


Ada Trindade de Almeida1; Raul Banegas2; Ricardo Boggio3; Bruna Bravo4; André Braz5; Gabriela Casabona6; Daniel Coimbra7; Silvia Espinosa8; Carolina Martinez9
Introduction: In the last decade, the use of hyaluronic acid fillers for facial enhancement has increased in Latin America. Hyaluronic acid fillers are considered relatively safe with a low incidence of adverse events. Because adverse events are not seen frequently in clinical practice or have been potentially underreported, there is a need for more guidance on the diagnosis and treatment of Hyaluronic acid-related adverse events. Objective: To provide an enhanced understanding of hyaluronic acid-related adverse events and to propose recommendations for their diagnosis and treatment. Methods: A 25-member multi-disciplinary expert panel meeting of Latin-American physicians was convened in Sao Paulo, Brazil to discuss what is known about hyaluronic acid-related adverse events and to provide insights based on clinical experience. Recommendations and algorithms were developed through a consensus process. Results: The panel categorized hyaluronic acid-related adverse events based on 3 time frames of onset (immediate, early and Late) and proposed a new term for adverse events that display persistent, intermittent, delayed Swelling (PIDS). Algorithms were created for diagnosis and treatment for each time frame. Conclusions: The new consensus algorithms for time-related diagnosis and treatment of hyaluronic acid-related adverse events will provide guidance for best practices in the clinical use of hyaluronic acid fillers.
Keywords: COSMETIC TECHNIQUES; DERMAL FILLERS; HYALURONIC ACID; INFLAMMATION; SUBCUTANEOUS INJECTIONS
The use of minimally invasive cosmetic procedures is rapidly increasing in Latin America and around the globe. Hyaluronic acid (HA) injections is among the most popular cosmetic procedures for facial rejuvenation,restoration of volume and aesthetic improvement of facial volume.1 Insofar as the indications for these products increase, the number of procedures increase, and treatment paradigms evolve (for example, new products, stratification techniques and greater injection volumes), there is the need of raising awareness in regards to adverse events (AEs) that can occur as a consequence of their use.1,2
The safety profile of injectable HA fillers is usually considered favorable, with a low incidence of AEs.1 Since those AEs are rare, some clinicians might not encounter them frequently in their practices and, therefore, are not experienced to recognize, diagnose, manage and treat them. Besides, there is relatively little clinical evidence on the appropriate approach for AEs related to HA.1 Considering the lack of clinical evidence and the need for clear diagnosis and treatment strategies, an expert panel meeting was conducted in order to discuss AEs related to HA and to develop recommendations for the professionals that treat patients with injectable HA fillers.
In May, 2016, in São Paulo,Brasil, a Latin-American multidisciplinary panel convened in order to discuss and develop guidelines to adequately identify and treat AEs related to HA injection in aesthetic medicine.A total of 25 specialists attended the meeting, including dermatologists, plastic surgeons, radiologists, one pathologist and one immunologist from Brazil,Mexico,Argentina and Colombia.
The objectives of the meeting were:
Analyze the evolution of the understanding, incidence and description of AEs related to HA;
Provide a classification that allows prompt identification of HA-related adverse events;
Provide knowledge on the diagnosis and treatment of HA-related AEs based on clinical experience;
Reach a consensus and recommend algorithms for the diagnosis and treatment of HA-related AEs.
The methodology of the consensus included questionnaires distributed among the experts and, presentations and discussions within the panel afterwards. Recent examples from the literature about injectable HA-related AEs and their treatments were discussed. All the participants were involved in the creation of algorithms and tables.The polling was conducted by the moderator and consensus was reached when at least two-thirds of the participants were in agreement.
Specific recommendations presented in this article represent the expert panel assessment based on their collective experience.
HA-related AEs overview
The literature available on HA-related AEs consists on retrospective studies, case reports and expert assessment.
The understanding of HA-related AEs progressed over the last 15 years. In 2002, HA-related AEs were considered a consequence of the bacterial fermentation impurities.3 In 2005, it was seen that the same clinical AE could have two different histologic patterns, either with a granulomatous or a non-granulomatous process.4 This raised the question whether there were different etiologies when the same clinical manifestation was seen. In 2009, the classification of nodules was suggested (painless/painful or inflammatory/non-inflammatory).5 In 2010, the crucial role of biofilms in the complications from fillers started to gather attention.6 From 2009 to 2015,some authors published reviews on the treatment of HA-related AEs with hyaluronidase.7-9 During this period (2014), blindness10 and vascular complications11 were reported as HA-related AEs.
