


Leandro Fonseca Noriega1; Leticia dos Santos Valandro2; Nilton Gioia Di Chiacchio1; Marina Lino Vieira1; Nilton Di Chiacchio1
Received on: 01/11/2017
Approved on: 02/01/2018
Study conducted at Hospital do Servidor Público Municipal de São Paulo - São Paulo (SP), Brazil.
Financial support: None
Conflict of interests: None
Viral warts are one of the most prevalent dermatoses. The clinical picture varies from a single lesion with spontaneous cure to multiple recalcitrant lesions. Bleomycin sulfate is a cytotoxic action drug approved for the chemotherapeutic treatment of some malignancies. There are a number of studies that have been carried out during the last 45 years demonstrating its usefulness in dermatology, especially in intralesional therapy for viral warts, meaning it is an excellent option for lesions in difficult-to-handle topographies and for cases that do not respond to other approaches.
Keywords: Bleomycin; Drug therapy; Viral wart
Bleomycin was originally isolated from the fungus Streptomyces verticillus, in 1962, by Umezawa et al.1 This glycopeptide has antibacterial and antiviral effects, however, it is very useful because of its cytotoxic effect. It was approved by the Food and Drug Administration (FDA) for systemic treatment of testicular carcinoma, malignant pleural effusion, Hodgkin and non-Hodgkin lymphoma. It was approved as adjuvant chemotherapy for the treatment of some advanced form of cutaneous squamous cell carcinoma.2-4
Despite not being approved for intralesional treatment, there are many case reports and studies in dermatology demonstrating efficacy and safety for the treatment of many conditions, such as viral warts, keloids, hemangiomas, vascular malformations and some malignant neoplasms (basal cell carcinoma, keratoacanthoma, squamous cell carcinoma and Kaposi sarcoma), for example.3,5,6
Knowing its low absorption when administered orally, intravenous, intramuscular or subcutaneous administration should be used in cases of systemic treatment, according to the approach protocol.3
Due to its low transepidermal absorption, a very high dose is required to achieve minimum tissue concentration when applied topically.3 Therefore, intralesional injection becomes an option for the treatment of localized lesions. It is considered that systemic absorption is minimal after one intralesional injection.7,8
James et al.9 dosed the serum level of bleomycin in seven patients with palmar viral warts after injection of one unit (U) of the drug. Serum concentration ranged from 7.5 to 113.5ng/ml and from 4.9 to 34.8ng/ml after 45 and 120 minutes, respectively.
It is mainly excreted through the kidneys, but liver participation is suggested.3,10 There is also enzymatic destruction with bleomycin hydrolase, enzyme found in many tissues, in varying concnetrations.3
It acts mainly via cleavage of the DNA strand. In the presence of oxygen, Fe2+ and a reducing agent, bleomycin transfer electrons from Fe2+ to oxygen, generating reactive oxygen species. The free radical causes oxidative damage to the nucleotides, cleaving the DNA strand.3 There is also degradation of cellular RNA.11 Another mechanism of action related to a good therapeutic response in viral warts is endothelial damage.11 Direct effect of bleomycin on human papillomavirus (HPV) was not described.
Because it is a hydrophilic substance, its permeability through the cell membrane is low. Mizuno e Ishida12 demonstrated that the association of bleomycin with lidocaine, procaine, tetracaine, dibucaine, butacaine or ethanol generates an increased cytotoxic effect. These substances would cause a disorganization of the cell membrane and, therefore, increased transmembrane permeability.3,12
The preparation commercially available is bleomycin sulfate, lyophilized powder, in vial/ampoule with 15U.3,4
Cutaneous viral warts are a common, benign skin infection, caused by HPV, that most frequently affects hands and feet (Figure 1).13,14 The presentation and severity can vary from a single lesion with spontaneous resolution to multiple, chronic lesions. They affect any age group, with a prevalence ranging from 5% to 30% in children and young adults.13-15
Immunosuppressed individuals are highly susceptible, with long standing lesions and reduced response to treatment.13,15 Besides aesthetic and functional limitations, we should bear in mind the association between HPV and cutaneous squamous cell carcinoma.15 Therefore, it is important to biopsy chronic verrucous lesions in adults, since they can represent malignant epithelial neoplasms.
