


Bruna Dal Bello1; Fabiola Azevedo Genovez de Lima Leme2; Ana Flávia Salai1; Fernanda Santana1; Natalia Roberta Castellen1
Among the diverse reconstruction alternatives used in surgical wounds, those employing cutaneous grafts are implemented when the closure – primary or by second intention – is unfeasible or, due to other factors, flaps are not recommend. The repair of surgical wounds using partial thickness graft obtained from the scalp with a flexible blade is described in 3 cases of conventional exeresis (2 basal cell carcinomas in the nasal region and 1 case of squamous cell carcinoma on the dorsum of the hand). The technique yielded good aesthetic outcomes, both in the receiver and donor areas.
Keywords: dermatologic surgical procedures; skin neoplasms; scalp; carcinoma, basal cell; carcinoma, squamous cell; skin grafts
Non-melanoma skin cancer (NMSC) is the most common neoplasm in humans.1 It is estimated that 175,760 new cases occurred in Brazil in 2016.2The NMSC group comprises many types of tumors, among which the most common is carcinoma basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), corresponding to roughly 95% of the total.1
The main treatment for SCC and BCC is surgical excision, which avoids functional impairment and decreases the risk of metastases in SCC cases. There are several options for reconstruction of surgical wounds after excision of NMSC, the choice depending on the size and location of the final defect.3 The authors of the present study describe 3 cases of surgical reconstruction using partial thickness graft obtained from the scalp with a flexible blade after conventional excision of BCC and SCC.
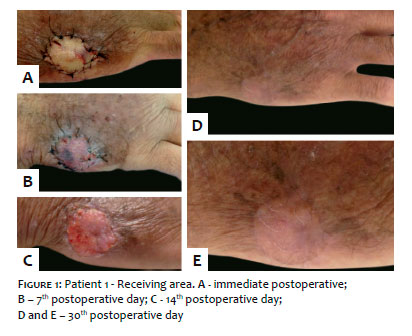
Eighty-year old male patient, phototype II, bearing an infiltrated hyperkeratotic plaque with an ulcerated center, measuring 2 cm, on the dorsum of the right hand. Histological diagnosis of SCC.
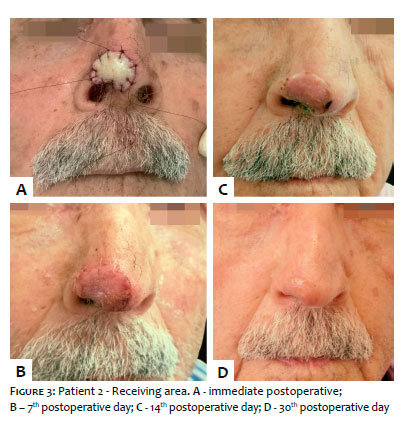
Ninety-three year old male patient, phototype II, with infiltrated erythematous-perlaceous papule, measuring 0,5 cm, located in the nasal tip, with histological diagnosis of solid, sclerodermiform and ulcerated BCC.
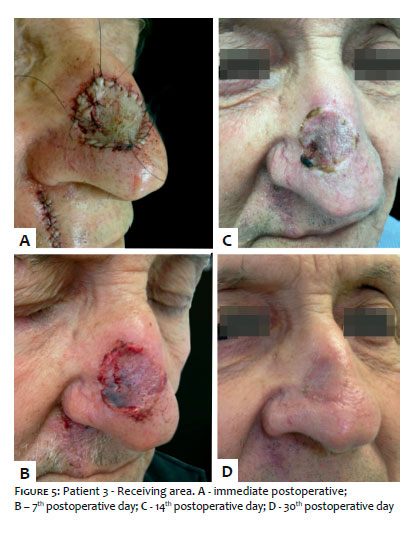
Eighty-one year old male patient, phototype II, bearing an infiltrated erythematous-ulcerated macula, measuring 1 cm, in the nasal dorsum, with histological diagnosis of solid and ulcerated micronodular BCC.