In an article from Friedman et al., the incidence of HA-related AEs was estimated in 0.15% in 1999 and 0.06% in 2000.3 This apparent reduction could have been caused by the availability of more purified raw materials for HA. In 2015, the incidence of AEs was estimated in 0.5% in a retrospective graphical analysis of 4,702 patients.12 A member of the panel noticed that Friedman’s article3 had post-marketing data, while other reports could come from the experiences of the physicians who performed the injections and represent the most recent increase of the indications for HA.
HA complications are frequently described with different terminologies that changed over the years. Some of the most common AEs reported in the beginning of the 2000s were hypersensitivity, edema not related to hypersensitivity, , infections, hematomas and ecchymosis, persistent erythema, pigmentary changes, overcorrection, necrosis (ischemia) and papulo-pustular lesions.13 As more patients were treated with HA fillers, reaction on the area of application, inadequate location, product sensitivity, infections and necrosis were also seen.14 In the end of the decade (2009), terms such as overcorrection, implant visualization, vascular damage, angioedema, erythema and telangiectasia were used to describe the AEs.15 Since the perception of the AEs evolved, additional descriptions became of note, including inadequate location, late immunomediated local reactions, hypersensitivity reactions, site infection and systemic AEs.16 Other terms were used to described AEs, including purple spots, edema, skin hypopigmentation, infection, nodular masses, paresthesia and vascular damage.2
According to Alijotas-Reig et al.,17 AEs usually begin as allergic granulomatous tissue reactions that evolve to abscesses, localized granulomatous reactions, abscess-like nodules, late granulomatous reactions, sterile abscesses, foreign body nodules ou late onset reactions. One of the members highlighted the fact that different descriptions of AEs are probably related to the same medical/clinical condition; therefore, a more consistent terminology is needed.
Other aspects of HA-related AEs
Anatomical, pathological, histological, immunological and radiological findings can help the diagnosis and treatment of HA-related AEs. From anatomical and pathological perspectives, absorbable fillers such as HA are associated to AEs with one of three different patterns of inflammation:(1) suppurative,(2) hypersensitivity reaction and (3) foreign body granuloma.The main histological findings that are relevant for the AE are: colloidal iron, that can be used as a specific stain for HA; eosinophilia, which is a typical pattern on the histopathology of HA-related AEs, that usually does not occur with other fillers (observe that HA cannot be seen on this histological finding);and capsulated HA, that can be seen in histopathological findings of foreign body granulomas with multinucleate giant cells.
From the immunological perspective, there is a lack of high level evidences to assess the effects of HA fillers.One exception was a study in 2007 by Hamilton et al.18 where it was confirmed that stabilized non-animal HA was not immunogenic in 433 participants, considering humoral immune response, because there was no activation of IgG and IgE antibodies after HA injection. Bacterial contamination and immunodeficiency were seen as factors that could contribute to the inflammation with the injection of HA fillers.
From a radiological perspective, ultrasound is a reliable method for dermatological evaluation, including for the investigation of AEs due to fillers.19 Ultrasound can help identify cosmetic fillers, characterize the AE and act as a guide for the injection of hyaluronidase. Fillers are distinct on ultrasound, and HA appears as a round or oval-shaped anechoic cyst.Wortsman et al.20 described standardized methods for the use of ultrasound in dermatology.
HA AEs Classification: Retrospect
There are some classifications of HA-related AEs described in the literature, usually time-related.The definition or time cut-off should be well demarcated for the accurate diagnosis and treatment of the AEs. A member of the panel offered examples of time-related classifications from the available literature. In 2009, Narins et al. described time-related classifications of AEs, into immediate, intermediate (two weeks to one year) and late (after one year) onsets.5 Also in 2009, Sclafani et al. utilized an alternative regimen of classification: immediate (0-2 days), early (3-14 days) and late (>14 days).15 In 2010, Rohrich et al.6 proposed a classification strategy that involved larger time intervals (≥14 days): early (<14 days), late (14 days-1 year) and delayed (>1 year). Cassuto and Sundaram (2013)21 described one classification of AE subdivided into a time scale similar to Scalfani et al.: acute (48 hours), subacute (≤2 weeks) and late (>2 weeks). Funt and Pavicic proposed a more generalized scheme of classification: early events (up to a few days) and late (from weeks to years).2 It is clear that there is a need for a classification based in consistent intervals. In 2014, Signorini et al convened a panel that proposed a more generalized scheme of classification: early and late reactions.1 The time interval of these classifications was not specified.