Cryotherapy, salicylic acid, lactic acid, glutaraldehyde, imiquimod, electrocautery, surgical excision, curettage, podophyllotoxin, cantharidin, 5-fluorouracil (topical or intralesional), immunotherapy, photodynamic therapy and pulsed dye laser are described as therapeutic options.3,13,14
The site, size, number of lesions and previous treatment failures will influence the choice of therapeutic approach.
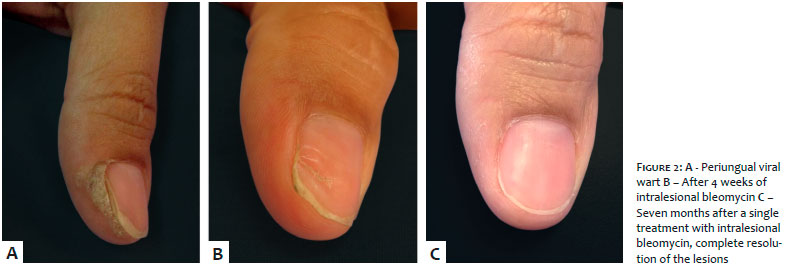
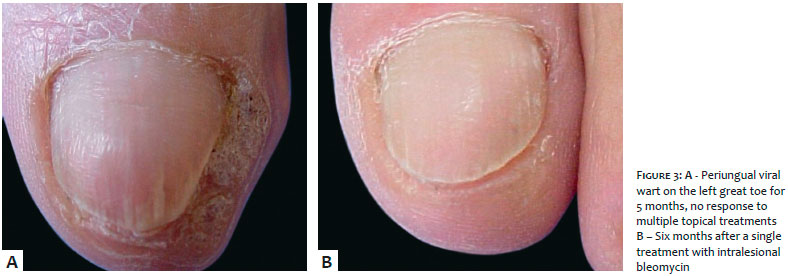
The first description of intralesional bleomycin for the treatment of viral warts was in the 1970s, and since then many studies have confirmed its efficacy and safety. For many authors, this is an excellent therapeutic option for difficult-to-approach sites, particularly the periungual region (Figures 2 and 3), and for recalcitrant lesions, even in immunosuppressed individuals.3,8,9,11,13,14,16,17
Dhar et al.18 assessed 73 patients between 5 and 50 years of age, with a total of 155 warts, comparing cryotherapy with intralesional bleomycin. The cure rate in the bleomycin group was of 94.9%; in the group treated with cryotherapy, 76.5%.
In a similar study, Adalatkhah et al.19 demonstrated cure in 86% and 68% of the cases treated with bleomycin and cryotherapy, respectively. Rossi et al.20 demonstrated a cure rate of 82%, 2.5-fold higher than in the placebo group.
Besides common and palmoplantar warts, there are studies showing efficacy for the treatment of anogenital warts, with a cure rate of up to 70%.21
Since intralesional bleomycin is a modality considered to be off-label, there is no standardized dilution. Most authors describe the use of this drug in varying concentrations, from 1 to 1.5U/ml:
15ml saline 0.9% for 15U bleomycin = 1U/ml.2
5ml distilled water for 15U bleomycin. Mix 1/3 of this solution with 2/3 2% lidocaine = 1U/ml.18,22
4 ml saline 0,9% + 6ml 2% lidocaine for 15U bleomycin = 1.5U/ml.21
The needle should be inserted at the base of the lesion and the injection continued until the local blanching is achieved.18,21 This is an important sign that the medication was correctly injected.3
Most articles mention that the ideal dose should range between 0.1 and 0.3U/lesion, and 3U is the maximum dose recommended per treatment. Usually, 2 or 3 treatments are required, every 3 or 4 weeks.3,18,21,23
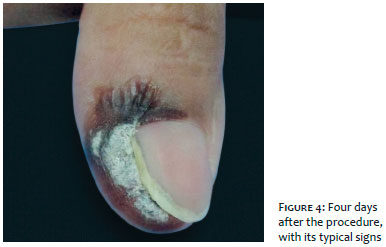
For lesions on the hands and/or feet, in the first week after the procedure, the formation of hematic and darkened crusts is expected. This is due to the absolute reduction in blood flow, which results in necrosis and subsequent disappearance of the lesion (Figure 4). In general, there is resolution in 2 to 4 weeks. Facial warts regress gradually and the lesions disappear without crust formation.3,11 Blood flow is probably reduced after injection; however, it is not completely blocked due to the rich vasculature of this area. Induction of endothelial apoptosis and direct keratinocyte injury can result in wart regression without necrosis or eschar.11
Application of a drop of bleomycin solution on the surface of the lesion, followed by multiple punctures is an alternative to intralesional therapy that was described as translesional multipuncture.4,15 Khalid et al.15 used this technique in 15 patients, using 0.1U/ml bleomycin solution and a 27G needle. The dose used ranged between 0.3 and 0.6ml per treatment. After 4 weeks, another treatment was performed in cases that persisted or recurred. They observed that 46.6%, 73.3% and 86.6% had a good response after 1, 3 and 6 months after the procedure, respectively.
