating the inflection point of the histogram, determined by the point of tangency of the lines at 45°. All pixels above the inflection point were considered desquamation areas.
The desquamation percentage was calculated according to the formula:
% desquamation = 100 * Px / Pt, where:
Px = number of pixels above the inflection point. Pt = number of total pixels of the image.
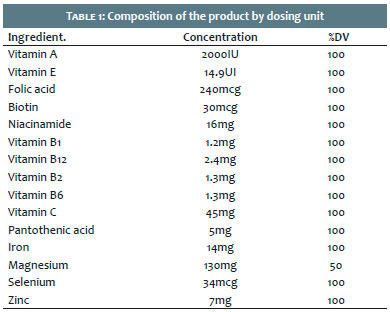
The nutraceutical product (Tacitá® Cristália, Itapira, SP, Brazil) is formed by vitamins A, B complex, C, E, folic acid, iron, niacin, biotin, zinc, calcium pantothenate, magnesium, selenium and lutein, among other micronutrients.
Table 1 shows the detailed formulation of the product studied.
They were provided by the sponsor for the study, 90 capsules by volunteers included in the study.
Each volunteer was instructed to take 1 capsule per day, during the 90 days of the study.
The age group of the volunteers included was from 19 to 45, with a mean age of 36 years.
Three volunteers did not return for the final assessment, what was considered loss to follow up.
Four volunteers had an adverse event during the study, which was mild and difficult to link to the use of the product. Three of these volunteers discontinued and their data were not considered in the efficacy evaluations. Data of 62 volunteers were considered population Per Protocol.
The primary criterion of efficacy was defined as being the reduction of the percentage of telogen hairs in the phototrichogram evaluation with Trichoscan®.
Secondary efficacy criteria were:
Increased percentage of anagen hairs in the phototrichogram
Increased hair density in the phototrichogram
Reduction of ungual desquamation by image analysis
Improved clinical parameters for hair evaluation
Improved clinical parameters for nail evaluation
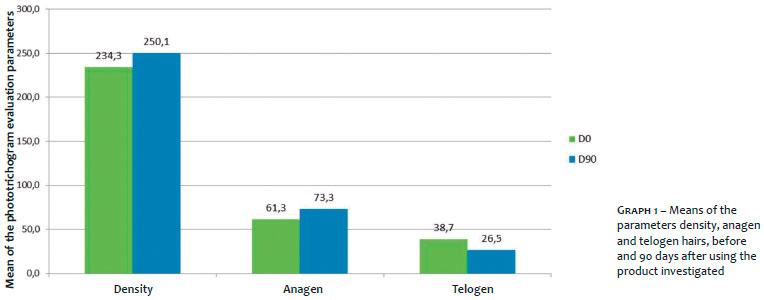
Graph 1 shows the mean evolution of the parameters: density, anagen and telogen hairs, initial evaluation (D0) and 90 days after using the product investigated (D90), in the phototrichogram.
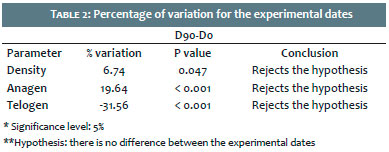
Table 2 shows the numerical values regarding the variation in percentage of the parameters evaluated in the phototrichogram, as well as statistical analysis performed using the Student T test.
Regarding the primary efficacy criterion, we could observe that there was a statistically significant reduction (p ≤ 0.05) in 31.56% of telogen hairs after continuous use of the product for 90 days.
Regarding secondary efficacy criteria evaluated by the phototrichogram, we observed that there was a 6.74% increase of hair density and 19.64% increase in anagen hairs, both also statistically significant (p < 0.05).
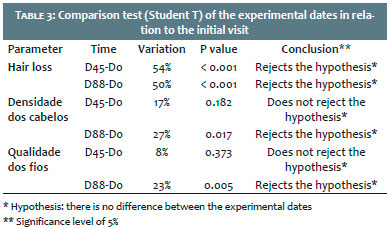
In the clinical evaluation and regarding hair loss, we observed a statistically significant improvement in three parameters evaluated (hair loss, quality and density) at 90 days. In the intermediate evaluation (45 days), only the parameter “hair loss” showed statistically significant improvement.
Table 3 shows the results of the clinical evaluation of parameters related to hair.
Regarding evaluation of nail desquamation using the imaging technique, a 36.63% reduction in median desquamation values was observed I the sample analyzed, between the initial and final date (T90).
Despite the representative values, due to sample dispersion, the statistical analysis with Wilcoxon test did not show significant differences between the initial and final date (p > 0.05).
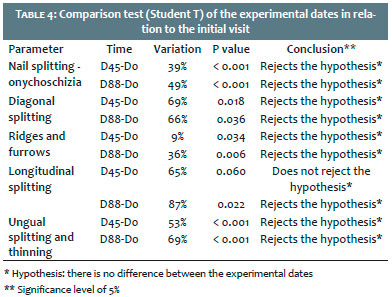
However, when we observe the results obtained by the clinical assessment performed by the medical investigators, we notice that the improvement was statistically significant (p < 0.05) in all parameters and all experimental dates, as seen in table 4:
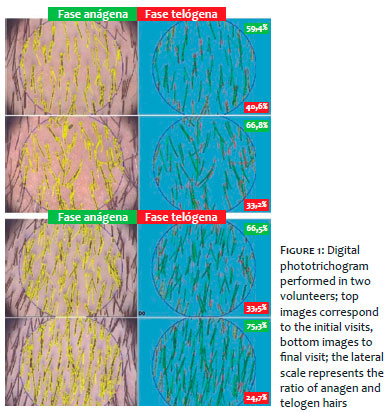
Figures 1 and 2 demonstrate examples of the results found in two volunteers with phototrichogram and nail photography, exemplifying how the efficacy criteria were evaluated.