Diagnosis and treatment: History Treatment of HA-related AEs
The panel considered that the treatment for the AEs changed over the years -previously, immunomodulation was considered the primary treatment because HA-related AEs were predominantly hypersensitivity reactions;3 it was also acknowledged that the biopsy plays an important role in the diagnosis and treatment of HA-related AEs;4 however, the conclusion was that patients seeking aesthetic treatment would not consent to a biopsy unless absolutely necessary and that a medico-legal process is always justified.
In regards to the use of hyaluronidase for the inflammatory nodules, it was questioned whether hyaluronidase should only be used in dissolving HA (as described below)22 or if it can be used to break the biofilm’s matrix.The first evidence published on biofilms related to fillers was based on the recovery of bacteria form histological slides.23 The panel considered if bacterial culture would be an effective method to diagnose the presence of bacteria. Even though negative bacterial culture reports are commonly found in clinical practice, new evidence suggests that a more sophisticated method (such as polymerase chain reaction, fluorescence in situ hybridization, for example) can identify bacteria in cases of negative bacterial culture results.24,25 Historically, there has been inconsistencies in the literature about the antibiotic utilized and the duration of treatment for biofilms related to the use of HA fillers.A member of the panel proposed that antibiotic therapy for biofilms should continue for at least three months. Sixteen pre-clinical studies demonstrate that antibiotic therapy can be used as a preventive measure against the formation of biofilms,26 and that some studies suggest prophylactic antibiotics to prevent biofilms.6,25
Hyaluronidase
Hyaluronidase enzymatically degrades HA through specific cleavage between C1 of the glucosamine portion and C4 of glucuronic acid.27,28 Most Latin American countries do not have approved regulated hyaluronidase available for injectable use. Even in countries where the product is available, it is not specifically approved for HA fillers. Hyaluronidase is quickly inactivated when administered intravenously.29 When hyaluronidase is administered via the subcutaneous route, the dermal barrier removed by the compound takes 24 to 48 hours to be restored.28
Hyaluronidase used in Latin America is more commonly obtained in compounding pharmacies and is not approved by the regulation agencies. For example, in Brazil, the most frequently used is Hyaluronidase 2.000U-Biometil (source:purified bovine testicle). The following hyaluronidases have regulatory approval for ophthalmologic injection in listed countries: Vitrase® (Bausch + Lomb;source: purified sheep testicle; approved in the USA and Canada);Hy-lenex® (Halozyme Therapeutics;source: recombinant human produced in ovary cells of Chinese hamsters; approved in the USA and Canada); Hyalase® (Sanof-Aventis; source: purified bovine testicles; approved in the USA, Canada and Europe); and Re-ductonidasa® (Advanced Cosmeceuticals; source:purified bovine testicles; available for use in Europe).28,30,31
One member of the panel alerted the group of known uses of hyaluronidase apart from the approved indication for HA-related AEs according to the time to reaction: 1) for early onset AEs (a cut-off of 15 days was proposed based on clinical experience), hyaluronidase is known to be used for the treatment of overcorrection/dislocation, vascular occlusion, hypersensitivity (hypersensitivity reaction type IV) and angioedema (hypersensitivity reaction type I); 2) for late onset AEs (occurring after 15 days) hyaluronidase is known to be used for the treatment of non-HA related nodules (hyaluronidase is effective even when the filler is not HA, but the mechanism is unknown) or nodules related to HA, migration of the implant (even for non-HA fillers), Tyndall effect,chronic biofilm by (even for non-HA fillers),and granulomatous reaction (even for non-HA fillers). In the published literature, the dose and interval of hyaluronidase injection differ among publications and there is no standardized protocol. One of the most common hyaluronidase uses described in the literature is for the treatment of overcorrection.9,32
Factors that influence the onset of HA-related AEs
The panel discussed some important factors regarding he onset of the AE. Regarding the injection technique, fanning, rapid injection, fast flow and larger volumes can increase the incidence of HA-related AEs.33 The use of larger caliber needles can minimize trauma and, therefore, reduce the complication rate. The importance of antiseptic agents to prevent bacterial contamination and to avoid the formation of biofilm was discussed in the literature.6 There is evidence on the efficacy of antiseptic agents for the prevention of bacterial contamination, even though the antiseptics are still underused. Moreover, there is no agreement between clinicians as to which is the best antiseptic agent (for example, chlorhexidine) to be used before the injection.The anatomical location of the fillers (for example, subcutaneous versus supraperiosteum)34 was also discussed as a possible factor that could influence the occurrence rate of HA-related AEs.
