


Maria Claudia de Almeida Issa1; Diego Cerqueira Alexandre2; Roger Domingos Almeida3; Sandra Maria Barbosa Durães1
Paraffinoma results from the implantation of mineral oil in the skin, being characterized by inflammatory reaction of foreign body type, with variable latency period. Initial lesions consist of hardened nodules, which can ulcerate, fistulate or necrose. This technique was widely used for aesthetic purposes in the 20th century, and is no longer performed by physicians. However, it is still used by non-medical professionals or by the patients themselves, mainly in the genital region, aimed at improving sexual activity. This paper reports a case of implantation of mineral oil in the penis, performed by a non-medical professional, for aesthetic purposes that evolved with necrosis after three years.
Keywords: GRANULOMA, FOREIGN-BODY; MINERAL OIL; NECROSIS; PENIS
Paraffinoma is an adverse reaction after injection of mineral, plant or animal oils in the subcutaneous tissue or skin. It is characterized by a non-allergic foreign body-type granulomatous reaction on histopathology.1-3 The latency period between the injection of the substance and initiation of the reaction is variable, from a few days to many years.3-6 This technique was often used in the 20th century for cosmetic purposes.1,6
Complications of this practice are reported since 1906 and contributed to its discontinuation in many countries. Nowadays, it is still performed by non-medical professionals and by patients, mainly for penis enlargement, in Asian and east European countries.4,6,7 Lesions start as indurated solitary or confluent nodules, forming plaques in the subcutaneous tissue and skin. Sometimes there is ulcer formation and fistulas with purulent or oily discharge and, in more advanced cases, necrosis of the affected area.3,7-10
Paraffinoma or oleoma, also known as mineral oil granuloma, is the histological pattern that appears after injection of substances with saturated hydrocarbon chains in the skin or subcutaneous tissue. Due to the inability of human enzymes to degrade these substances, a foreign body-type granulomatous reaction can occur, in which part of the subcutaneous tissue is replaced by cysts of different sizes. They manifest clinically as indurated nodules that can also be associated with lymphatic drainage obstruction, caused by the non-absorbable substance. This lesion can occur within a few days or manifest years after injection of the substance.1-6
The injection of non-absorbable substances such as oils is an ancient and obsolete practice used since the beginning of the 20th century, aiming at correcting imperfections and improving cosmetic appearance.3,6,10 The first report of the use of these substances for cosmetic purposes is from 1899, when Gersuny injected mineral oil into a boy’s scrotum after bilateral orchiectomy due to tuberculosis.1-8
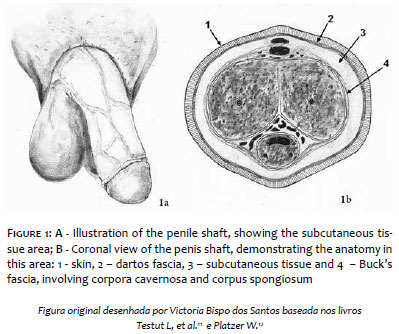
This practice was abandoned by physicians due to disastrous adverse reactions, but is still performed by non-medical professionals and by patients.2,5,6,9 Of the penile enhancement techniques used by these professionals, the most common are inoculation of semiliquid substances and the implantation of penile spheres. These spheres are composed of metal or plastic, measure around 1 cm and contain non-absorbable liquid substances, such as mineral oil, in their interior. They are injected into the subcutaneous tissue above Buck’s fascia (Figure 1).10
Even though there are reports of immediate effects and good cosmetic results as volume enhancement for the modification of the shaft contour, mineral oil injection triggers short and long term complications: skin inflammation, edema, abscess, lymphangitis, ulcers, local migration, corpora cavernosa invasion, phimosis, paraphimosis, erectile dysfunction, urinary disturbances and, in advanced cases, skin necrosis of the penile shaft.3,6-10 The inflammation associated with the injection of mineral oil can rarely lead to the development of squamous cell carcinoma.1,6,10
The treatment of choice is surgery, aiming at removing the paraffinoma. Antibiotics and oral steroids can be required, apart from surgical intervention. In the case of necrosis, surgical or chemical debridement is indicated, associated with supportive measures as steroids, tetracyclines or colchicine due to the difficulty in completely removing the substance injected.3,5,6,8-10
Thirty-eight-year-old male patient, Caucasian, professional tattoo artist underwent application of mineral oil spheres in the penis 3 years ago, by a non-medical professional (tattoo artist), with the purpose of modifying the penile surface. After two years, he noticed rupture of the spheres, with flattening of the implants and subsequent induration of the shaft’s skin. He did not seek medical care immediately. With the progression of the lesion, he decided to seek a plastic surgeon, that surgically debrided it. The clinical course was not satisfactory, and resulted in necrosis of the penile shaft’s skin.
