


Paula Tavares Colpas1; Paulo Cesar Martins Alves1; Carolina Caliári Oliveira1; Ana Luiza Resende Pires2; Angela Maria Moraes2; Maria Beatriz Puzzi1
Received on: 08/01/2018
Approved on: 28/02/2018
Study conducted at Universidade Estadual de Campinas , Campinas - SP, Brazil.
Financial support: Fapesp, CNPq e Capes
Conflict of interests: None
Introduction: Juvenile dermatomyositis (JDM) is a systemic disease that affects children’s proximal musculature and skin. The ulcerated stage of the disease is a therapeutic challenge.
Objective: To evaluate the improvement of ulcerated stage of JDM caused by the use of cell therapy.
Methods: Co-culture of autologous fibroblasts and keratinocytes, application of these cells in ulcers in conjunction with fibrin glue, and placement of chitosan-alginate or chitosan-xanthan membrane on the lesions.
Results: Less than 12 hours after therapy, the patient reported complete cessation of pain and, within 2 days, healing tissue emerged. Some of the ulcers were almost completely healed by the end of the 1st week, and some of the calcinoses disappeared. This technique does not cure the disease, however it improves the patient’s quality of life, and it is possible to cryopreserve healthy cells to treat new lesions. Given the fact that the cells are of autologous origin, the risk of rejection is eliminated. Furthermore, this procedure does not require debridement of the lesions or hospitalization.
Conclusions: The application of autologous cultures of fibroblasts and keratinocytes in ulcers is already considered an effective treatment in patients with burns and other skin wounds, and has now also been proven effective in the treatment of wounds in JDM.
Keywords: Calcinosis; Cell-and tissue-based therapy; Dermatomyositis; Fibroblasts; Keratinocytes; Polysaccharides; Wound healing
Juvenile dermatomyositis (JDM) is a rare and severe systemic condition that affects primarily the proximal muscles and skin in children, with a prevalence of three per million in the population. Its etiology is not completely understood, but it is suggested that it is caused by an autoimmune reaction in individuals genetically susceptible to environmental triggers.1,2 JDM’s cutaneous manifestations can be severe and difficult to treat, with significant long-term morbidity.2,3
Calcinosis, characterized by the formation of calcium deposits in the skin, usually affects 10% to 70% of pediatric patients with JDM, being generally diagnosed in the first three years of the disease. Together with dermatomyositis itself, calcinosis can negatively impact in the patient’s quality of life, resulting in weakness, functional disability, muscular atrophy, cutaneous ulcers and, consequently, local pain and secondary infections.4 Dystrophic calcifications occur where there is tissue damage, with normal serum levels of calcium and phosphorus. Although they can appear in any part of the body, the areas most commonly affected are elbows, knees, trunk, hands, feet, buttocks and head. Calcinosis is usually painless; however, it can be associated to tenderness on palpation and pain with compression, evidencing panniculitis and ulcerations on histopathology. There is deposition of calcium on the skin surface, making it susceptible to infections.5
In juvenile dermatomyositis, the severity of the disease can be related to cutaneous calcinosis, delay in starting treatment and, potentially, to genetic polymorphisms of TNF-a-308. Despite the lack of data on the pathogenesis of calcinosis in JDM, a possible mechanism is calcium release from mitochondria of muscle cells affected by the myopathy. Macrophages, pro-inflammatory cytokines and defects in regulatory proteins of calcium were also suggested, as well as vascular ischemia, which also has a role in calcinosis. The deposition of calcium can occur in the subcutaneous tissue or in muscles and then ulcerate, draining a chalky substance. Ulcerated disease is severe and can be fatal, reflecting the importance of cutaneous vascular disorders, with tissue hypoxia and necrosis.1,3,6
As calcinosis tends to worsen with the progression of JDM, early and aggressive therapeutic approach has been suggested as an option to reduce cutaneous and muscular sequelae. Multiple medications have been used, such as corticosteroids, methotrexate, bisphosphonates, probenecid, warfarin, aluminum hydroxide, colchicine, diltiazem, infliximab, immunoglobulin, hydroxychloroquine, cyclophosphamide and thalidomide, but there is no consensus on the best therapy.1-5 Success of these medications is usually limited to disease control, with no extension to cure. Furthermore, side effects associated to their prolonged use can also worsen the patient’s health.