Classification of AEs: panel recommendations
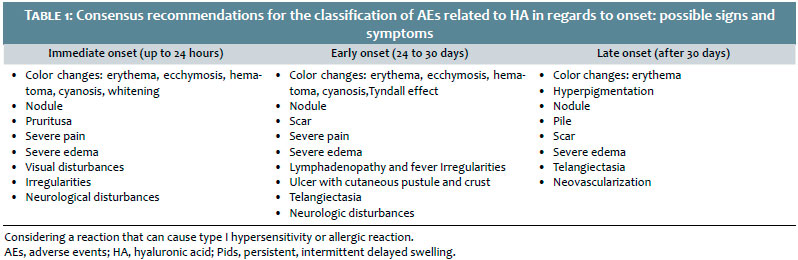
The first objective discussed by the expert panel was to implement a classification to organize the diagnosis and treatment of HA-related AEs.The panel agreed that the classification should be according to time, because the time for the onset of the AE was considered the most important information that a patient can give to the clinician.The panel defined the time for onset of the AE in three intervals: immediate onset (in up to 24 hours), early onset (from 24 hours to 30 days) and late onset (after 30 days).They also defined the most commonly seen signs and symptoms in each interval. Regarding late onset HA-related AEs, the panel also proposed the use of the expression “persistent intermittent delayed swelling”(Pids), defined as edema or swelling that occurs on the site of the filler or vicinity. It was seen that triggers such as vaccination, infection or local trauma are usually present and are frequent causes of edema.
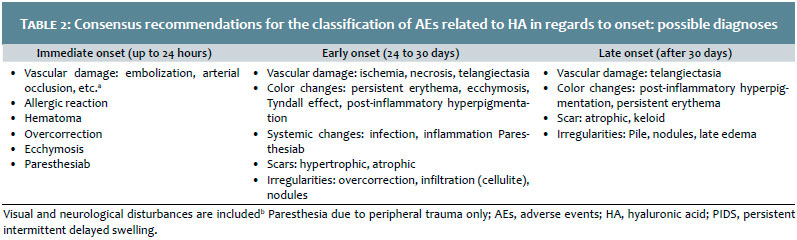
The recommended panel classification and a list of possible signs and symptoms are presented in table 1. Possible diagnoses are presented in table 2.
Diagnosis and treatment: Recommendations of the panel and algorithms
Once established the possible diagnoses for each interval, the panel discussed the treatment and the required tests for individualized diagnosis and follow-up based on the published literature and personal experience.This section resumes the group’s consensus recommendations, specialist opinions and algorithms considered by the panel to represent best practice of treatment for each diagnosis.These algorithms were built taking into consideration the diagnoses listed in table 2 for each classification related to the timing of the onset of the reaction: immediate onset (up to 24 hours), early onset (from 24 hours to 30 days) and late onset (after 30 days).
Immediate onset AEs
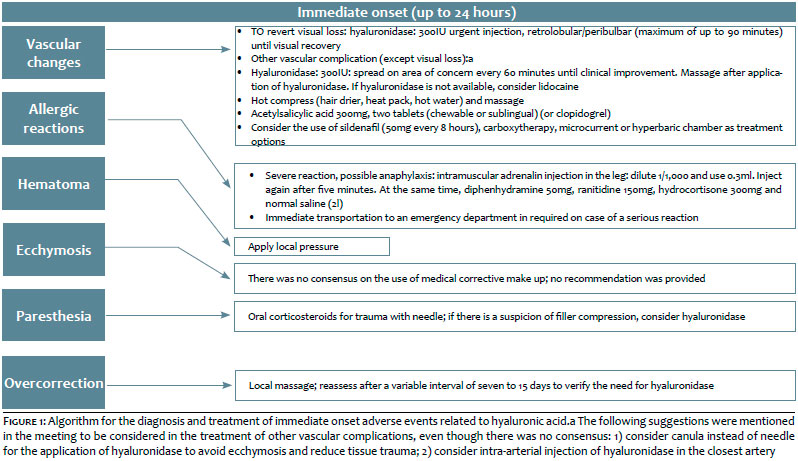
The algorithm for the diagnosis and treatment of immediate onset HA-related AEs is sown in figure 1. The panel emphasized the importance of the clinical diagnosis for vascular damage. If vascular damage is identified clinically, the immediate treatment as defined in figure 1 becomes compulsory. Recommendations of tests for follow-up of immediate onset vascular damage include consideration of ultrasound and ophthalmological and/or neurological assessment, if applicable.The panel also observed that severe allergic reactions (such as suspected anaphylaxis) require immediate treatment with adrenaline.They also made recommendations for other less severe immediate onset reactions, but there was no consensus for the treatment of ecchymosis.
