


Bruna Morassi Sasso1; Maria Carolina Fidelis2; Maria Letícia Cintra3; Emerson Henrique Padoveze4
Rosacea can develop into phyma, which is characterized by hypertrophy of sebaceous glands and proliferation of connective tissue and blood vessels. Regarded as a serious complication, phymas are more common in men, being more frequent in the nose — when it is called rhinophyma. Rosacea and rhinophyma can cause functional and aesthetic impairment, leading to a worsening in the patients' quality of life. Pharmacological and physical therapies are performed in initial stages, however phymatous variants of the condition respond poorly to the first. The authors of the present article report a case of surgical correction of a giant rhinophyma using the shaving and electrocoagulation techniques, with excellent aesthetic and functional outcomes.
Keywords: RHINOPHYMA; ROSACEAE; ELECTROSURGERY
Rosacea is a chronic inflammatory skin condition occurring most commonly in women, with multifactorial etiology.1 Phyma is currently considered a manifestation of rosacea that, in contrast, affects more commonly men and that can be recurrent or appear as a consequence of chronic inflammation.2 Rhinophyma is the most frequent presentation, characterized by uneven thickening of the nose, from mild to florid, with dilated infundibula and telangiectases. On the histology, it is represented by a pattern similar to rosacea, with a lymphocytic and plasmacytic inflammatory infiltrate around the vessels and the infundibulum, associated with hyperplasia of sebaceous glands and peculiar angulated vessels. In the florid forms, a fibrotic pattern can be seen, with thickening of the dermis and reduction or absence of pilosebaceous follicles.3
Phymatous changes, despite benign, cause severe cosmetic problems and occasionally functional impairment.
Patients present with negative symptoms from the disease, such as low self-esteem and lessened social interactions.4 Improving those symptoms promotes the individual’s well-being.
Since the pharmacological treatment provides limited results for the phymatous form,4 we report a florid case of rhinophyma treated surgically that resulted in significant improvement and subsequent improvement of the patient’s quality of life.
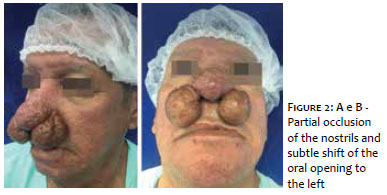
Fifty-nine-year-old Caucasian male patient presented with the complaint of thickening of the nose for 10 years. On physical examination, the nose had increased size due to papulonodular mildly erythematous soft lesions, with a cribriform surface, localized on the nasal tip, and two pedunculated tumors with similar features on the nasal alae (Figures 1.A, 1.B, 2.A). There was also a subtle shift to the left of the oral fissure and partial occlusion of the nares by the lesions (Figure 2.B). The patient denied any comorbidities, but stated that the nasal growth interfered with inhalation.
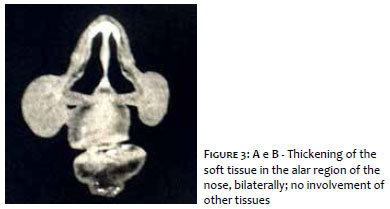
The diagnosis of rhinophyma was proposed, and imaging studies were used (computerized tomography) to assess the extent and nature of the changes, revealing no deep tissue involvement (Figure 3).
As the condition was unsightly, stigmatizing and caused functional impairment of the nose, we opted for a surgical repair. The procedure was performed in one step, with local tumescent anesthesia. Shaving was performed with a flexible surgical blade (DermaBlade®, American Safety, United States), followed by hemostasis with monopolar diathermy using low energy currents.