Pain is one of the main limiting factors of this treatment, which can last up to 72 hours, with a peak at the time of injection.3 This would be one of the reasons why some authors use lidocaine as diluent, reducing pain during and immediately after the procedure.18,21-23
Other common side effects of the intralesional therapy with bleomycin are: erythema, edema, ulceration, hematic crust formation and eschars.2,3,16
Transient hypopigmentation or hyperpigmentation can occur (particularly in phototype IV, V or VI patients), atrophic or hypertrophic scars and hematomas. Less frequently, Raynaud phenomenon, digit necrosis, ungual dystrophy and loss of the nail were described after injection of periungual warts.2-4,8 Although rare, flagellate dermatitis can also occur with intralesional therapy.3,24
There are no reports of systemic complications with the use of intralesional bleomycin, except for flu-like symptoms, only described in the treatment of hemangiomas or vascular malformations.7,21,25
Options to reduce pain during intralesional injection3,26
Application of topical anesthetic or local injection
Using small diameter needles (27G or 30G)
Substitution of the needle when multiple punctures are necessary
Stretching or pinching adjacent skin
Applying ice or specific vibration devices
Inject slowly
Avoid a large volume by application area
Hypersensitivity or idiosyncratic reaction to the medication, Raynaud phenomenon, peripheral vascular disease, pregnancy (category D) and breastfeeding.3,27
There are no safety studies regarding intralesional use in the pediatric age group.3
Despite being described for many years as an effective and safe therapeutic approach for viral warts, intralesional injection of bleomycin remains an off-label option. Studies revealed a high cure rate even in cases refractory to other therapies, in lesions on difficult-to-handle sites and in immunosuppressed patients. Pain is the main limiting factor of this procedure.
We highlight the importance of histopathology in the evaluation of long standing verrucous lesions in adults, because they can represent a squamous cell carcinoma and not only a plain viral wart.
Leandro Fonseca Noriega | ORCID 0000-0002-2972-3718
Design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation
Letícia dos Santos Valandro | ORCID 0000-0002-2225-1973
Design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation
Nilton Gioia Di Chiacchio | ORCID 0000-0001-5944-7737
Design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation
Marina Lino Vieira | ORCID 0000-0002-0477-1406
Design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation
Nilton Di Chiacchio | ORCID 0000-0001-9536-2263
Design and planning of the study, preparation and writing of the manuscript, data collection, analysis and interpretation
1. Umezawa H, Maeda K, Takeuchi T,Okami Y. New antibiotics, bleomycin A and B. J Antibiot (Tokyo). 1966;19(5):200-9.
2. Yamamoto T. Bleomycin and the skin. Br J Dermatol. 2006;155(5):869-75.
3. Saitta P, Krishnamurthy K, Brown LH. Bleomycin in dermatology: a review of intralesional applications. Dermatol Surg. 2008;34(10):1299-313.
4. AlGhamdi KM, Khurram H. Successful treatment of periungual warts with diluted bleomycin using translesional multipuncture technique: a pilot prospective study. Dermatol Surg. 2011;37(4):486-92.
5. Jones CD, Guiot L, Samy M, Gorman M, Tehrani H. The Use of Chemotherapeutics for the Treatment of Keloid Scars. Dermatol Reports. 2015;7(2):5880.
6. Heller R, Jaroszeski MJ, Reintgen DS, Puleo CA, DeConti RC, Gilbert RA, et al. Treatment of cutaneous and subcutaneous tumors with electrochemotherapy using intralesional bleomycin. Cancer. 1998;83(1):148-57.
7. Payapvipapong K, Niumpradit N, Piriyanand C, Buranaphalin S. Nakakes A. The treatment of keloids and hypertrophic scars with intralesional bleomycin in skin of color. J Cosmet Dermatol. 2015;14(1):83-90.