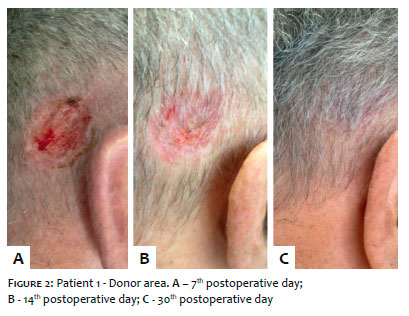
In all three cases, the marking and excision of the lesion was performed with standard margins, the closure was carried out using grafts. Likewise, the chosen donor area in all cases was the scalp’s retroauricular region (right retroauricular region in the first case, and left in the others). After measurement and marking of the donor site, the graft was removed with the shaving technique, using a Wilkinson® flexible blade. Next, it was sutured into the receiving area, and a Brown’s dressing was performed. Second intention closure was chosen for the donor area, using dressings with Aquaphor® (Eucerin, Brazil). Patients were instructed to use cephalexin for 7 days and analgesics, and return for follow-up at 7, 14 and 30 days after the surgery. The suture stitches and Brown’s dressing were removed on the 7th postoperative day, when it was possible to observe good adhesion of the graft to the receiving area and no signs of necrosis. At that moment, the scalp’s donor area already showed signs of repilation in all cases. Fourteen days after, the receiving area already presented a very positive aesthetic and functional result, with coloration similar to that of the peripheral area (Figures 1, 3 and 5). Complete repilation of the donor areas was observed 30 days later (Figures 2, 4 and 6). In none of the cases were there intercurrences during the immediate or late postoperative period. Anatomopathological examination of the third case revealed that the lateral margin was compromised by the neoplasia, entailing the need of new treatment.
Skin grafts are used when primary or second intention closures are not feasible and local cutaneous distensibility or other factors are prohibitive for the implementation of a flap. In the case of closure of wounds following tumor excision in conventional surgeries, grafts are especially interesting due to the fact it is possible to maintain the conformity of the surgical margins, which can be enlarged with greater precision should they are compromised by the neoplasia,3 as in the third case described.
Skin grafts can be classified according to their thickness. The partial thickness skin graft (PTSG) is composed of the epidermis and variable portions of the superficial dermis. Due to the fact that it is thinner, the PTSG is more likely to be adhered than the full-thickness graft variant (which contains the entire dermis).4 The technique for collecting the PTSG donor area can be compared to the technique for excision of tumor lesions in situ. In turn, in the excision of tumor lesions in situ in the scalp, the use of flexible blades showed benefit as compared to other techniques for it caused less bleeding and did not require the joining or suturing of the surgical edges, which could lead to scarring with alopecia.5 Other authors also consider second intention healing the most appropriate technique in cases of PTSG due to its superficiality.4
The scalp was first described as a donor area in 1963. Initially it was only used in cases where other donor sites were not available; nevertheless, its use was popularized due to the low rate of complications, the possibility for the same area to be used as a donor area more than once, and the rapid healing provided by the rich vascularization and presence of cutaneous attachments. Also due to profuse vascularization, the scalp may bleed more during graft collection as compared to other donor sites; however, the use of adrenaline in local anesthesia, soaked pads and occlusive dressings easily prevent bleeding.6
In addition to the fact that the donor area becomes imperceptible after local repilation, the scalp provides a good aesthetic outcome when transferred to the face, neck and extremities for wound closure, as it has good color compatibility with these sites.7 More recently, Hexsel et al. reported the aesthetic outcome in the receiving area of 39 patients who underwent PTSG originary from the retroauricular region with flexible blade for surgical wound closure in Mohs micrographic surgery. Good color compatibility was obtained in nasal, thoracic and extremity defects, probably due to the fact that the donor region was naturally protected by hair and ears, meaning that they had less intense chronic actinic damage.4 In the cases described, the results were also aesthetically satisfactory results already on the 30th postoperative day.