Early onset AEs
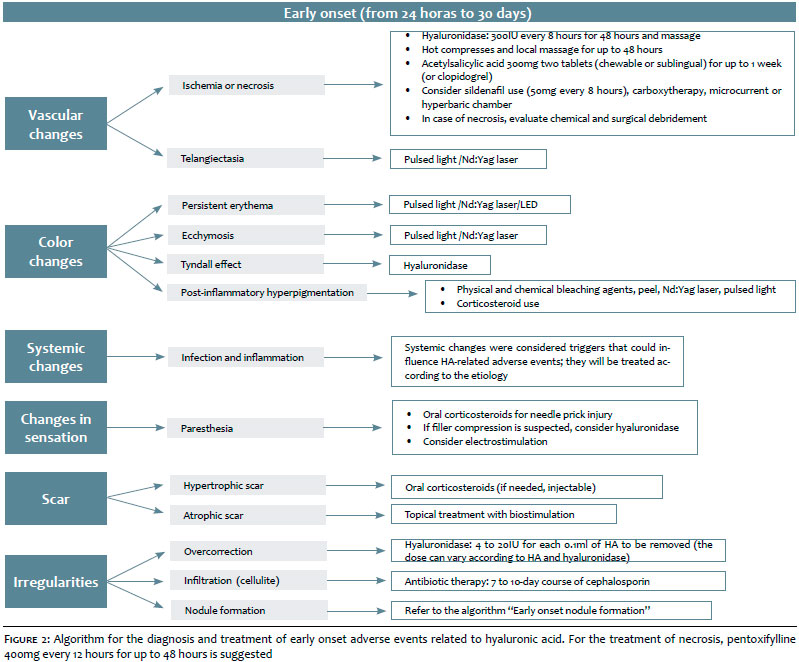
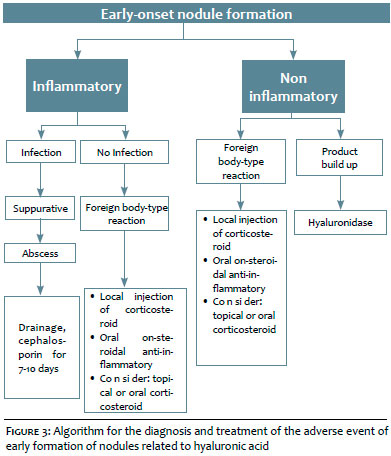
The algorithm for the diagnosis and treatment of early onset HA-related AEs is exposed in figure 2 and for the early onset formation of nodules related to HA, in figure 3.The diagnostic tests include: evaluation of systemic changes, full blood count, reactive C protein and erythrocyte sedimentation rate (ESR); ultrasound, culture (aspirates) and biopsy (the tissue must also be sent for culture) are recommended for nodules. Whenever possible, a biopsy should be performed before commencement of antibiotic therapy.The panel also observed that, in case a biopsy is performed, the tissue should also be sent for culture, because the pathogen sensitivity is higher in tissue than in aspirates. Depending on the type of test needed, a specific stain should be considered for each biopsy.These stain techniques include: hematoxylin and eosin, colloidal iron (to identify HA), Ziehl-Neelsen stain (for mycobacteria), methenamine silver, periodic acid–Schiff (PAS) and Grocott silver methenamine (for fungi). Ultrasound was also recommended as a technique for the differential diagnosis of non-inflammatory foreign body-type reactions, filler build up and for the detection of vascular AEs.Treatment recommendations include the use of antibiotics, non-steroidal anti-inflammatory agents, corticosteroids or hyaluronidase.