8. Deshmukh NS, Belgaumkar VA, Mhaske CB, Doshi BR. Intralesional drug therapy in dermatology. Indian J Dermatol Venereol Leprol. 2017;83(1):127-32.
9. James MP, Collier PM, Aherne W, Hardcastle A, Lovegrove S. Histologic, pharmacologic, and immunocytochemical effects of injection of bleomycin into viral warts. J Am Acad Dermatol. 1993;28(6):933-7.
10. Dantzig PI. Immunosuppressive and cytotoxic drugs in dermatology. Arch Dermatol. 1974;110(3):393-406.
11. Lee JH, Burm JS, Yang WY, Kang SY, Byun SW. Treatment of Verruca Vulgaris in Both External Auditory Canals Using Bleomycin Injections. Clin Exp Otorhinolaryngol. 2015;8(3):295-7.
12. Mizuno S, Ishida A. Selective enhancement of bleomycin cytotoxicity by local anesthetics. Biochem Biophys Res Commun. 1982;105(2):425-31.
13. Kwok CS, Gibbs S, Bennett C, Holland R, Abbott R. Topical treatments for cutaneous warts. Cochrane Database Syst Rev. 2012;(9):CD001781.
14. Gibbs S, Harvey I, Sterling J, Stark R. Local treatments for cutaneous warts: systematic review. BMJ. 2002;325(7362):461.
15. Sterling JC, Gibbs S, Haque Hussain SS, Mohd Mustapa MF, Handfield-Jones SE. British Association of Dermatologists' guidelines for the management of cutaneous warts 2014. Br J Dermatol. 2014;171(4):696-712.
16. Ungureanu S, Martin-Clavijo A. Our experience in using bleomycin injection for resistant viral wart treatment. J Am Acad Dermatol. 2015; 72(5 Suppl 1): AB211.
17. Lewis TG, Nydorf ED. Intralesional bleomycin for warts: a review. J Drugs Dermatol. 2006;5(6):499-504.
18. Dhar SB, Rashid MM, Islam A, Bhuiyan M. Intralesional bleomycin in the treatment of cutaneous warts: a randomized clinical trial comparing it with cryotherapy. Indian J Dermatol Venereol Leprol. 2009;75(3):262-7.
19. Adalatkhah H, Khalilollahi H, Amini N, Sadeghi-Bazargani H. Compared therapeutic efficacy between intralesional bleomycin and cryotherapy for common warts: a randomized clinical trial. Dermatol Online J. 2007;13(3):4.
20. Rossi E, Soto JH, Battan J, Villalba L. Intralesional bleomycin in verruca vulgaris. Double-blind study. Dermatologia Revista Mexicana 1981;25(2):158–65.
21. Lee JY, Kim CW, Kim SS. Preliminary study of intralesional bleomycin injection for the treatment of genital warts. Ann Dermatol. 2015;27(2):239-41.
22. Soni P, Khandelwal K, Aara N, Ghiya BC, Mehta RD, Bumb RA. Efficacy of Intralesional Bleomycin in Palmo-plantar and Periungual Warts. J Cutan Aesthet Surg. 2011;4(3):188–91.
23. Nunley JR, Wolverton SE. Medicamentos Sistêmicos. In: Bologna JL, Jorizzo JL, Schaffer JV. Dermatologia. 3 ed. Rio de Janeiro: Elsevier; 2015. p. 3442-66.
24. Abess A, Keel DM, Graham BS. Flagellate hyperpigmentation following intralesional bleomycin treatment of verruca plantaris. Arch Dermatol. 2003;139(3):337-9.
25. Horbach SE, Rigter IM, Smitt JH, Reekers JA, Spuls PI, van der Horst CM. Intralesional Bleomycin Injections for Vascular Malformations: A Systematic Review and Meta-Analysis. Plast Reconstr Surg. 2016;137(1):244-56.
26. Park KK. Minimize that "pinch and burn": tips and tricks to reduce injection pain with local anesthetics. Cutis. 2015;95(6):E28-9.
27. BRASIL, Ministério da Saúde. Secretaria da Atenção à Saúde. Departamento de Ações Programáticas e Estratégicas. Amamentação e uso de medicamentos e outras substâncias. Brasília: Editora do Ministério da Saúde, 2010. 92 p.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}