


Leandra d’Orsi Metsavaht
Burns are still the cause of a great portion of injuries and deaths triggered by external factors in Brazil. Also, it is intensely linked to absenteeism, and functional and aesthetic sequelae, especially in the male population. The assessment of burns should take into account their depth and location, involvement of the upper airways and causative agent. In cases where the treatment is carried out in an outpatient setting, after adequate washing of the lesions, 1% silver sulfadiazine cream is still the topical antimicrobial of choice, in addition to tetanus prophylaxis. Aimed at avoiding possible limitations of motion and social interaction, the prevention of hypertrophic scars and keloids is very important.
Keywords: burns; silver sulfadiazine; cicatrix; keloid
In Brazil, as well as all over the world, burns are public health problem. Children and the elderly are particularly vulnerable to this type of trauma, either because of domestic violence, pans with boiling water, dealing with alcohol or physical limitations.1
Lesions caused by burns are responsible for a large part of the external causes wounds and deaths in Brazil, as well as absenteeism, besides functional and aesthetic sequelae such as hypertrophic scarring, mainly in the male population.1
By definition, a burn is characterized as a partial or total destruction of the skin caused by thermal, electrical, chemical or radioactive trauma. Severity and prognosis of a burn are defined by the evaluation of the causal agent, depth, extension of the body surface burned, location, age, pre-existing conditions and associated lesions.
The role of the dermatologist in the treatment of burns is little discussed in the few reports in this regard. Burns occur in 2 million people per year in the United States, resulting in 60,000 hospitalizations and 6000 deaths, half of which are in children. The ratio between men and women is 2:1, either in the United States1 or in Brazil,3,6 since men are more predisposed to occupational risks.3 The mean age in Brazilian studies was 30 years.1,5 Around this age the protective force of the population is concentrated, being burns responsible for economic and social problems.1
In Millan's study about the epidemiology of burns in children, the mean age was 5.2 years. Of the total of 98 children, 67 (68.4%) were male and 31 (31.6%) were female. The accidents were responsible for 93 (94.9%) cases, and in one (1%) there was violence. In four (4.1%) cases, the circumstances of the burn were unknown. A higher occurrence of burns in children up to two years of age was observed.5
Negligence for child abuse are responsible for 20% of pediatric burns in the United States of America, being the main sources of burns in children the scalding, the fire and the electricity. Mortality rates have dropped due to better surgical and resuscitation techniques.2 In a study performed in the state of Minas Gerais, the most frequent etiological agent of burns was liquid alcohol, affecting 34.4% of patients, followed by overheated liquids (28.1%) with a highlight for water and oil, and in third place direct flame, responsible for 17.6% of burns cases.1 Scalding is the most prevalent agent in children up to four years of age,3 according to the epidemiological study of Cruz e Calfa.7
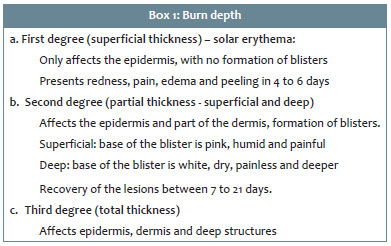
The severity and prognosis of a burn are defined by evaluating the causal agent, depth, extension of the body surface burned, location, age, pre-existing conditions and associated lesions. The treatment of these lesions, including the need for hospitalization will be guided by these factors.1,3,7 The traditional nomenclature categorizes burn wounds into first, second and third degrees (box 1). Second degree burns can then be further divided into the superficial and deep variants. Burns involving deep structures such as muscles and bones can be included as fourth degree. However, the definitive diagnosis of the depth of a burn is only possible after a time frame of 24 to 72 hours, due to occlusive vascular changes.3
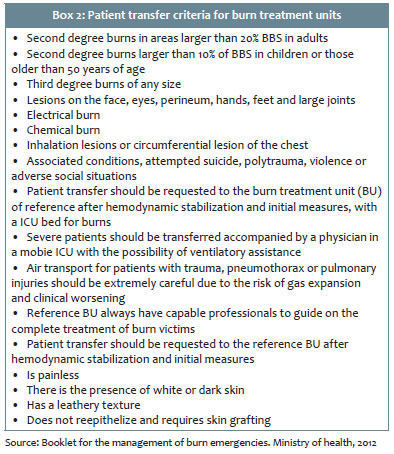
Adult patients with a second-degree body surface burn above 15% or children with more than 10%, third degree burns above 5%, electrical burns or those that involve airways, face, both hands, both feet and perineum are the classical indications for hospitalization. The physician should analyze each patient individually, indicating the best treatment, if out or inpatient.2
In areas where the dermis is thinner (such as ears, volar aspect of the forearms, medial thighs and perineum), the burns can be deeper than what is suggested by the initial presentation. This thinner dermis is also seen in children and the elderly in general. The severity of the burn is based on the rule of nines to assess the affected body area (BSA – Body Surface Area) (figure 1).1,4 This formula cannot be used in children, since the head corresponds to 19% in a two-year-old child. The initial assessment should also take into consideration airways and the cardiovascular system, since inhalation lesion can affect up to 25% of burn patients. The physician should also have in mind the possibility of hypovolemic shock, regardless of the severity of the burn and should ... fluids and rhabdomyolysis, which can seriously affect renal function3 (box 2).
