


Sandra Tagliolatto1; Aldo Toschi2; Tania Maria Henneberg Benemond1,3; Suzana Lu Chen Wu3; Vania Marta Figueiredo Yokomizo1,3
Cryolipolysis is known worldwide as an effective and safe treatment for the reduction of localized body fat. A review of the current literature on the subject was carried out, including possible complications of the technique.
Keywords: cryotherapy; adipose tissue; therapeutics
Cryolipolysis is the non-invasive cooling of the fat cells to induce lipolysis without damaging other types of tissue.1,2
The studies began in 1997, from the report of clinical cases with the possibility of reduction of the fat layer in case the area was submitted to low temperatures. The first repot showed reduction of the cheek fat in children who ate posicles (popsicle panniculitis), and the second study demonstrated the same effect on the thighs of people who went horse riding in very low temperatures (equestrian cold panniculitis).3-5
Therefore, the mechanism is based on the idea that cooling triggers the natural death of fat cells, i.e., apoptosis, considered the natural, ordered and gradual process in which the cellular membrane is maintained intact and there is absence of the healing response.1
The first studies could show a reduction in the fat layer in animal models. A reduction of the thickness of the fat layer in pig’s skin was demonstrated 90 days after the procedure of cryolipolysis.5,6
The concept of selective cryolipolysis is also important: fat cells are more susceptible to cold than cells in the skin, nerves, or muscles. Therefore, the procedure can be performed to eliminate fat cells without compromising adjacent tissues.1,2
In 2010o FDA approved the cryolipolysis device (CoolSculpt-ing® — ZELTIQ Aesthetics Inc. — Pleasanton — CA-USA) for the reduction of the fat in flanks and abdomen. Throughout the years, the procedure was also approved for other body areas.1,7
Over time, many devices of different companies and nationalities appeared in the market. They are all similar and the devices as a rule have a concave applicator with two cooling plaques, to where the fat is sucked and submitted to low temperatures for a set time, in order for lipolysis to occur. Nowadays, some devices offer the possibility of treatments in two areas at the same time.
It is worth highlighting that only the devices certified as safe for the application of cryolipolysis by the Agência Nacional de Vigilância Sanitária (Anvisa) can be commercialized in Brazil.
The tissue to be treated is sucked by a moderate vaccum inside the applicator, becoming in contact with both cooling plaques.
In most devices, the temperature is modulated by thermoelectric elements and controlled by sensors that monitor tissue temperature during the whole treatment, which lasts approximately 60 minutes.1,7
The technique is similar for all devices, being necessary the use of a protection blanket over the skin before the tip is positioned. At the end of the cycle, soon after removal of the applicator, the area must be massaged for 2 minutes, practice that has a direct impact in the final result.1
The procedure is indicated for the treatment of localized, well-defined fat buildups with visible limits, with a sufficient amount to fill the cavity of the applicator. A minimum of a 2.5cm fold in the adipometer and the overlying skin should be intact.8
The most common treatment areas are the upper and lower abdomen, the flanks and the fat buildups on the back. However, over time, the areas of application have widened, with the development of new tips such as those used on the internal aspect of the thighs, buttocks, arms and chin.
To achieve the desired results, a global evaluation of the potential treatment areas should be performed. Treatment plan can contemplate many cycles and session on a specific area.1
This approach makes it possible to treat patients with larger deposits of fat and leads to more satisfactory results.
The number of treatment cycles depends on the volume of the region; however, the same area can only be submitted to a new treatment session after 8 weeks, time necessary for the resolution of the inflammatory process.
It is important to tell patients that the results can take up to 2 to 3 months to be noticed, time necessary for the elimination of the lipids by macrophage phagocytosis.1,8,9
The technologie is contraindicated: in patients with a diagnosis of cold-related conditions such as cryoglobulinemia, paroxysmal cold hemoglobinuria, cold urticaria and Raynaud phenomenom. It should also be avoided in patients with a hernia on the treatment area, pregnant women and if, on the target area, scars or infections ca be seen.1,6
Few side effects are reported with the technique when adequately performed (adequated skin fold, patients with none of the contraindications mentioned above, use of the protective blanket, massage after the procedure.1
Studies demonstrate that there are no changes in the cholesterol, triglycerides or liver function changes, and no long-lasting sensory change was seen.10-12
The most commonly reported side effects were mild to moderate pain and sensory changes that can persist for 2 to 3 weeks. Erythema and hematoma can occur due to the suction. Edema on the treated area can perist for up to 4 weeks.8
Colics and muscle spasms were reported.