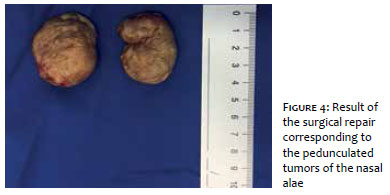
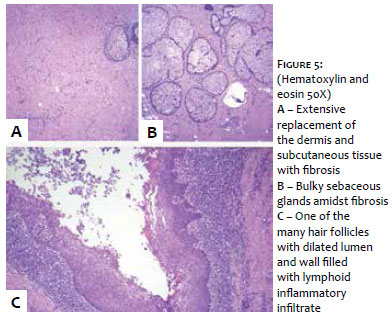
Both pedunculated tumors measured approximately 4 cm in diameter (Figure 4). Samples were sent for histology, that showed fibrosis of the dermis and subcutaneous tissue and bulky sebaceous glands and perifollicular inflammatory infiltrate, confirming the diagnosis of rhinophyma (Figure 5).
Figures 6 to 8 show the immediate, intermediate (15 days) and late (1 month) post-operative periods. It is possible to observe excellent cosmetic and functional results with great patient satisfaction. Figure 8 shows the patient before surgery and 1 month after, with resolution of the nostril occlusion.
The etiology of rhinophyma (from Greek, rhis, nose and phyma, growth)5 is unknown, currently considered serious progression of rosacea.6 It can cause cosmetic and functional impairment, besides local irritation and pain.6
Patients with rosacea have high rates of anxiety and depression, higher than alcoholism.7 They can also present with shyness and social phobia due to the skin condition.8
Aiming at clinical and quality of life improvement for the patient with rosacea, it is crucial to base the approach in the pharmacological, behavioral and physical therapies. Pharmacological therapy has low effectiveness for the phymatous presentations4 and the surgical approach is usually advocated.5 Destructive treatments can be performed with CO2 laser, conventional ablative surgery, dermabrasion and electrosurgery.4,9
Of the surgical options, we chose shaving and cautery, a safe, effective and low cost option. In this case, it offered the patient an exceptional and very satisfactory result.
Bruna Morassi Sasso
Performed the surgery and provided photographs Wrote the manuscript
Maria Carolina Fidelis
Performed the surgery Helped write the manuscript
Maria Letícia Cintra
Histological examination Photograhps
Emerson Henrique Padoveze
Surgical coordinator Manuscript review
1. Yigider AP, Kayhan FT, Yigit O, Kavak A, Cingi C. Skin diseases of the nose. Am J Rhinol Allergy. 2016;30(3):83-90.
2. Addor FAS. Skin barrier in rosacea. An Bras Dermatol. 2016;91(1):59-63.
3. Schüürmann M, Wetzig T, Wickenhauser C, Ziepert M, Kreuz M, Ziemer M. Histopathology of rhinophyma - a clinical-histopathologic correlation. J Cutan Pathol. 2015;42(8):527-35.
4. Hofmann MA, Lehmann P. Physical modalities for the treatment of rosacea. J Dtsch Dermatol Ges. 2016;14 Suppl 6:38-43.
5. Little SC, Stucker FJ, Compton A, Park SS. Nuances in the management of rhinophyma. Facial Plast Surg. 2012;28(2):231-7.
6. Weinkle AP, Doktor V, Emer J. Update on the management of rosacea. Clin Cosmet Investig Dermatol. 2015;7;8:159-77.
7. Moustafa F, Lewallen RS, Feldman SR. The psychosocial impact of rosacea and the influence of current management options. J Am Acad Dermatol. 2014;71(5):973-80.
8. Gupta MA, Gupta AK, Chen SJ, Johnson AM. Comorbidity of rosacea and depression: an analysis of the National Ambulatory Medical Care Survey and National Hospital Ambulatory Care Survey-Outpatient Department data collected by the U.S. National Center for Health Statistics from 1995 to 2002. Br J Dermatol. 2005;153(6): 1176-81.
9. Lazzeri D, Agostini T, Spinelli G. Optimizing cosmesis with conservative surgical excision in a giant rhinophyma. Aesthetic Plast Surg. 2013;37(1):125-7.
Study conducted at Universidade Estadual de Campinas (Unicamp) – Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}