Burns affecting less than 15% of the body surface can be treated in an outpatient scenario. The wound should be cleaned with water and chlorhexidine; if the latter is not available, water and neutral soap. Always remember to check if the tetanus vaccine is up-to-date. If it is not, the administration of tetanus toxoid for prophylaxis should be indicated. Circumferential burns on the chest might need escharotomy to improve thoracic expansion.2
Despite the scarce scientific evidence and studies only in animal models, silver sulfadiazine 1% is still recommended by the Brazilian Ministry of health as the standard topical antimicrobial for the treatment of burns. Face and perineum should be exposed. For the other areas, occlusive dressing with silver sulfadiazine 1%.8 Evaluate the need for systemic antibiotics.2,4
Deeper burns might need serial debridement, especially those of third and second degrees. Nowadays, human skin substitutes such as acellular dermal matrix, bilaminate collagen sulfate, chondroitin, silicone and auto transplant of cultivated epithelial cell present a lower risk for infection and better healing than autologous human and animal skin transplants.
In the case of a chemical burn, the team in charge for the first assessment should use universal protection to avoid contact with the chemical agent causing the burn, that should be identified if acid, base or organic compound. The concentration, volume and duration of contact should also be assessed. Remember that the lesion is progressive, being important to remove the clothes and remove excessive causative agent and running water for at least 30 minutes. Exhaustively irrigate the eyes in case of ocular burns. In case of burns by powder, use a brush or fabric. In doubt, make contact with the toxicological center of your area.2
After the healing period, care with future sequelae starts. Burn scar care aims at maintaining the function of the affected limbs and making them aesthetically acceptable. The objective should be achieved as quickly and comfortably and as less costly as possible. Recent studies demonstrate that silicone plaques and gels are the most effective nonsurgical treatment for burn scars with scientific evidence. They are effective both for the treatment or the prevention of hypertrophic scarring.9
Multiple mechanisms have been suggested to explain the efficacy of the silicone, including tissue hydration, pressure, increase in the scar temperature, induction of tissue hypoxia, formation of a local static field, silicone absorption, reduction of the mast cell activity, of the interleukin 1 (IL-1) level and production of extracellular matrix, all leading to the reduction of collagen synthesis.10,12 However, the exact mechanism of action is still unknown.
The most recent guidelines for the treatment of scars advocate the use of silicone therapy as prevention and as first-line treatment for keloids and hypertrophic scars. Silicone tapes and gels are nowadays the gold standard noninvasive treatment in these cases. Silicone tapes have the inconvenience of requiring fixation. Besides, the aspect in exposed areas bothers some of the patients. Treatment should be initiated soon after reepithelization of the wound. It is more effective in the immature dynamic phase of healing and it is not as effective in old scars.7
Silicone gels and tapes should be used twice a day every 12 hours, for a minimum of three months, covering the whole extension of the scar to be treated.