Since there is no gold standard nor a therapeutic algorithm to manage JDM and considering that repair of damaged skin is by proliferation and growth of dermal cells (essentially fibroblasts) and/or epidermal cells (keratinocytes and melanocytes), cell therapy can be a relevant alternative for the treatment of JDM associated to calcinosis. Promising results were reported with the use of cell therapy for the treatment of chronic ulcers of different etiologies;7-17 therefore, a positive result can could also be expected for this disease.
Biopolymers, of the polysaccharide and protein class, have been widely used in the development of interactive and bioactive dressings, being not only useful for protecting the wound, but also playing an important role in promoting healing. Formation of granulation tissue and reepithelization, followed by angiogenesis and continuous deposition of collagen fibers, limiting scar formation and tissue retraction, were seen with the use of chitosan, for example.18,19 The association of multiple polymers is also relevant, since it allows for the development of dressings with improved properties, such as enhanced fluid absorption. Relevant in vivo studies were described recently on the use of membranes manufactured by the association of chitosan with xanthan20 and alginate21 for the treatment of cutaneous ulcers in Wistar rats, with or without the combination or mesenchymal cells, demonstrating a potential that could be used as dressings in JDM lesions.
The objective of this study was to demonstrate an alternative therapy for the treatment of chronic ulcers in JDM patients with calcinosis that are not responsive to conventional treatments, using culture of autologous cells and subsequently covered with membranes of biocompatible polysaccharides.
This study was approved by the Committee of Ethics in Research of the Universidade Estadual de Campinas (Unicamp – CEP: 444.726).
A male, 18-year-old patient, diagnosed with JDM since 5 years of age, undergoing conventional treatment with methotrexate and corticosteroids, with universal calcinosis and chronic cutaneous ulcers, some with exposure of bone, was submitted to skin biopsy of a non-ulcerated on the right arm after signing a consent form. Fragments of approximately 2cm2 were collected and stored in saline, antibiotic and antifungal (Anti-Anti 15240, batch 577999, GIBCO/Invitrogen) until being transferred to culture jars. During the whole research, the patient maintained the previous systemic treatment.
The skin fragments were placed into culture jars with a keratinocyte medium (KSFM-GIBCO/ Invitrogen) supplemented with 10% of fetal bovine serum (FBS - LGC Biotechnology) and L-glutamine 0.2mg/ml, penicillin 100UI/mL and streptomycin 0.1mg/ml (GIBCO/Invitrogen), until processing. Subsequently, the fragments were transferred to Petri dishes with trypsin 2.5% and EDTA solution 0.1% (GIBCO/Invitrogen) and incubated at 37°C e 5% CO2 for 3 hours, when the dermis was separated from the epidermis. Trypsin was neutralized with a KSFM medium supplemented with 10% FBS. The supernatant (containing dermal and epidermal cells) was filtered (40mm Falcon/Corning) and centrifuged for 10 minutes at 400G.
