


Isadora Melo Zambuzzi1; Carlos Henrique Lopes Vidal1; André Cesar Antiori Freire Pessanha2
Introduction: Non-melanoma skin cancer is among the most frequent neoplasms in Brazil and is deemed a public health problem. Initial diagnosis is based on clinical suspicion and includes dermoscopy. Confirmation is carried out via histological analysis. Dermoscopy also contributes to the demarcation of tumor safety margins. Objective: To analyze the accuracy of dermoscopy in the diagnosis of non-melanoma skin cancer and its effectiveness in defining the lateral margins of these tumors in excisional biopsies. Methods: Comparison of the dermoscopy-based diagnostic hypothesis with the final histological outcome and involvement of lateral margins. Results: The data relating to a total of 70 lesions suspicious of non-melanoma skin cancer arising from a group of 50 patients were evaluated from 2015 to 2017. The comparison of the diagnostic hypothesis with the final histological outcome after excisional biopsy, indicated success rates of 79.6% for suspected cases of basal cell carcinoma and 23.8% for squamous cell carcinoma. Safety margins were observed in 74% of basal cell carcinomas and in 60% of squamous cell carcinomas. Conclusions: The diagnosis of non-melanoma skin cancers depends on experienced dermatologists and pathologists, with the interaction between these professionals being crucial. Dermoscopy has contributed in a more significant way to the diagnosis of basal cell carcinoma when compared to that of squamous cell carcinoma.
Keywords: SKIN NEOPLASMS; DIAGNOSIS, DIFFERENTIAL; MARGIN
Non-melanoma skin cancer (NMSC) is among the most common malignancies, occurring more than the other types of cancers combined,1,2 therefore being a public health issue due to its increasing incidence and to the consequent costs associated with treatment.3
Tumors that are representative for NMSC are basal cell carcinomas (BCC) and squamous cell carcinomas (SCC),4-6 the latter representing about 20% of skin cancer cases and the former approximately 70%.6 In general, they cause more morbidity than mortality, but both have the potential to metastasize (0.5% for BCC and 20% for SCC).7 Diagnostic suspicion of these tumors starts with the clinical aspect and is aided by dermoscopic features.8 BCC’s dermoscopy can present with the following signs, with high specificity:“spoke wheel” areas, large blue-grey ovoid nests, multiple blue-grey globules, “leaf-like” areas (or in “gloved finger”), arborizing telangiectasias and ulcerations (less specific).9 SCC’s is usually not that specific as to differentiate it from the early variants (actinic keratosis and Bowen disease) and, in some cases, even other entities such as seborrheic keratoses, verruca vulgaris, and keratoacanthomas. Glomerular vessels and yellow-white areas are dermoscopic findings in SCC.
The gold-standard for the diagnosis of NMSC, either BCC or SCC, is histopathology.5 There are, however, non-invasive methods to examine the lesions in an initial phase and stratify their risk, dermoscopy being one of them.12,13 Its importance consists in the necessity to minimize costs with unnecessary biopsies, define the physician’s attitude towards the patient and, in some cases, reduce surgical morbidity. On the other hand, dermoscopy contributes for the early diagnosis (early or small lesions) and appropriate treatment (determination of surgical margins). These are key-factors for a more favorable prognosis for NMSC.14
The objective of the study is to perform a self-assessment of an academic service of the Brazilian Society of Dermatology (SBD) regarding the clinical-dermoscopic accuracy rates for NMSC and analyze the degree of efficacy of the excisional biopsy in avoiding an incisional step considering the cases accurate for NMSC.
Study conducted at the service of dermatology, Universidade de Mogi das Cruzes, São Paulo, Brazil, from 2015 to 2017, where 70 suspicious lesions for NMSC were evaluated in a group with 50 patients.
Inclusion criteria for the lesions were low-risk NMSC (up to 1cm and well-defined) and prediction of non-complex reconstruction, i.e., edge-edge closure to enable wider excision in case of affected margins. The lateral margin used was 3mm and the deep margin was down to the subcutaneous tissue, with the scalpel at a 90º angle in relation to the skin.
Exclusion criteria were tumors larger than 1cm, ill-defined, recurrences and periorificial.
The lesions were registered in a database with the following information: diagnostic hypothesis, age, gender, and area of the lesion. After this step, the dermoscopic diagnostic hypothesis was compared to the final histologic diagnosis and involvement of surgical margins.
The dermoscopic diagnostic accuracy rate was defined by the degree of agreement of the diagnostic hypothesis with the final histologic report. The therapeutic accuracy rate aided by dermoscopy was defined as the percentage of NMSC cases that had surgical margins clear of malignancy.
The development of the database, as well as the analysis of the data, was done with Microsoft Excel. The statistical analysis was quanti-qualitative and descriptive.
