


Aloísio Carlos Couri Gamonal1; Dário Nascimento Ferreira Alves2; Sônia Maria Neumann Cupolilo3; Dominique Fonseca Rodrigues Lacet4
Pachydermodactyly is a rare, benign and acquired form of digital fibromatosis characterized by the thickening of soft tissues in the lateral regions of the proximal interphalangeal joints, typically of the digiti II, III and IV of both hands. In most cases it is associated with repeated digital microtraumas. The authors of the present article report the case of a 22-year-old patient with a typical clinical presentation of the condition. The treatment with triamcinolone injections led to a partial reduction of the thickening, in addition to hypopigmentation and hyperemia, meaning it was an unfavorable option. Although rare and benign, this typical clinical condition deserves attention, and unnecessary and costly investigations, as well as inappropriate treatments should be avoided.
Keywords: HAND DERMATOSES; SOFT TISSUE NEOPLASMS; FINGERS; YOUNG ADULT; GLUCOCORTICOIDS; CUMULATIVE TRAUMA DISORDERS; FIBROMA; TREATMENT OUTCOME
Pachydermodactyly (PDD) was initially described by Bazex et al. in 1973 as a “digital pachyderma of the first phalanges”.1 Two years later, Verbov, based on the Greek words pachy (thick), dermo (skin) and dactylos (finger), named it as a variant of the true interphalangeal pad.2 PDD is a rare, benign and acquired form of digital fibromatosis, characterized by the thickening of soft tissue in the lateral aspect of the proximal interphalangeal joints (PIJ). A review article identified only 161 reported cases, being more common in men during puberty and young adults.3
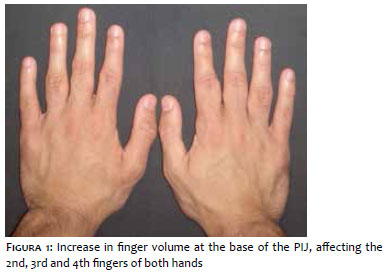
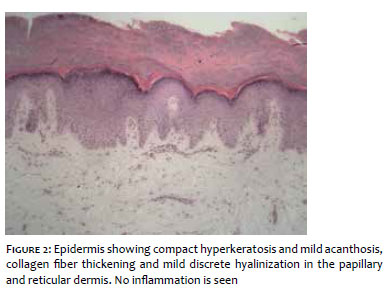
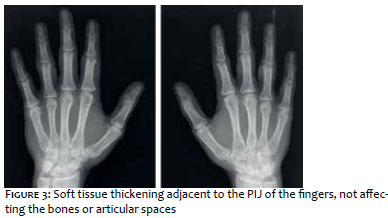
Twenty-two-year-old male patient, college student, complains of progressive increase in volume on the base of his fingers over the past 5 years. He reports repeat minor trauma during his teens due to the habit of cracking his knuckles and constantly touching his fingers. He denied systemic signs or symptoms. Physical examination revealed increase in finger volume on the base of the PIJ, affecting the 2nd, 3rd and 4th fingers of both hands (Figure 1). The changes were asymptomatic, with no loss of finger movement and his main concern was the cosmetic appearance. Histopathology of an elliptical skin biopsy of the PIJ region of the 3rd left finger showed compact hyperkeratosis and mild acanthosis of the epidermis, besides thickening of the collagen fibers and mild hyalinization in the papillary and reticular dermis, with no inflammation in the dermis nor any changes on the appendages (Figure 2). Hands and wrists radiograph showed thickening of soft tissue close to the PIJ of the fingers, with no bony or joint space changes (Figure 3). The diagnosis of pachydermodactyly was then made, and the patient was informed of its benign nature. Despite knowing that, the patient requested treatment for cosmetic reasons.
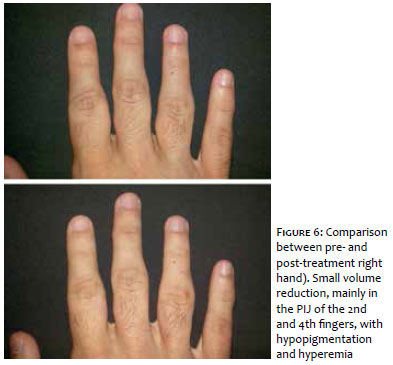
We opted to treat with 20mg/ml triamcinolone acetonide solution. As the initial approach, we injected into the affected area, PIJ of the 4th finger of the left hand, to see if there was going to be any adverse reaction to the medication, and there was none. Two weeks later, the procedure was performed again in the PIJ of the 2nd, 3rd, and 4th fingers of both hands. On review after 3 months, there was a mild reduction in volume in the PIJ area of the 4th left finger and 2nd right finger, with erythematous (secondary to neovascularization) and hypopigmented areas, common steroid side effects. The patient opted to have another session in the areas he considered the worst: PIJ of the 4th left finger and 2nd and 4th right fingers. Two months later, more reduction, although mild, of volume was observed; nonetheless, there was increase in hyperemia and hypopigmentation. The comparison between pre- and post-treatment can be seen in figures 4, 5 and 6.