The cell pellet was resuspended in culture medium and transferred to culture jars with a concentration of 1x105 cells/ml in 2ml of specific culture medium for each cell type and then incubated at 37°C and 5% CO2. Keratinocytes were cultivated in KSFM medium (KSFM-GIBCO/Invitro- gen) supplemented with 10% fetal bovine serum (FBS - LGC Biotechnology) and L-glutamine 0.2mg/ml, penicillin 100UI/ml and streptomycin 0.1mg/ml (GIBCO/Invitrogen). Fibroblasts were cultivated in medium 199 (Sigma-Aldrich), supplemented with 10% fetal bovine serum (FBS - LGC Biotechnology) and L-glutamine 0.2mg/ml, penicillin 100UI/mL and streptomycin 0.1mg/ml (GIBCO/Invitrogen). Culture media were changed three times per week. When the cells reached confluence, cultures were trypsinized with trypsin and EDTA solution for 10 minutes at 37°C and 5% CO2. As previously, trypsin was neutralized with fetal bovine serum 10%. This procedure was performed until a minimal amount was obtained for each cell type, approximately 5x106 keratinocytes and 10x106 fibroblasts. The whole process took between 21 and 30 days. Cells were cryopreserved in fetal bovine serum and DMSO solution at -80°C.
The whole process involving cell manipulation was performed in a clean room (class 10.000 ISO 7 - ISO 14644-1).
The preparation of membranes followed a technique already established at the Department of Material Engineering and Bioprocesses, Faculdade de Engenharia Química, Universidade Estadual de Campinas.
Membranes were obtained according to adaptations to methods established by Rodrigues et al.,22 Bueno and Moraes23 and adapted by Pires and Moraes,24 in the case of chitosan-alginate devices (C-A), based in procedures developed by Veiga and Moraes25 and Bellini et al.26 for the chitosan-xanthan membranes (C-X).
Chitosan with deacetylation degree of 96% (Sigma-Aldrich, batch number 109K0043V), medium viscosity sodium alginate from Macrocystis pyrifera (Sigma-Aldrich, batch number 058K0126), xanthan gum (Sigma- Aldrich, batch number 108K0038), glacial acetic acid, calcium chloride dehydrate and sodium hydroxide (Merck); besides, the water used was distilled and deionized in a Milli-Q system (Millipore).
Chitosan and alginate membranes were prepared with the addition of quantities of 180ml of 1% chitosan solution (m/v) dissolved in 2% acetic acid (v/v) in 360ml 0.5% alginate aqueous solution (m/v) at the flow of 200ml/h in the stainless steel reactor, maintained at 25°C, under stirring of 500rpm. After mixing the solutions, the stirring intensity was increased to 1000rpm for 10 additional minutes. Afterwards, 26ml of 2M NaOH aqueous solution were added to increase pH to 7, maintaining stirring for 10 more minutes. Afterwards, 7.2ml of 2% CaCl2 aqueous solution (m/v) were added to reticulate alginate carboxyls that did not form complexes with chitosan. The mixture obtained was deaerated for 120 minutes, transferred (in quantities of equal masses) into four polystyrene Petri dishes (diameter of 15cm) and dried in a dryer at 60°C for 6 hours. After drying, the membranes were immersed in 150ml aqueous solution of 2% CaCl2 (m/v) for 30 minutes for reticulation of free carboxyls leftover form alginate and then washed twice for 30 minutes with 200ml of deionized water. The final drying step was performed at room temperature for 24 hours.
In the case of chitosan and xanthan gum membranes, 200ml of aqueous solution of xanthan gum 1.5% (m/v) were added to 200ml of 1.5% chitosan solution (m/v) dissolved in 1.5% acetic acid (v/v) with a flow of 30ml/h, at 25°C and under stirring (1000rpm). After, the suspension was deaerated and the mixture was transferred into a polystyrene dish of 15cm diameter and the material was dried at 37°C for a variable period of 24 to 48 hours. The membrane was washed twice for 30 minutes with 200ml deionized water, once with 250ml of 10mM Hepes buffer (Sigma-Aldrich) to neutralize pH and, finally, with 500ml deionized water. A final drying step was performed at room temperature for 24 hours, securing the edges to prevent shrinking of the membrane.
The membranes were sterilized with Oxyfume 30 (30% ethylene oxide and 70% CO2) at 40°C for 8 hours, with relative humidity of 30% to 80% by the Central de Esterilização Comércio e Indústria Ltda - Acecil (Campinas, SP).