The research was performed within the parameters of the Resolution 466/12 and their complements of the Conselho Nacional de Saúde/Ministério da Saúde, that states that collected data must be anonymous and reliable. The Committee of Ethics in Research – CEP/UMC approved the protocol of research number 50776615.8.0000.5497 and report 1.463.323.
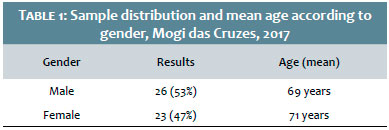
Seventy skin lesions were analyzed with diagnostic hypothesis (DH) of NMSC in a group of 50 patients, 27 being male (54%) and 23 female (46%) with a mean age of 70 years (Table 1). Of these data, the DH of BCC represented 70% and of SCC, 30%.
The diagnostic accuracy rate for BCC was of 79.6%, and for SCC, 23.8% (Table 2).
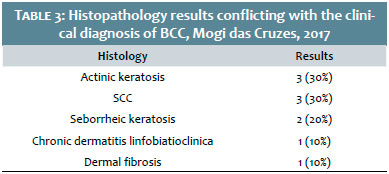
Table 3 shows the other histologic diagnoses found, that do not correspond to the clinical hypothesis of BCC.
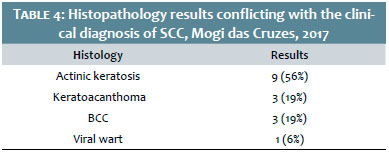
Table 4 shows other histologic diagnoses found that do not correlate with the clinical hypothesis of SCC.
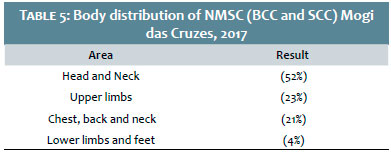
Regarding the body location, the most affected areas were head and neck, followed by upper limbs and hands (Table 5). The area more prevalent for BCC was the head and neck (63%), and for SCC, upper limbs (48%).
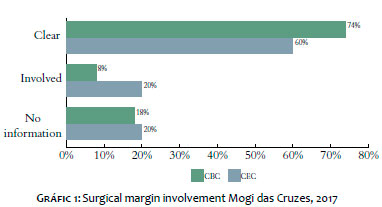
Of the accurate BCC diagnoses, 74% had surgical margins clear of malignancy, compared to 60% of SCC. There was no description of the surgical margins in seven BCC lesions and one SCC lesion (Graph 1).
(70% to 20%, 3,5 relationship).6 Regarding the results found, the proportion of BCC to SCC was of 39:8 or 4.875. Therefore, in this study, there was a higher relative prevalence of BCC compared to SCC in the histologic results.
In this study, we observed that the accuracy rate for BCC was higher than for SCC. This finding can be explained based on the more specific dermoscopic features for the former, compared to the latter.17 Dermatoses with clinical and dermoscopic features similar to SCC such as actinic keratosis (AK),15
keratoacanthoma (KAC)15,18 and verruca vulgaris (VV)19 made up an expressive percentage of the diagnoses found among suspicious SCCs. Thus, only 23.8% accuracy rate for SCC is relative. It is considered that SCC, added to this group of dermatoses clinically and dermoscopically similar corresponds to 85% of the results found with the clinical suspicion in some cases. However, we recognize that the clinical criteria to differentiate SCC of these other dermatoses failed frequently in this study.
Misdiagnosis is suspected BCCs can be explained by some factors: non-specific clinical features and dermoscopic vascular features similar in some cases of BCC, KA and SCC; even though possible, the dermoscopic differentiation17 demands a higher experience of the assistant physicians in the dermoscopy learning curve. Operator-dependent (pathologist) or even laboratory logistic (wrong slides or reports) errors must be considered.
Regarding the surgical margins, we observed that they were insufficient in some cases of NMSC, taking into consideration a 3mm excision from the outer limits of the tumor, dermoscopically marked, with a higher relevance for SCC, justifying larger safety margins than the medical literature recommends for this tumor, compared to BCC.
One possible explanation is the commonly ill-defined limits of SCCs, besides accompanying inflammation.
We should include possible operator-dependent-type biases of the histopathology. Many reports were inconclusive regarding the margins.
NMSC diagnosis depends on consistent and well sound information, using clinical, dermoscopic and, specially, histopathologic criteria. The accuracy of the first two depends largely on the experience of the dermatologist, and the third of a pathologist experienced in skin and, if possible, skin tumors. More than that, the interaction between the two professionals is extremely important.
In tertiary cutaneous oncology services, the assistant dermatologist should specify the type of biopsy (incisional x excisional) and the characteristics that lead to the clinical suspicion, so that the pathologist can fulfill their role with equal accuracy.