Hair loss and brittle nails is a very common complaint in dermatological practice, many times presented in combination and resulting in psychological disturbances in the patients,2 most of them young women who are concerned about their cosmetic appearance.
When specific causes are ruled out, chronic, non-specific telogen effluvium and brittle nail syndrome can be responsible for the larger number of cases.3-5
After ruling out systemic conditions, treatment is mandatory. In these cases, oral supplementation with specific nutraceuticals for hair and nails is quite common among dermatologists, with a positive feedback to the patient.9,10
The association of vitamin and micronutrients is the most adequate choice in these circumstances, promoting restoration of depleted elements due to inappropriate diet that still has no obvious signs of clinically manifested deficiency.9,10
Nutraceutical compounds especially developed for the treatment of hair and nails are able to offer doses close to the dietary reference intakes (DRI) of essential vitamins, micronutrients and trace elements for the metabolism of hair and nails.9,10
The nutraceutical evaluated in this study has the goal of providing an adequate intake of these elements, preventing and treating the first signs of telogen effluvium associated to brittle nail syndrome.
The results obtained after 90 days of treatment were positive, demonstrating that the product tested was capable of statistically reducing the percentage of telogen hairs and, in the same way, increase the percentage of anagen hairs. Reversal of TE is characterized by this effect, with increased anagen/telogen ratio. Besides, clinical evaluations followed the same pattern, with statistically positive results for the three parameters evaluated.
Regarding the treatment for nail fortification, the results obtained were also positive. The evaluation with image analysis demonstrated a 36.63% reduction of desquamation of the nails evaluated and, even though not statistically significant due to data dispersion, the absolute result leaves no doubts of the benefit obtained. To confirm this positive action, clinical evaluations followed, with marked improvement for the items “diagonal splitting” and “longitudinal splitting”.
The use of the combination containing vitamins A, B complex, C, E, folic acid, iron, niacin, biotin, zinc, calcium pantothenate, magnesium, selenium and lutein demonstrated the ability of treating chronic TE associated to brittle nail syndrome, increasing the anagen/telogen ratio and improving the aspect of the affected nails, proving to be an adequate therapeutic option for the treatment of hair and nails.
Sérgio Schalka | ORCID 0000-0003-2425-7962
Principal investigator of the study, main author of the manuscript
Patrícia Camarano Pinto Bombarda | ORCID 0000-0001-5791-2631
Co-investigator of the study, contributed to data tabulation and statistical analysis, reviewed the manuscript
Camila Canale | ORCID 0000-0002-9548-7987
Co-investigator of the study, contributed to data tabulation and statistical analysis
1. Breitkopf T, Leung G, Yu M, Wang E, McElwee KJ. The basic Science of hair biology: what are the causal mechanisms for the disordered hair follicle? Dermatol Clin. 2013;31(1):1-19.
2. Shrivastava SB. Diffuse hair loss in an adult female: Approach to diagnosis and management. Indian J Dermatol Venereol Leprol. 2009;75(1):20-7.
3. Harrison S, Sinclair R. Telogen Effluvium. Clin Exp Dermatol. 2002;27(5):389-95.
4. Mulinari-Brenner FA, Bergfeld WF. Understanding telogen effluvium. An Bras Dermatol. 2002; 77(1):87-94.
5. Mounsey AL, Reed SW. Diagnosing and treating hair loss. Am Fam Physician.2009; 80(4):356-62.
6. Jackson AJ, Price VH. How to diagnose hair loss. Dermatol Clin. 2013;31(1):21-8.
7. Hoffmann R. TrichoScan: combining epiluminescence microscopy with digital image analysis for the measurement of hair growth in vivo. Eur J Dermatol. 2001;11(4):362-68.
8. Hoffmann R. Trichoscan: what's new? Dermatology. 2005;211(1):54-62.
9. Finner AM. Nutrition and hair: deficiencies and supplements. Dermatol Clin. 2013; 31(1):167-72.
10. Lengg N, Heidecker B, Seifert B, Truieb RM. Dietary supplement increases anagen hair rate in women with telogen effluvium: results of a double-blind, placebo-controlled trial. Therapy. 2007; 4(1):59-65.
11. Van de Kerkhof PC, Pasch MC, Scher RK, Kerscher M, Gieler U, Haneke E, et al. Brittle nail syndrome: a pathogenesis-based approach with a proposed grading system. J Am Acad Dermatol. 2005; 53(4):644-51.
12. Iorizzo M, Pazzaglia M, Piraccini BM, Tullo S, Tosti A. Brittle nails. J Cosmet Dermatol. 2004; 3(3):138-44.
13. Costa IMC, Nogueira LSC, Garcia PS. Brittle nail syndrome. An Bras Dermatol. 2007; 82(3):263-7.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}