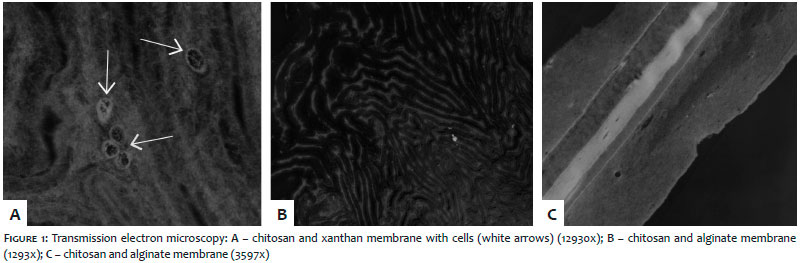
Transmission electron microscopy was performed to verify behavior of the cells in the membrane (Figure 1).
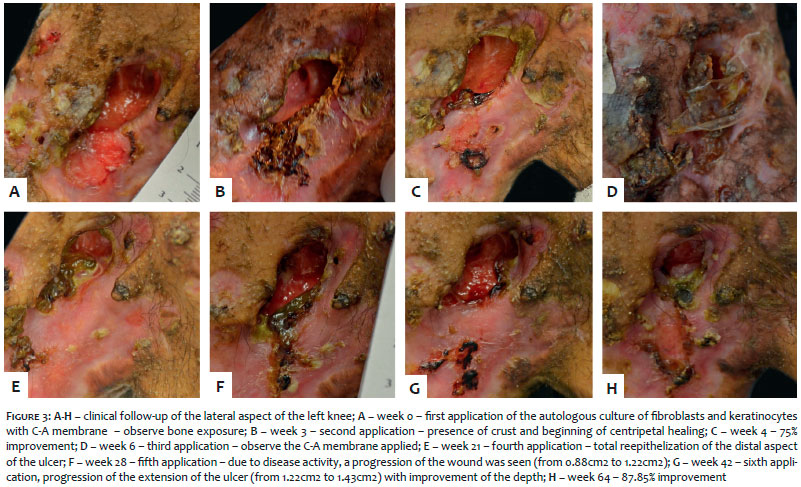
The cells were thawed and cultivated for at least 72 hours before application. On the day of application, the cells were trypsinized, washed and counted according to protocols previously described by Rehder et al.,13, Souto et al.,27,15 Bosnardo16 and Dinato et al.17 A culture of fibroblasts of a total of 1x107 cells was prepared. For the application, cells were sprayed with fibrin glue (Beriplast P – CSL-Behring) over the ulcer bed under antiseptic conditions, in an outpatient setting (Figure 2).
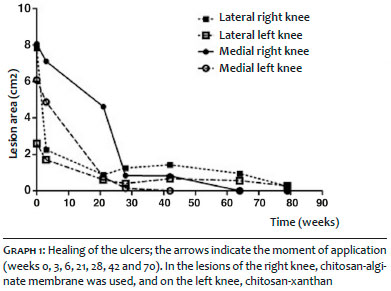
After spraying the cells, the polysaccharide membranes previously dilated with saline were placed on the ulcer (Figure 3), in order to protect the area against agents that could remove the graft, aiming at aiding the healing process.
The patient was followed for 20 months, every 7 days in the first month, and every 15 or 30 days thereafter. New applications were performed according to the patient’s response, in a total of 7. Photographic documentation was made with Nikon D5100 camera, using a ruler to determine the total area of the ulcer, delineating its borders. The images were processed with the software Image J2, and the differences in the values of the areas were determined for each ulcer using the software GraphPad Prism5.
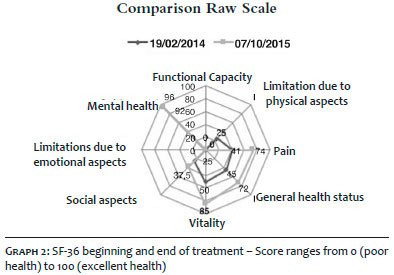
A quality of life questionnaire (SF-36) was also used before and at the end of the treatment.