Late onset AEs
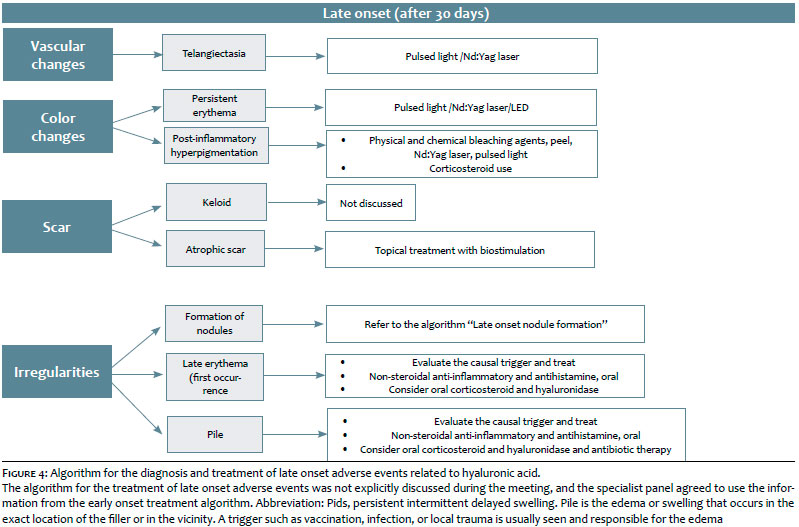
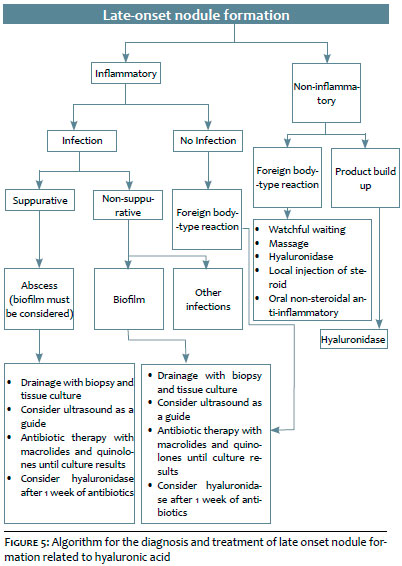
The algorithm for the diagnosis and treatment of late onset HA-related AEs is in figure 4. It must be noted that the algorithm for the treatment of these AEs was not explicitly discussed during the meeting, but the panel members agreed in utilizing an approach similar the early onset AE.The panel discussed the late onset formation of nodules (Figure 5) and noted that a similar treatment should be conducted for suppurative (abscess) and non-suppurative infection (biofilm) infection, and also for non-infectious foreign body-type reactions in the case of late onset AEs, because the clinical manifestations are similar.
Considerations for the prevention of AEs
Based on the literature and clinical experience, the panel recommended chlorhexidine over an alcohol background for disinfection, however, it must be used cautiously on the periocular region due to the risk of ocular irritation/damage.Aqueous chlorhexidine can be considered.
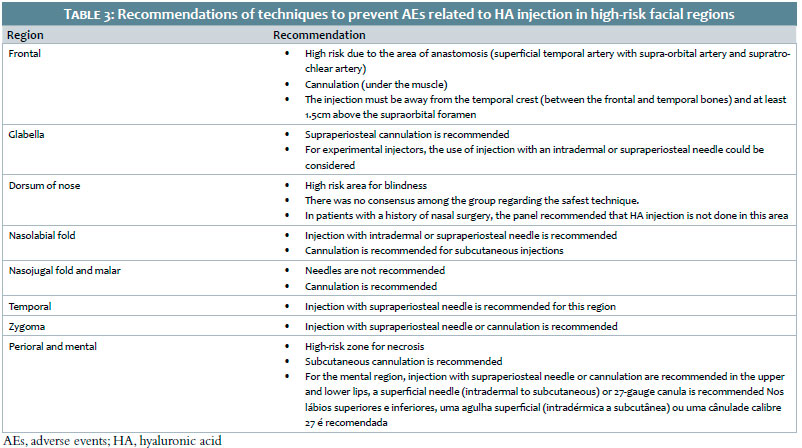
Areas of high risk for fillers were considered the areas supplied by the internal branches of the carotid artery (for example, supraorbital and supratrochlear), areas with extensive vascular anastomoses (for example, superficial temporal artery with supraorbital artery and supraocular artery; infraorbital artery with angular artery) and on the areas where the arteries emerge from the cranial foramen (supraorbital, supratrochlear and mental region). The high-risk areas are the nasolabial fold, glabella and dorsum of nose.The recommendations for the injection of HA in high-risk zones are presented in table 3.