The exact etiology of PDD is unknown. It is likely to be a consequence of repeated minor traumas associated to friction, interlacing and cracking the knuckles, as in this case and others.4,5,6 However, there are reports of unknown cause with no history of repeated minor traumas or touching the hands.6,7
The typical presentation of PDD is edema and asymptomatic thickening of the periarticular soft tissue of the PIJ of the 2nd-4th fingers, occurring symmetrically in both hands, with no bone abnormalities, synovitis or restriction of movement. The thickening is mainly located on the radial and ulnar distribution. There can be lichenification and scaling on the affected areas.5 In some cases, pain.7 Unilateral PDD was also described.8 Less often, the thumbs can also be thickened.6 Our patient had the typical presentation, bilateral and symmetrical, on the PIJ of the 2nd to the 4th fingers.
PDD was already described in association with: Dupuytren’s contracture, Asperger syndrome, Ehlers-Danlos syndrome, carpal tunnel syndrome, tuberous sclerosis, gynecomastia, feet syndactyly, atrophia maculosa varioliformis cutis, and Tourette syndrome.3
Differential diagnosis includes many conditions: true interphalangeal pad, pseudo-knuckle pad, collagenous plaques of the hands, juvenile digital fibromatosis, juvenile hyaline fibromatosis, nodular fibromatosis of the skin, acromegaly, thyroid disease, fibrous inflammatory conditions, among others.5
Histologically, there is hyperkeratosis, acanthosis, thickening of the dermis, increase in fibroblasts and collagen deposits, thickening of the basement membrane and of the eccrine sweat glands, intense build-up of mucopolysaccharides, poor demarcation between papillary and reticular dermis, mucin deposits between type III and V collagen fibers with reduction in type I collagen.3
Hand radiographs and magnetic resonance imaging (MRI) show thickening of soft tissues with no bone involvement or articular abnormalities, as in this case.3,7
Chen et al.6 proposed the following diagnostic criteria:
• asymptomatic patient
• no morning stiffness
• no pain on movement or tenderness on palpation
• non-circumferential thickening of the radial or ulnar fingers
• laboratory tests showing non-specific results
• plain radiographs only showing thickening of soft tissues.
With the typical findings, additional work up such as MRI or skin biopsy are not usually necessary for the diagnosis. In our case, histopathology findings were useful to exclude similar conditions and to support the clinical and radiographic findings of PDD.
There is no effective well-established treatment for PDD at present. There are reports of thickening regression upon ceasing digital friction.4 There are reports showing that oral Tranilast for 6 months, an antiallergic drug, improved thickening.7 Triamcinolone injections reduced the volume after 2 sessions in 1 month, with mild hypopigmentation.9 In our patient, the injections resulted in partial reduction with subsequent hypopigmentation and hyperemia, not making it a good option from the cosmetic point of view. Surgical excision can also be an option.10
We concluded that triamcinolone injections may not be a good option due to the possibility of secondary hypopigmentation and hyperemia, besides subtle reduction of volume. Although rare and benign, this typical condition must be considered, avoiding unnecessary and costly investigations, as well as inappropriate treatments.
To Dr. Annair Freitas do Valle, our gratitude for the application of the medication.
Aloísio Carlos Couri Gamonal
Clinical diagnosis, therapeutic approach and patient follow-up.
Dário Nascimento Ferreira Alves
Clinical diagnosis, therapeutic approach and patient follow-up.
Sônia Maria Neumann Cupolilo
Histological diagnosis.
Dominique Fonseca Rodrigues
Lacet Histological diagnosis.
1. Bazex A, Dupré A, Teillard J. Pachydermie digitale des premieres phalanges par hyperplasie conjonctive dermique et aplasie hypodermique. Bull Soc Fr Dermatol Syphiligr. 1973;80:455-8.
2. Verbov J. Letter: Pachydermodactyly: a variant of the true knuckle pad. Arch Dermatol. 1975;111(4):524.
3. Paravina M, Stanojevic´ M, Jovanovic´ D, Ljubisavljevic´ D. Pachydermodactyly: a case report and literature review. Serbian Journal of Dermatology and Venereology. 2014;6(4):174-85.
4. Requena CB, Miot HA, Marques ME, Miot LD. Case for diagnosis. Pachydermodactyly. An Bras Dermatol. 2014;89(2):359-60.
5. Beltraminelli H, Itin P. Pachydermodactyly--just a sign of emotional distress. Eur J Dermatol. 2009;19(1):5-13.
6. Chen CK, Shyur SD, Chu SH, Huang LH, Kao YH, Liu LC. Pachydermodactyly: three new cases in Taiwan. J Microbiol Immunol Infect. 2015;48(3):340-4.
7. Higuchi C, Tomita T, Yoshikawa H. Pachydermodactyly treated with tranilast in a young girl. Case Rep Orthop. 2014:132854.
8. Cabanillas M, Monteagudo B, León-Muíños E, Suárez-Amor O. Pachydermodactyly in a young girl: cutaneous manifestation of a psychiatric disorder? Pediatr Dermatol. 2010;27(3):306-8.
9. Pereira JM, Pereira FCN, Pereira VCN. Interphalangeal pads on pachydermodactyly. An Bras Dermatol. 2004;79(3):313-21.
10. Dias JM, Costa MM, Romeu JC, Soares-Almeida L, Filipe P, Pereira-da-Silva JA. Pachydermodactyly in a 16-Year-Old Adolescent Boy. J Clin Rheumatol. 2012;18(5):246-8.
Study conducted at Núcleo de Pesquisa em Dermatologia (Nupede) of the Hospital Universitário da Universidade Federal de Juiz de Fora (HU-UFJF) - Juiz de Fora (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}