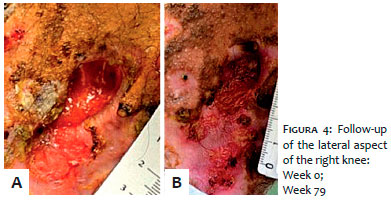
The patient had multiple cutaneous ulcers, ranging from 0.5cm2 to 8cm2, distributed all over the body but mainly on the lower limbs (Figure 2). The lesions selected for the treatment were the larger and the deeper, which caused more discomfort. The healing process was documented with photographs in weeks zero, 3, 21, 28, 42,64 (Figure 3) and 79 (Figure 4).
Less than 12 hours after the application of cells and membranes, the patient reported total improvement of the pain and, in two days, the healing process started. Soon thereafter, a shiny film was seen on the surface of the ulcers. Some days later, an intense exudate, attributed to fibrin, granulation tissue and crust was seen in some lesions, with subsequent centripetal closure. Some wounds were completely closed after one week of treatment.
A taxa de cicatrização alcançada foi acima de 95%, com melhora contínua, mesmo após cinco meses da última aplicação (Gráfico 1). O paciente não apresentou mais dores nas áreas tratadas, com importante melhora na qualidade de vida (Gráfico 2). É interessante notar que a calcinose desapareceu mesmo em áreas não tratadas diretamente.
The healing rate achieved was above 95%, with continuous improvement even after 5 months of the last application (Graph 1). The patient did not have any more pain on the treated areas, with significant improvement in quality of life (Graph 2). Interestingly, the calcinosis disappeared even in areas that were not treated directly.
JDM is a rare autoimmune disease that affects primarily the muscles and the skin. The main treatment is with high doses of corticosteroids combined to other immunosuppressant drugs. Approximately 30% of patients cannot control the disease, despite multiple interventions,1-5 as seen in our patient. The application of stem cells was described as a last resource in the treatment of patients with autoimmune diseases refractory to treatment but persistence of cutaneous disease, including calcinosis and contractures.28
Treatment of the ulcerated and refractory disease is very complex, and autoimmune diseases are quite challenging. Tissue engineering focused on autologous keratinocytes and fibroblasts has been used in the treatment of cutaneous ulcers since the 1980s. the technique was initially tested in burn patients, with good results. Then improved healing was seen in vascular and diabetic ulcers.16,17 In recent years, tissue engineering significantly advanced with this goal, and one of the trends in dermatology is the use of combined biomaterials with biopolymers and cells fulfilling biosafety requirements and that are active in the type of wound treated.20 Positive and relevant results were seen in our JDM patient after the application of autologous fibroblasts and keratinocytes, applied with fibrin glue, followed by the coverage with membranes made of chitosan with xanthan or alginate.
The protection provided by chitosan-alginate and chitosan-xanthan dressings with negative stimuli from the environment plays a role in the healing process. According to Wang et al.,29 the optimal dressing should be flexible and able to control local water loss. It must be resistant to bacterial infection therefore preventing sepsis, have adequate adherence on the ulcer, as well as not being antigenic, non-toxic and easy to apply and remove. From the engineering perspective, the material for the dressing should also have adequate mechanical properties so as to maintain its integrity during use.24 Rates of water evaporation are also important, both for maintaining adequate humidity in the wound bed and to avoid unwanted accumulation of secretions. Both membranes used in this study achieved this goal, being effective in the contribution to expedite tissue regeneration and promote speedy recovery. Besides, membranes are clear, which allows observation of the wound bed, without needing to be removed.