This consensus panel meeting of experts from Latin America generated knowledge about the diagnosis and treatment of HA-related AEs.HA is considered an option for aesthetic treatment that is usually safe and has a low incidence of AEs. The panel created recommendations based in algorithms for the diagnosis and treatment according to the time of reaction onset: immediate onset (in up to 24 hours), early onset (from 24 hours to 30 days) and late onset (after 30 days).The commonest signs and symptoms and the possible diagnoses for each time interval were defined.The panel also proposed Pids as a new term for an AE of “persistent intermittent delayed swelling”occurring on the site of the filler or in its vicinity. Diagnostic and follow-up tests were also defined and recommendations for the steps aiming at preventing most commonly occurring HA-related AEs were made.
The recent increase in the uses and indications for HA highlight the importance of the knowledge shared by the Latin America Expert Panel.Their consensus recommendations provide support for clinicians that use HA fillers and can minimize their occurrence and enable the treatment of AEs.
The authors express their gratitude to the other members of the Expert Panel of Hyaluronic Acid Adverse Events: Dr. Bertha Tamura, Roseli Andrade: speakers for Merz;Christine Guarnieri, Meire Parada, Rodrigo Ferraz: speakers for Galderma; Eliandre Palermo speaker for Galderma and Merz. Maria Helena Sandoval, Fernanda Ca- vallieri, Márcio Bouer, Eduardo Finger e Gregório Pereira: no conflicts of interest.
Ada Trindade de Almeida:
Intelectual participation, preparation and proof-reading
Raul Banegas:
Intelectual participation, discussions
Bruna Bravo:
Intelectual participation, discussions
André Braz:
Intelectual participation, discussions and presentations
Gabriela Casabona:
Intelectual participation, discussions and presentations
Daniel Coimbra:
Intelectual participation, discussions
Silvia Espinosa:
Intelectual participation, discussions
Carolina Martinez:
Intelectual participation, discussions
1. Signorini M, Liew S, Sundaram H, De Boulle KL, Goodman GJ, Monheit G et al. Global Aesthetics Consensus: Avoidance and Management of Complications from Hyaluronic Acid Fillers-Evidence- and Opinion-Based Review and Consensus Recommendations. Plast Reconstr Surg. 2016;137(6):961e-71e.
2. Funt D, Pavicic T. Dermal fillers in aesthetics: an overview of adverse events and treatment approaches. Clin Cosmet Investig Dermatol. 2013;(6):295-316.
3. Friedman PM, Mafong EA, Kauvar AN, Geronemus RG. Safety data of injectable nonanimal stabilized hyaluronic acid gel for soft tissue augmentation. Dermatol Surg. 2002;28(6):491-4.
4. Parada MB, Michalany NS, Hassun KM, Bagatin E, Talarico S. A histologic study of adverse effects of different cosmetic skin fillers. Skinmed. 2005;4(6):345-9.
5. Narins RS, Coleman WP 3rd, Glogau RG. Recommendations and treatment options for nodules and other filler complications. Dermatol Surg. 2009;35(Suppl 2):1667-71.
6. Rohrich RJ, Monheit G, Nguyen AT, Brown SA, Fagien S. Soft-tissue filler complications: the important role of biofilms. Plast Reconstr Surg. 2010;125(4):1250-6.
7. Rzany B, Becker-Wegerich P, Bachmann F, Erdmann R, Wollina U. Hyaluronidase in the correction of hyaluronic acid-based fillers: a review and a recommendation for use. J Cosmet Dermatol. 2009;8(4):317-23.
8. Balassiano LK, Bravo BS. Hyaluronidase: A necessity for any dermatologist applying injectable hyaluronic acid. Surg Cosmet Dermatol. 2014;6(4):338-43.
9. Almeida ART, Saliba AFN. Hyalruonidase in cosmiatry: what should we know? Surg Cosmet Dermatol. 2015;7(3):197-204.
10. Carruthers JD, Fagien S, Rohrich RJ, Weinkle S, Carruthers A. Blindness caused by cosmetic filler injection: a review of cause and therapy. Plast Reconstr Surg. 2014;134(6):1197-201.