More rarely, a prolonged loss of sensation can occur (3 to 6 weeks).
Intense late-onset pain is reported with a prevalence of 0.1%,7 14 days after the procedure, with a duration of up to 20 days.
There are also reports of fainting during the treatment.1
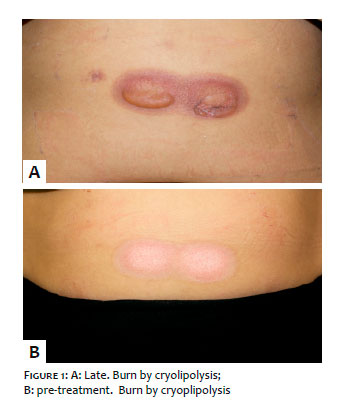
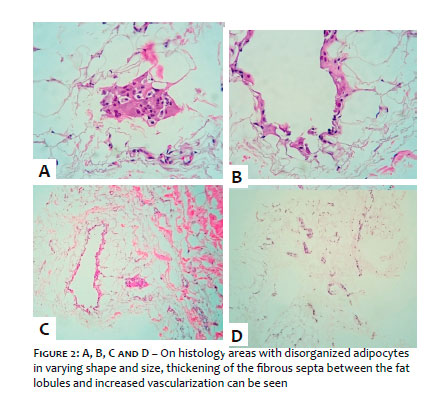
Paradoxal fat hypertrophy has been described with an estimated frequency of 0.0051%. it usually begins 2 to 3 months after the treatment. There is initial reduction in the volume of the area treated, followed by an increase in volume, that stabilizes 5 months after the treatment, leading to a bulge on the site with the shape of the applicator. The skin remains unchanged in appearance but with a hardened and “rubbery” texture (Figures 1 A and B). No common characteristics were identified in the cases, with reports of the occurrence in the flanks, abdomen and upper back, with a higher incidence in males. On histopathology examination, areas with disorganized adipocytes, with varying shape and size, thickening of the fibrous septa between the fat lobules and increased vascularization are seen. Even though the cause is still not established, many etiopathogenic hypothesis have been suggested: hypertrophy of preexisting adipocytes, recruitment of pre-adipocyte populations and/or stem cells, altered expression of receptors or factors associated to the metabolism of adipocytes, damage associated to hypoxia. Hypoxia will lead to the realease of factors that will trigger the angiogenesis cascade and the increase in capillaries and possibly fat hyperplasia. The thickening of the septa is due to reactive fibrosis from adipocyte damage.1,9,12-14 (Figures 2 A, B,C and D)
The rates of satisfaction with cryolipolysis are higher than with other non-invasive technologies for the treatment of localized fat.
Clinical studies demonstrate an approximate reduction of 25% in the thickness of the fat layer after one cycle of treatment.1,9,13,14
Approach on the subject by the Grupo de Estudos em Tecido Subcutâneo.
In the Brazilian Society of Dermatology, Regional São Paulo (SBD-Resp), many study groups are active, made of members with specific interests, among them the “Grupo de Estudos emTecido Subcutáneo” (Study Group in Subcutaneous Tissue), whose members devised this publication, making some consideration regarding the treatment of localized fat with cryolipolysis, as follows.
Lipoaspiration and its variants such as laserlipolysis, provide more satisfactory results in the reduction of localized fat when compared to non-invasive technologies; and, if performed adequately, under Klein tumescent anesthesia, offer few risks and adverse effects.
However, it can be considered that in terms of non-in-vasive equipments for the treatment of fat deposits, cryolipolysis seems to be the mechanism with best performance so far.
However, we must point out that, although cryolipolysis is classified as a non-invasive treatment, asdverse events can occur, particularly when non-adequate devices are used and/or when unskilled professionals perform the technique, in particular without following the safety measures, such as the use of the protection blanket, for example.
The vulgarization of the method is of concern, since good devices require a higher investment. There is also the need for medical follow-up, because possible side effects as those above-mentioned can occur, which is many times neglected.
Possibly, the burns on the skin and subcutaneous tissue reported seem to have been caused by the incorrect application of the technique and not by the method itself, since they are not reported as adverse events in the medical literature. (Figures 3 A and B).