The complex chitosan-alginate seems to have a positive action in the process of tissue remodeling in scars, increasing the rates of collagen synthesis, while also improving compaction of new fibers and promoting the presence of mature firoblasts.29 Moreover, these membranes seem to stimulate and regulate multiple phases of the healing process,21 being useful in the treatment of cutaneous ulcers. Both collagen synthesis and modulation of wound contraction by chitosan-alginate membranes can result in a fast closure of the lesion.21 Similar results were seen on chitosan-xanthan membranes associated to mesenchymal cells.20
The role of fibrin glue is not clear in this case. The product is a biological adhesive that works by simulating the exudative phase of healing, frequently used in plastic surgery, as well as organ transplants. In this case, our hypothesis of its possible benefit is by the improved cell and membrane adherence to the lesions, and by its hemostatic and antibacterial actions.30-33 Under normal circumstances, soon after the injury, fibrin and fibronectin are deposited in the wound. There, fibrin acts as a hemostatic barrier, adhering tissue to surrounding cells and stimulating the migration of fibroblasts, what probably also occurred in this case. Redher et al.34 demonstrated that the application of fibrin glue alone, without cell culture, was not able to reepithelize the wound, despite crust formation. The authors did not mention reduction of the pain with this application.
Fibrin matrix releases growth factors, such as vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF) and transforming growth factor b (TGF-ß), and these proteins can be related to improvement of the pain, soon after beginning of treatment. Besides the antibacterial action, increased endothelial cell migration and proliferation can contribute to improved vascular supply and also provide an ideal environment for fibroblast and keratinocyte migration, proliferation and differentiation, improving healing.31
Improvement of calcinosis is not clear, and Köebener phenomenon was not seen after treatment started, not even in the biopsy site.
Cell therapy with autologous fibroblasts and keratinocytes was used in this study for a more effective treatment of ulcers in JDM patients with better functional and aesthetic results, as well as a faster recovery and elimination of pain, allowing the patient to return to his studies. The development of a strategy based on cell therapy represents a progress in the treatment of ulcers of different etiologies,17 and the use of C-A and C-X membranes associated to autologous cells is very advantageous because membranes can function as a physical barrier, preventing external contamination,20 besides having a possible role in healing. There was no difference of performance in the healing rates with different membranes.
The implants described here were effective when compared to conventional treatments of skin grafting with healthy donor sites,16,17,35 even if some ulcers did not completely heal, probably due to their extension and depth. Cell cultures can be cryopreserved and eventually used in a new application. Autologous cells are great candidates, because with them the risk of rejection is eliminated. Another positive aspect is not needing hospitalization or debridement of the lesions.
This was the first case described showing the use of cultures of autologous fibroblasts and keratinocytes associated to chitosan-alginate or chitosan-xanthan membranes for the treatment of cutaneous ulcers associated to juvenile dermatomyositis.
In this study, we demonstrated an effective strategy for the treatment of cutaneous disease caused by juvenile dermatomyositis, even though it was not completely cured. Maybe the combination of stem cell transplant with autologous cutaneous cells could be the cure for a patient like ours, who presents with extensive and debilitating disease. Although it as a sophisticated and restricted technique, it proved to be a valid therapeutic strategy that can be used in JDM and in ulcers with other etiologies.
Paula Tavares Colpas | ORCID 0000-0002-1389-0749
Main researcher of the article, responsible for literature review, writing, proofreading and final approval.
Paulo César Martins Alves | ORCID 0000-0002-6833-0343
Responsible for cell culture and manuscript review
Carolina Caliari Oliveira | ORCID 0000-0001-7906-9809
Responsible for cell culture and manuscript review.
Ana Luiza Resende Pires | ORCID 0000-0001-8247-6288
Responsible for the production of membranes and manuscript review.
Angela Maria Moraes | ORCID 0000-0002-5813-332X
Supervision and study review.
Maria Beatriz Puzzi | ORCID 0000-0001-8248-7884
Supervision and study review.
1. Batthish M, Feldman BM. Juvenile Dermatomyositis. Curr Rheumatol Rep. 2011; 13(3): 216-24.
2. Martin N, Li CK, Wedderburn LR. Juvenile dermatomyositis: new insights and new treatment strategies. Ther Adv Musculoskelet Dis. 2012; 4(1): 41-50.