11. DeLorenzi C. Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J. 2014;34(4):584-600.
12. Beleznay K, Carruthers JD, Carruthers A, Mummert ME, Humphrey S. Delayed-onset nodules secondary to a smooth cohesive 20 mg/mL hyaluronic acid filler: cause and management. Dermatol Surg. 2015;41(8):929-39.
13. De Boulle K. Management of complications after implantation of fillers. J Cosmet Dermatol. 2004;3(1):2-15.
14. Cohen JL. Understanding, avoiding, and managing dermal filler complications. Dermatol Surg. 2008;34(Suppl 1):S92-9.
15. Sclafani AP, Fagien S. Treatment of injectable soft tissue filler complications. Dermatol Surg. 2009;35(Suppl 2):1672-80.
16. Alijotas-Reig J, Fernandez-Figueras MT, Puig L. Inflammatory, immune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241-58.
17. Alijotas-Reig J, Hindie M, Kandhaya-Pillai R, Miro-Mur F. Bioengineered hyaluronic acid elicited a nonantigenic T cell activation: implications from cosmetic medicine and surgery to nanomedicine. J Biomed Mater Res A. 2010;95(1):180-90.
18. Hamilton RG, Strobos J, Adkinson NF Jr. Immunogenicity studies of cosmetically administered nonanimal-stabilized hyaluronic acid particles. Dermatol Surg. 2007;33(Suppl 2):S176-85.
19. Wortsman X. Identification and complications of cosmetic fillers: sonography first. J Ultrasound Med. 2015;34(7):1163-1172.
20. Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Martorell A, Catalano O, et al. Guidelines for performing dermatologic ultrasound examinations by the DERMUS Group. J Ultrasound Med. 2016;35(3):577-80.
21. Cassuto D, Sundaram H. A problem-oriented approach to nodular complications from hyaluronic acid and calcium hydroxylapatite fillers: classification and recommendations for treatment. Plast Reconstr Surg. 2013;132(4 Suppl 2):48S-58S.
22. Soparkar CN, Patrinely JR. Managing inflammatory reaction to restylane. Ophthal Plast Reconstr Surg. 2005;21(2):151-3.
23. Lemperle G, Nicolau P, Scheiermann N. Is there any evidence for biofilms in dermal fillers? Plast Reconstr Surg. 2011;128(2):84e-5e.
24. Bjarnsholt T, Tolker-Nielsen T, Givskov M, Janssen M, Christensen LH. Detection of bacteria by fluorescence in situ hybridization in culture-negative soft tissue filler lesions. Dermatol Surg. 2009;35(Suppl 2):1620-4.
25. Alhede M, Er O, Eickhardt S, Kragh K, Alhede M, Christensen LD et al. Bacterial biofilm formation and treatment in soft tissue fillers. Pathog Dis. 2014;70(3):339-46.
26. Lebeaux D, Chauhan A, Rendueles O, Beloin C. From in vitro to in vivo models of bacterial biofilm-related infections. Pathogens. 2013;2(2):288-356.
27. Cavallini M, Gazzola R, Metalla M, Vaienti L. The role of hyaluronidase in the treatment of complications from hyaluronic acid dermal fillers. Aesthet Surg J. 2013;33(8):1167-74.
28. Hylenex recombinant [package insert]. San Diego, CA: Halozyme Therapeutics, Inc.; 2016.
29. Menzel EJ, Farr C. Hyaluronidase and its substrate hyaluronan: biochemistry, biological activities and therapeutic uses. Cancer Lett. 1998;131(1):3-11.
30. Vitrase [package insert]. Tampa, FL: Bausch & Lomb Incorporated; 2014.
31. Hyalase Product Information. Australia: sanofi-aventis; 2010.
32. Cohen B, Bashey S, Wysong A. The use of hyaluronidase in cosmetic dermatology: a review of the literature. J Clin Investigat Dermatol. 2015;3(2):7.
33. Glogau RG, Kane MA. Effect of injection techniques on the rate of local adverse events in patients implanted with nonanimal hyaluronic acid gel dermal fillers. Dermatol Surg. 2008;34(Suppl 1):S105-9.
34. Griepentrog GJ, Lucarelli MJ. Anatomical position of hyaluronic acid gel following injection to the eyebrow. Ophthal Plast Reconstr Surg. 2013;29(5):364-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}