


Mariana Morais Tavares Colferai; Elizabeth Leocadia Fernandes; Denise Steiner; Gabriela Momente Miquelin; Camila Carneiro Marques; Kelly Cristina Signor
Kaposi's sarcoma is a rare multicentric neoplasm originating from endothelial cells, with cutaneous and extracutaneous manifestation. The present paper describes a case of an uncommon clinic variant of a Kaposi’s sarcoma in a 32 year-old male patient bearer of acquired immunodeficiency syndrome (AIDS), with regression after undergoing combined treatment with antiretroviral therapy and radiotherapy.
Keywords: sarcoma, kaposi; herpesvirus 8, human; acquired immunodeficiency syndrome; keloid
First described in 1872, Kaposi’s sarcoma (KS) is a rare multicentric neoplasm originating from endothelial cells with cutaneous and extracutaneous manifestation.1
The present paper reports the case of a patient bearer of a rare variant of epidemic KS — the keloidal variant — that receded under the combined treatment with antiretroviral therapy and radiotherapy.
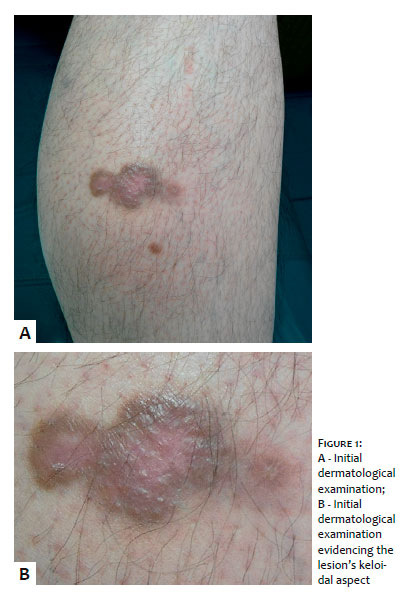
A 32-year-old Caucasian, single businessman, sought medical care describing the appearance of an asymptomatic lesion in the left lower limb roughly six months before, with progressive growth. He denied local trauma, as well as the use of systemic and topical medications. The patient had a history of disc herniation and allergy to acetylsalicylic acid, dipyrone and non-steroidal anti-inflammatory.
At the dermatological examination, he presented an erythematous-violaceous hardened nodule, painless on palpation, located at the inner region of the left leg (Figure 1).
Laboratory tests came out positive for HIV, with initial viral load of 378,000, CD4: 324 and CD8: 565.
On histopathological examination of the lesion (Figure 2), the epidermis showed rectification of epithelial ridges, superficial and deep dermis with numerous small vessels with collapsed walls and swelled endothelium, amid fusiform cells with evident nucleoli. It was possible to observe foci of extravasated erythrocytes, foci of hemosiderotic pigment deposition, multiple foci of mixed infiltrate, and interstitial fibrosis thickening. The diagnosis was compatible with KS.
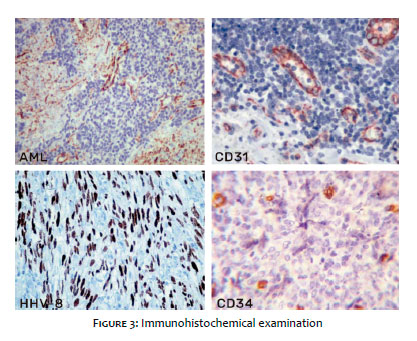
Immunohistochemical examination (Figure 3) showed positivity for smooth muscle actin (SMA), CD31, CD34 and herpesvirus 8.
Multidisciplinary follow-up was started at the oncology and infectology departments, as well as antiretroviral therapy. After 3 months of treatment, the patient coursed with viral load = 91, CD4: 503 and CD8: 933, however with only partial regression of the lesion. He then underwent 10 radiotherapy sessions, progressing with an important improvement. (Figure 4,)
After 2-year follow-up, the new histological examination of the lesion revealed absence of histological criteria for the diagnosis of KS.
Hungary’s Moritz Kaposi described 5 men with a type of uncommon multifocal skin sarcoma, which he called “multiple idiopathic pigmented sarcoma of the skin”. This pathological entity became known as Kaposi’s sarcoma (KS).2
Kaposi’s sarcoma is a multicentric endothelial tumor of low malignant potential, being considered rare up until the onset of the AIDS epidemic. Its incidence increased considerably from 1981, especially in male patients who have sex with men (HIV-associated epidemic KS). In 1994, the participation of a virus of the herpes group (HHV-8 or SKHV) in the pathogenesis of KS was discovered. More recent studies show the 3 most correlated factors in its etiopathogenesis: HIV infection, HHV-8 infection and the role of cytokines. From 1996, the introduction of combined antiretroviral therapy (Haart) in patients with HIV infection resulted in a significant reduction in the number of new cases of epidemic KS.