3. Meher BK, Mishra P, Sivaraj P, Padhan P. Severe calcinosis cutis with cutaneous ulceration in juvenile dermatomyositis. Indian Pediatr. 2014; 51(11): 925-27.
4. Shinjo SK, Souza FHC. Update on the treatment of calcinosis in dermatomyositis. Rev Bras Reumatol 2013; 53(2):211-14.
5. Hoeltzel MF, Oberle EJ, Robinson AB, Agarwal A, Rider LG. The presentation, assessment, pathogenesis and treatment of calcinosis in juvenile dermatomyosistis. Curr Rheumatol Rep. 2014; 16(12): 467.
6. Valenzuela A, Chung L, Casciola-Rosen L, Fiorentino D. Identification of Clinical Features and Autoantibodies Associated With Calcinosis in Dermatomyositis. JAMA Dermatol 2014; 150(7):724-29.
7. Pruniéras M, Régnier M, Woodley D. Methods for cultivation of keratinocytes with air-liquid interface. J Invest Dermatol 1983; 81(Suppl 1): 28s-33s.
8. Régnier M, Patwardhan A, Scheynius A, Schmidt R. Reconstructed human epidermis composed of keratinocytes, melanocytes and Langerhans cells. Med Biol Eng Comput 1998; 36(6): 821-244.
9. Kim BM, Suzuki S, Nishimura Y, Um SC, Morota K, Maruguchi T, et al. Cellular artificial skin substitute produced by short period simultaneous culture of fibroblasts and keratinocytes. Br J Plast Surg. 1999; 52(7):573-78.
10. Bolívar-Flores YJ, Kuri-Harcuch W. Frozen allogeneic human epidermal cultured sheets for the cure of complicated leg ulcers. Dermatol Surg. 1999; 25(8):610-17.
11. Stock UA, Vacanti JP. Tissue engineering: current state and prospects. Annu Rev Med. 2001; 52:443-451.
12. Margulis A, Zhang W, Garlick JA. In vitro fabrication of engineered human skin. Methods Mol Biol. 2004; 289:61-70.
13. Rehder J, Souto LR, Issa CM, Puzzi MB. Model of human epidermis reconstructed in vitro with keratinocytes and melanocytes on dead de-epidermized human dermis. São Paulo Med J. 2004; 122(1):22-5.
14. Johnsen S, Ermuth T, Tanczos E, Bannasch H, Horch RE, Zschocke I, et al. Treatment of therapy-refractive ulcera cruris of various origins with autologous keratinocytes in fibrin sealant. Vasa. 2005; 34(1):25-9.
15. Souto LR, Rehder J, Vassalo J, Cintra ML, Kraemer MHS, Puzzi MB. Model for human skin reconstructed in vitro composed of associated dermis and epidermis. São Paulo Med J. 2006; 124(2):71-6.
16. Bosnardo CAF. Análise clínica prospectiva randomizada aberta, para o tratamento das úlceras de venosas, através da terapia celular com o enxerto de queratinócitos autólogos; comparada em dois grupos, associado ou não, a Diosmina Hesperidina Micronizada. [tese]. Campinas: Universidade Estadual de Campinas; 2010.
17. Dinato M, Puzzi MB, Rehder J, Batista F. Tissue therapy with autologous dermal and epidermal culture cells for diabetic foot ulcers. Cell Tissue Bank. 2012; 13(2): 241-49.
18. Muzzarelli RAA, Morganti P, Morganti G, Palombo P, Palombo M, Biagini G, et al. Chitin nanofibrils/chitosan glycolate composites as wound medicaments. Carbohydr Polym. 2007;70(3):274-84.
19. Muzzarelli RAA. Chitins and chitosans for the repair of wounded skin, nerve, cartilage and bone. Carbohydr Polym 2009; 76(2):167-82.