Another situation ot be discussed is the need for multiple sessions (in the same area ou in contiguous areas) to enhance the results; however, the increased costs of the therapy might make the method impracticable, affecting the end result, particularly if the device used requires the use of “disposables”.
Finally, the Grupo de Estudos em Tecido Subcutáneo/ SBD-Resp classifies this technology as effective for the treatment of localized fat but has some reservations regarding real expectations in relation to results. We highlight that the current methodology proposes the application of the method in different areas to obtain better results, making the procedure costly and many times making its best use impossible, with a direct impact on the final result. The group also considers cryolipolysis safe but emphasizes that the technique should be strictly followed, both for the indication (minimal skin fold, patients with no cold-related conditions, hernias or other conditions that preclude the method) and for the execution of the procedure (use of protective blanket, for example). Lastly, we emphasize that it is an intervention that, although not frequent, is subject ot adverse effects and, therefore, the presence of a physician in the indication, execution and follow-up of the treatment is necessary.
Sandra Tagliolatto
Literature research, elaboration of the text, organization of the article and photos, submission of the article
Aldo Toschi
Elaboration of the text about the approach of the subject by the grupo de estudos do tecido subcutáneo
Tania Maria Henneberg Benemond
Suggestions in the elaboration of the text
Suzana Lu Chen Wu
Clinical and histologic about complications of the method (paradoxal hyperplasia and burn)
Vania Marta Figueiredo Yokomizo
Suggestions in the elaboration of the text
1. Krueger N, Mai SV, Luebberding S, Sadick NS. Cryolipolysis for nonin-vasive body contouring: clinical efficacy and patient satisfaction. Clin Cosmet Investig Dermatol. 2014; 7: 201-5.
2. Avram MM, Harry RS. Cryolipolysis for subcutaneous fat layer reduction. Lasers Surg Med. 2009; 41(10):703-8.
3. Epstein EH Jr, Oren ME. Popsicle panniculitis. N Engl J Med 1970;282(17):966-967
4. Beacham BE,Cooper PH, Buchanan CS,Weary PE. Equestrian cold panniculitis in women. Arch Dermatol. 1980; 116(9):1025-7
5. Manstein D, Laubach H, Watanabe K, Anderson RR (2008) A novel cryotherapy method of non-invasive, selective lipolysis. Lasers Surgery Med Suppl 40(S20): 104 11/08
6. Zelickson B, Egbert BM, Preciado J, Allison J, Springer K, Rhoades RW, et al. Cryolipolysis for noninvasive fat cell destruction: initial results from a pig model. Dermatol Surg. 2009;35(10):1462-70.
7. Jalian HR, Avram MM, Garibyan L, Mihm MC, Anderson RR. Paradoxical adi- pose hyperplasia after cryolipolysis. JAMA Dermatol. 2014; 150(3): 317-19
8. Nelson AA, Wasserman D, Avram MM. Cryolipolysis for reduction of excess adipose tissue. Semin Cutan Med Surg. 2009;28(4): 244-9
9. Garibyan L, Sipprell WH 3rd, Jalian HR, Sakamoto FH, Avram M, Anderson RR. Three-dimensional volumetric quantification of fat loss following cryolipolysis. Lasers Surg Med. 2014;46(2):75-80
10. Klein KB, Zelickson B, Riopelle JG, Okamoto E, Bachelor EP, Harry RS, et al. Non-invasive cryolipolysis for subcutaneous fat reduction does not affect serum lipid levels or liver function tests. Lasers Surg Med. 2009;41(10):785-90
11. Klein KB1, Zelickson B, Riopelle JG, Okamoto E, Bachelor EP, Harry RS, Preciado JA. Non-invasive cryolipolysis for subcutaneous fat reduction does not affect serum lipid levels or liver function tests.
12. Coleman SR, Sachdeva K, Egbert BM, Preciado J, Allison J. Clinicl efficacy of non-invasive cryolipolysis and its effects on peripheral nerves. Aesthetic Plast Surg. 2009; 33(4):482-8
13. Dierickx CC, Mazer JM, Sand M, Koenig S, Arigon V. Safety, tolerance and patient satisfaction with noninvasive cryolipolys. Dermatol Surg. 2013; 39(8):1209-16
14. Stevens WG, Pietrzak LK, Spring MA. Broad Overview of a Clinical and Commercial Experience With Cool Sculptin. Aesthetic Surg J. 2013;33(6):835-46
Study conducted by the Study Group in Subcutaneous Tissue – SBD, Regional São Paulo
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}