Since it was first described, the disease has been reported in 5 different clinical pictures with distinct clinical presentations, epidemiology and prognosis. The 5 subtypes are: 1) Classic KS, an indolent disease seen primarily in middle-aged men origi-nary from Southern or Eastern Europe; 2) African Endemic Cutaneous KS, a localized aggressive process affecting middle-aged individuals in tropical Africa; 3) African Endemic Lymphadeno-pathic KS, an aggressive disease affecting young patients, especially children younger than 10; 4) KS in patients immunosup-pressed by AIDS (epidemic); or 5) secondary to lymphoma or immunosuppressive treatment.3
It may be limited to the skin, nevertheless might involve the oral mucosa, lymph nodes and viscera. It may have indolent development, with only cutaneous lesions restricted to the lower limbs, or rapid progression, with extensive cutaneous and visceral lesions.
AIDS-associated KS begins with multiple nodules in the upper thorax, head, and neck, and rapidly progresses with dissemination to the skin and internal organs, leading to death.
The evolutionary clinical forms of presentation of KS are: 1) Macular KS, 2) KS in non-destructive localized plaque, 3) exophytic KS, 4) infiltrative KS, 5) generalized lymphadeno-pathic KS, 6) cutaneous and visceral KS, 7) KS telangiectatic, 8) keloidal KS, 9) ecchymotic KS and 10) cavernous or lymphangioma-like KS. Extracutaneous KS is more evident in the gastrointestinal tract, lymph nodes and lungs.4
Its histopathology varies according to the development of the lesions.
Macular lesions: there is proliferation of vascular spaces in the superficial dermis, lined by endothelial cells that separate the collagen bundles and are accompanied by a discrete infiltrate of lymphocytes and plasma cells.
Plaque lesions : the vascular changes reaches the deep dermis and subcutaneous, and fusiform cells arise that are positive for histochemical markers of vessels.
Nodular lesions: there is preponderance of fusiform cells with nuclear atypia and mitosis forming bundles; in the periphery, there are bizarre vascular spaces containing erythrocytes, which are also extravasated; there are macrophages containing hemosiderin amid lymphocyte infiltrates, plasmocytes, histiocytes and, occasionally, neutrophils.
The description of the keloidal variant is extremely unusual and limited to a 1994 report of 3 cases. The lesions are firm and rubber-like, and can be linear. Histologically, there is remarkable dermal expansion with dense and hyalinized collagen, with clear presence of keloids. The histological differential diagnosis includes a scar at the cutaneous biopsy site prior to any KS lesion. It is suggested that cytokines play a fundamental role in the development of the changes in keloidal stroma in this uncommon variant.5
Diagnosis is clinical and histopathological. Angiomas and other vascular tumors should be considered in the differential diagnosis. The disseminated forms of AIDS require differentiation vis a vis bacillary angiomatosis, angiomas, metastases, lichen planus, syphilis, melanocytic nevi and insect bites.6
Kaposi’s sarcoma has a good response to the different therapeutic strategies. Surgical excision, cryotherapy and radiotherapy can be used for localized lesions. Systemic treatment is indicated for larger, multiple skin lesions or when there is involvement of viscera. Among the available treatments, chemotherapy is used to on both cutaneous and visceral lesions in cases of disseminated disease. There are several active chemotherapeutic agents with variable response rate (60 to 80%), among them are: liposomal anthracyclines (doxorubicin, daunorubicin), pacl-itaxel and vinblastine, and etoposide. Interferon immunotherapy can be indicated in selected cases.1 The introduction of highly active antiretroviral therapy, allowing immunological reconstitution of HIV-infected patients, has had a profound impact on KS associated with this infection, significantly decreasing its occurrence; when introduced in patients with HIV and KS, it also enables tumor regression.6
Mariana Morais Tavares Colferai:
Bibliographic review, manuscript preparation and submission
Gabriela Momente Miquelin:
Bibliographic review, manuscript preparation
Elizabeth Leocadia Fernandes:
Guidance, discussion and review of the manuscriptDenise Steiner:
Guidance and final review
Kelly Cristina Signor:
Photographic records and correction of images
Camila Carneiro Marques:
Bibliographic review and spelling review
1. Ohe EMDN, Padilha MHVQ, Enokihara MMSS, Almeida FA, Porro AM. Fatal outcome in classic Kaposi's sarcoma. An Bras Dermatol. 2010;85(3):375-9.
2. Bolognia JL, Jorizzo JL, Rapini RP . Dermatology. 2nd ed. Rio de Janeiro: Elsevier; 2011.
3. James WD, Berger TG, Elston DM. Andrews' diseases of the skin: clinical dermatology. 10th ed. Rio de Janeiro: Elsevier; 2007.
4. Belda Junior W, Di'Chiacchio N, Criado PR. Tratado de Dermatologia. Vol 1. São Paulo: Editora Atheneu; 2010.
5. Grayson W, Pantanowitz, L. Histological variants of cutaneous Kaposi sarcoma. Diagn Pathol. 2008; 3:31
6. Sampaio SAP, Rivitti EA. Dermatology. 3rd ed. rev. e ampl. São Paulo: Artes médicas; 2007.
This study was performed at the Universidade de Mogi das Cruzes - Mogi das Cruzes (SP), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}