20. Bellini MZ, Caliari-Oliveira C, Mizukami A, Swiech K, Covas DT, Donadi EA, et al. Combining xanthan and chitosan membranes to multipotent mesenchymal stromal cells as bioactive dressings for dermo-epidermal wounds. J Biomat Appl. 2015; 29(8): 1155-66.
21. Caetano GF, Frade MA, Andrade TA, Leite MN, Bueno CZ, Moraes AM, et al. Chitosan-alginate membranes accelerate wound healing. J Biomed Mater Res B Appl Biomater. 2015; 103(5):1013-22.
22. Rodrigues AP, Sanchez EMS, Costa AC, Moraes AM. The Influence of Preparation conditions on the characteristics of chitosan-alginate dressings for skin lesions. J Appl Polymer Sci. 2008; 109(4):2703-10.
23. Bueno CZ, Moraes ÂM. Development of porous lamellar chitosan-alginate membranes: Effect of different surfactants on biomaterial properties. J Appl Polym Sci. 2011;122(1):624-31.
24. Pires ALR, Moraes ÂM. Improvement of the mechanical properties of chitosan-alginate wound dressings containing silver through the addition of a biocompatible silicone rubber. J Appl Polym Sci. 2015;132(12):41686.
25. Veiga IG, Moraes AM. Study of the swelling and stability properties of chitosan-xanthan membranes. J Appl Polym Sci. 2012;124(Suppl 1): E154-60.
26. Bellini MZ, Pires ALR, Vasconcelos MO, Moraes AM. Comparison of the properties of compacted and porous lamellar chitosan-xanthan membranes as dressings and scaffolds for the treatment of skin lesions. J Appl Polym Sci. 2012;125(Suppl 2): E421-31.
27. Souto LRM. Modelo de pele humana (Derme + Epiderme) Reconstruída In Vitro. [dissertação]. Campinas: Universidade Estadual de Campinas; 2005.
28. Enders FB, Delemarre EM, Kuemmerle-Deschner J, van der Torre P, Wulffraat NM, Prakken BP, et al. Autologous stem cell transplantation leads to a change in proinflammatory plasma cytokine profile of patient with juvenile dermatomyosistis correlating disease activity. Ann Rheum Dis. 2015; 74(1): 315-317.
29. Wang L, Khor E, Wee A, Lim LY. Chitosan-alginate PEC membrane as a wound dressing: assessment of incisional wound healing. J Biomed Mater Res. 2002; 63(5): 610-18.
30. Scardino MS, Swaim SF, Morse BS, Sartin EA, Wright JC, Hoffman CE. Evaluation of fibrin sealants in cutaneous wound closure. J Biomed Mater Res. 1999; 48(3): 315-21.
31. Currie LJ, Sharpe JR, Martin R. Use of fibrin glue in skin grafts and tissue- engineered skin replacements: a review. Plast Reconstr Surg. 2001; 108(6):1713-26.
32. Pérez-Guisado J, Gaston KL, Benítez-Goma JR, Cabrera-Sánchez E, Fidalgo- Rodríguez FT, Rioja LF, et al. Smoking and diabetes mellitus type 2 reduce skin graft take; the use of fibrin glue might restore graft take to optimal levels. Eur J Dermatol 2011; 21(6): 895-8.
33. Jeschke MG, Finnerty CC, Shahrokhi S,Branski LK, Dibildox M, ABA Organization and Delivery of Burn Care Committee. Wound coverage technologies in burn care: novel techniques committee. J Burn Care Res. 2013; 34(6):612-20.
34. Rehder J, Bosnardo CAF, Kraft MBPL, Frade MAC, Guillaumon AT, Batista FBX, et al. A comparative study of cell therapy and fibrin glue applied to chronic venous ulcers. Procedia Engineering 2013; 59: 85-91.
35. Gómez C, Galán JM, Torrero V, Ferreiro I, Pérez D, Palao R, et al. Use of an autologous bioengineered composite skin in extensive burns: clinical and functional outcomes. A multicentric study. Burns. 2011; 37(4): 580-89.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}