The fact that silicone-based products have a high cost, are noninvasive therapeutic option and present benefits explain their clinical popularity. It is an important adjuvant method in the management of hypertrophic scars.9-13
Pressure therapy has been used since the 1970s and is considered the standard therapy to treat post-burn hypertrophic scars, being the first line in many centers. A pressure between 24 and 13 mm Hg for 6 to 12 months is recommended. These data, although empirical, are based in a wide network of observers. It appears that the efficacy occurs ... aesthetic results are variable. In a randomized prospective study with 122 burn patients, pressure dressings did not increase the time for maturation of the wound nor reduced the hospitalization of patients.14
Lesions caused by Burns are still responsible for a large part of external causes wounds and deaths in Brazil, as well as absenteeism and functional and aesthetic sequelae, mainly in the male population.
The prevention is very important to reduce morbidity and mortality caused by burns, since most are accidental and perfectly avoidable, and caused by liquid alcohol. Domestic accidents represent 51% of all burns cases in our society, 80% of which take place in the kitchen. Children up to 10 years of age represent 43% of all burn cases.1 Parent's and guardian's education and safety measures at work would be the best ways to prevent burns and their consequences.3
Silver sulfadiazine 1% continues to be the topical treatment of choice for burns. The prevention of hypertrophic scars in burn patients is very important because they can bring either functional – movement range – or aesthetic and social limitations. The dermatologist has a key role for the treatment of burns and management of scars.
Leandra d'Orsi Metsavaht:
Conception and planning of the study, preparation and writing of the manuscript, obtaining, analyzing and interpreting the data.
1. Cartilha para tratamento de emergência das queimaduras. Ministério da Saúde. 2012. http://bvsms.saude.gov.br/bvs/publicacoes/cartilha_tratamento_emergencia_queimaduras.pdf.
2. Leão CEG, Andrade ES, Fabrini DS, Oliveira RA, Machado GLB, Gontijo LC. Epidemiology of burns in Minas Gerais. Rev Bras Cir Plast. 2011; 26(4):573-7.
3. Berman B, Viera MH, Amini S, Huo R, Jones IS. Prevention and management of hypertrophic scars and keloids after burns in children.J Craniofac Surg. 2008;19(4):989-1006.
4. Bologna, J et al. Textbook of Dermatology . Editora Elsevier.3a. Edição. 2015
5. Bessa DF, Ribeiro ALS, Barros SEB, Mendonça MC, Bessa IF, Alves MA, et al. Epidemic Profile of Burned Patients at the Hospital Regional de Urgência e Emergência de Campina Grande – Paraíba – Brazil. Rev Bras Ciênc Saúde. 2006;10(1):73-80
6. Miller AC, Rashid MR, Falzon L, Elamin ME, Zehtabchi S. Silver sulfadiazine for the treatment of partial-thickness burns and venous stasis ulcers. J Am Acad Dermatol. 2012; 66(5):e159-65
7. Cruz S, Calfa A. Epidemiological survey of burns in children less than six years in age admitted to the Corporation for Aid to Burned Children (COANIQUEN) in Antofagasta, Chile. Rev Cienc Salud. 2001;5(1):17-26.
8. Metsavaht LD, Surgical treatment of scars. Surg Cosmet Dermatol 2016;8 (1):11-20.
9. O'Brien L, Pandit A. Silicon gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database Syst Rev. 2006;(1):CD003826.
10. O'Brien L, Jones DJ. Silicone gel sheeting for preventing and treating hypertrophic and keloid scars. Cochrane Database of Syst Rev. 2013; (9):CD003826.
11. Kim SM, Choi JS, Lee JH, Kim YJ, Jun YJ. Prevention of postsurgical scars: comparison of efficacy and convenience between silicone gel sheet and topical silicone. J Korean Med Sci. 2014; 29(Suppl 3):249-53.
12. Tziotzios C, Profyris C, Sterling J. Cutaneous scarring: Pathophysiology, molecular mechanisms, and scar reduction therapeutics - Part II. Strategies to reduce scar formation after dermatologic procedures. J Am Acad Dermatol. 2012; 66(1):13–24
13. Momeni M, Hafezi F, Rahbar H, Karimi H. Effects of silicone gel on burn scars. Burns. 2009;35(1):70-4.
14. Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. editors.Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. p. 677-84.
This study was performed at the Instituto Brasil de Tecnologias da Saúde (Ibts) – Rio de Janeiro (RJ), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}