The complication rates linked to the scalp as a donor site are low, for although there are reports of alopecia, hair shaft transfer along with grafted skin, and hypertrophic scarring, these occurrences can be prevented if the correct graft thickness is not exceeded.8 Some electric surgical devices are capable of providing programmed and uniform graft thicknesses.9 However, the cost of the procedure is minimized by using a flexible blade, which should be handled as flat as possible during the removal of the graft aimed at ensuring thinness and uniformity to the piece.4
Hexsel et al. reported that the most common complication in the scalp PTSG receiving area is the emergence of inclusion cysts between 3 weeks and 3 months after the procedure, which has not been observed in the cases reported in the present paper. These cysts should be drained in order to avoid progression into pustules, however they do not usually prevent adhesion of the graft.4 Khalid et al. investigated how long it would take for the healing of the donor site to take place and the complications of 30 patients who underwent PTSG, where the scalp was the donor area. It was possible to observe that all patients experienced repilation of the donor site — 86% on the 6th postoperative day. The observed complications were: folliculitis in 2 patients and crust formation in 1 patient. None of the patients developed alopecia, hair transplantation to the receiving area or hypertrophic scar.6
Other studies evaluated the scalp as a donor area in burned children with good development of the healing process between 7 and 10 days after the procedure.8 The authors of the present paper also experienced these facts, with rapid repilation of the donor area and absence of complications in the 3 described cases.
The time during which dressings are necessary in the postoperative period, the practicality of performing them, and their little interference in the daily activities make the scalp a convenient donor site for PTSG, especially in elderly patients and children. 10 These were also reasons for choosing this type of graft.
We would like to thank Dr. Leonard H. Goldberg, who discussed and demonstrated this technique to Dr. Fabiola Leme during the Observer Fellowship at DermSurgery, Houston (TX), USA.
Bruna Dal Bello:
Writing of the manuscript and bibliographic survey. Assistant surgeon in the three reported cases
Fabiola A. Genovez L. Leme:
Surgeon. Provided guidance in the three reported cases
Ana Flavia Salai:
Surgeon in the 1st reported caseFernanda Santana:
Main surgeon in the 2nd reported case
Natalia Roberta Castellen:
Main surgeon in the 3rd reported case
1. Madan V, Lear JT, Szeimies RM. Non-melanoma skin cancer. Lancet 2010; 375(9715): 673-85.
2. Instituto Nacional de Câncer José Alencar Gomes da Silva. Tipos de Câncer: Pele não Melanoma. [Internet] Rio de Janeiro: Ministério da Saúde; [cited 2016 Out 24] Available from: http:// www.inca.gov.br/wps/wcm/ connect/tiposdecancer/site/home/pele_nao_melanoma
3. Silva LRTE, Ribeiro AMQ, Fleury Junior LFF. Surgical management of high-risk squamous cell carcinoma of the scalp: series of cases. Surg Cosmet Dermatol 2015; 7(2):166-70
4. Hexsel CL, Loosemore M, Goldberg LH, Awadalla F, Morales-Burgos A. Postauricular Skin: an excellent donor site for split-thickness skin grafts for thee head, neck, and upper chest. Dermatol Surg 2015; 41(1):48-52
5. Vergilis-Kalner IJ, Goldberg LH, Firoz B, Landau JM, Kimyai-Asadi A, Marquez D, et al. Horizontal excision of in situ epidermal tumors using a flexible blade. Dermatol Surg 2011; 37(2):234-6
6. Khalid K,Tarar MN, Mahmood F, Malik FS, Mohrose MY, Ata-ul-Haq. Scalp as a donor site for split thickness skin grafts. J Ayub Med Coll Abbotta-bad 2008: 20(1); 66-9
7. Finucan T, Budo J, Clarke JA. Partial thickness scalp grafts: clinical experience of their use in resurfacing facial defects. Br J Plast Surg 1984; 37(4):468-71
8. MacLennan SE, Kitzmiller WJ, Mertens D, Warden GD, Neale HW. Scalp autografts and hair transfer to the face in the burned child. Plast Re-constr Surg 1998; 102(6):1865-8
9. Zingaro EA, Capozzi A, Pennisi VR. The scalp as a donor site in burns. Arch Surg 1988; 123(5):652-3
10. Liebau J, Arens A, Kasten, Schwipper V. The scalp as a favorable donor site for limited-sized split-thickness skin grafts in comparison to the thigh donor site. Eur J Plast Surg 2004; 27(5):238-40.
This study was performed at the Faculdade de Medicina de Jundiaí - Jundiaí (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}