Dermoscopy learning curve leads to a higher accuracy rate in clinical suspicion. This resource, however, failed in differentiating SCC from other verrucous conditions. The higher surgical margin involvement in SCC cases reinforces the use of larger margins than the recommended when facing this tumor, when compared to BCCs. For BCCs, dermoscopy contributed to the diagnosis in a greater way, however, was not typical nor unanimous in the resolution of excisional biopsy
André Cesar Pessanha:
Research project, data recording and final review
Isadora Zambuzi:
Introduction and organisation of the results
Carlos Vidal:
Preparation of the tables, discussion and submission of the study
1. Rogers HW, Weinstock MA, Feldman SR, Coldiron BM. Incidence estimate of nonmelanoma skin cancer (keratinocyte carcinomas) in the U.S. Population, 2012. JAMA Dermatol. 2015;151(10):1081-6.
2. Barton V, Armeson K, Hampras S, Ferris LK, Visvanathan K, Rollison D, et al. Nonmelanoma skin cancer and risk of all-cause and cancer-related mortality: a systematic review. Arch Dermatol Res. 2017;309(4): 243-51.
3. Guy GP Jr, Machlin SR, Ekwueme DU, Yabroff KR. Prevalence and costs of skin cancer treatment in the U.S., 2002-2006 and 2007-2011. Am J Prev Med. 2015;48(2):183-7.
4. Chinem VP, Miot HA. Epidemiologia do carcinoma basocelular. An Bras Dermatol. 2011;86(2):292-305.
5. Costa CS. Epidemiologia do câncer de pele no Brasil e evidências sobre sua prevenção. Diagn. Tratamento. 2012;17(4):206-8.
6. Zink BS. Câncer de pele: a importância do seu diagnóstico, tratamento e prevenção. Revista HUPE. 2014;13(Suppl 1):76-83.
7. Bath-Hextall FJ, Perkins W, Bong J, Williams HC. Interventions for basal cell carcinoma of the skin. Cochrane Database Syst Rev. 2007;24(1):CD003412.
8. Argenziano G, Puig S, Zalaudek I, Sera F, Corona R, Alsina M et al. Dermoscopy Improves Accuracy of Primary Care Physicians to Triage Lesions Suggestive of Skin Cancer. J Clin Oncol. 2006;24(12):1877-82.
9. Rezze GG, Sá BCS, Neves RI. Dermatoscopia: o método de análise de padrões. An Bras Dermatol. 2006;81(3):261-8.
10. Firnhaber JM. Diagnosis and treatment of basal cell and squamous cell carcinoma. Am Fam Physician. 2012;86(2);161-8.
11. Fargnoli MC, Kostaki D, Piccioni A, Micantonio T, Peris K. Dermoscopy in the diagnosis and management of non-melanoma skin cancers. Eur J Dermatol. 2012;22(4):456-63.
12. Reggiani C, Manfredini M, Mandel VD, Farnetani F, Ciardo S, Bassoli S, et al. Update on non-invasive imaging techniques in early diagnosis of non-melanoma skin cancer. G Ital Dermatol Venereol. 2015;150(4):393-405.
13. Hacioglu S, Saricaoglu H, Baskan EB, Uner SI, Aydogan K, Tunali S. The value of spectrophotometric intracutaneous analysis in the noninvasive diagnosis of nonmelanoma skin cancers. Clin Exp Dermatol. 2013;38(5):464-9.
14. Deinlein T, Richtig G, Schwab C, Scarfi F, Arzberger E, Wolf I, et al. The use of dermatoscopy in diagnosis and therapy of nonmelanocytic skin cancer. J Dtsch Dermatol Ges. 2016;14(2):144-51.
15. Warszawik-Hendzel O, Olszewska M, Maj M, Rakowska A, Czuwara J, Rudnicka L. Non-invasive diagnostic techniques in the diagnosis of squamous cell carcinoma. J Dermatol Case Rep. 2015;9(4):89-97
16. Emiroglu N, Cengiz FP, Kemeriz F. The relation between dermoscopy and histopathology of basal cell carcinoma. An Bras Dermatol. 2015;90(3):351-6.
17. Lallas A, Apalla Z, Argenziano G, Longo C, Moscarella E, Specchio F, et al. The dermatoscopic universe of basal cell carcinoma. Dermatol Pract Concept. 2014;4(3):11-24.
18. Rosendahl C, Cameron A, Argenziano G, Zalaudek I, Tschandl P, Kittler H. Dermoscopy of Squamous Cell Carcinoma and Keratoacanthoma. Arch Dermatol. 2012;148(12):1386-92
19. Zanini M, Wulkan C, Paschoal FM, Maciel MHM, Machado Filho CDS. Carcinoma verrucoso: uma variante clínico-histopatológica do carcinoma espinocelular. An Bras Dermatol. 2004;79(5):619-621.
Study conducted at Universidade de Mogi das Cruzes (UMC) - Mogi das Cruzes (SP), Brasil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}