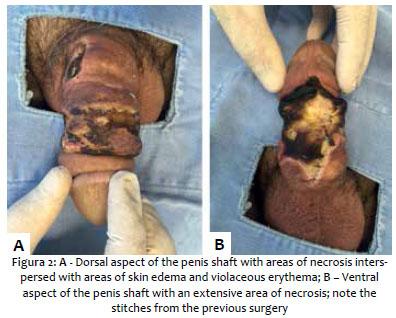
One month after the procedure, the patient was seen as an outpatient, complaining of local intense pain, but had no urinary complaints nor fever. On examination, there were indurated areas and violaceous erythema on the dorsal aspect and necrosis on the ventral aspect of the penis’ shaft. Penile shaft and glans edema was also observed (Figure 2), with no enlarged glands or meatal discharge. The scrotum was spared. On the day of the consultation, he was taking cephalexin 500mg q.i.d. We opted to continue treatment with cephalexin, adding collagenase with topical chloramphenicol, prednisone (60mg/day) and oral dipyrone.
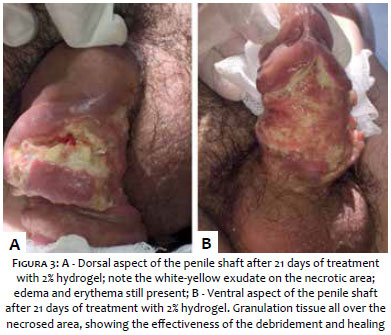
After one week the patient returned, still complaining of severe local pain and fever (37.8ºC). The dorsal aspect was still edematous, indurated, had a violaceous erythema and necrosis of the superficial tissues. However, the ventral aspect of the penis showed some improvement, with no necrosis and some granulation areas. He was then examined by the urology team that initially ruled out urethral lesions. Ciprofloxacin 500mg t.d.s and clindamycin 600mg t.d.s were initiated, both orally. The dose of prednisone was maintained, but the topical treatment was changed to 2% hydrogel because of its selective chemical debridement effect. After 21 days, the patient returned with improvement of the lesions on both aspects of the penis (Figure 3). The antibiotics were discontinued and tapering of prednisone begun.
The patient was also assessed by a plastic surgeon, who opted to do a surgical approach. First, a subcutaneous tunnel was designed on the scrotum so that the penis could pass through it. On the second stage, a graft with skin from the scrotum was place
The complications derived from paraffinoma can manifest within a few days of injection or years later. As in this case, where they appeared 2 years after placement of the implant. Usually, indurated nodules are observed, and those can ulcerate and fistulate, having as differential diagnoses genital ulcers of many etiologies. Albeit rare, necrosis can occur, compromising urinary and sexual functions of the organ.3,6-10 In this case, the patient’s penile urethra was apparently not damaged according to the urologist’s evaluation, and he had no trouble passing urine despite the edema. The erectile function of the penis was also spared, despite the complaint of pain. The urology team offered to perform uretherocystoscopy after clinical improvement of the necrosis for a better assessment of the urethra.
The recommended treatment will vary according to the clinical presentation. Surgery for removal of the indurated nodules is initially indicated, and it must be performed as early as possible. In this case, the patient sought medical care only after one year of having the lesion. In cases of more severe complications, such as necrosis, chemical or surgical debridement must be performed.5,6,8-10
Although paraffinomas are extremely rare nowadays, physicians must be vigilant for its recognition, since many patients will not admit to clandestine mineral oil injection. Early diagnosis is crucial for a good prognosis of the affected organ. In the case of male genital implants, a multidisciplinary approach, with urology and plastic surgery, is necessary.
Maria Claudia de Almeida Issa
Medical care of the patient and manuscript supervision, orientation and proofing.
Diego Cerqueira Alexandre
Medical care of the patient and manuscript elaboration.
Roger Domingos Almeida
Surgical care of the patient and image structuring.
Sandra Maria Barbosa Durães
Medical care of the patient and manuscript supervision, orientation and proofing.
1. Imbert E, Milpied B, Jouary T, Versapuech J, Goussot JF, Taieb A, et al. Penile swelling and ulceration. Acta Derm Venereol. 2010;90(1):81-2.
2. Cohen JL, Keoleian CM, Krull EA. Penile paraffinoma: self-injection with mineral oil. J Am Acad Dermatol. 2002;47(5 Suppl):S251-3.
3. Magrin PF, Ribeiro CO, Quevedo Filho LP, Durães SMB, Rochael MC. Oleoma: Relato de caso com boa resposta à tetraciclina. Dermatol Online J. 2010;16(10):7. Portuguese.
4. Santos P, Chaveiro A, Nunes G, Fonseca J, Cardoso J. Penile paraffinoma. J Eur Acad Dermatol Venereol. 2003;17(5):583-4.
5. Balighi K, Farsinejad K, Naraghi ZS, Tamizifar B. Paraffinoma and ulcer of the external genitalia after self-injection of nandrolone. Int J Dermatol. 2008;47(10):1092-4.
6. Pehlivanov G, Kavaklieva S, Kazandjieva J, Kapnilov D, Tsankov N. Foreign-body granuloma of the penis in sexually active individuals (penile paraffinoma). J Eur Acad Dermatol Venereol. 2008;22(7):845-51.
7. Glicenstein J. Les premiers « fillers », vaseline et paraffine. Du miracle à la catastrophe. Ann Chir Plast Esthet. 2007;52(2):157-61. French.
8. Hohaus K, Bley B, Köstler E, Schönlebe J, Wollina U. Mineral oil granuloma of the penis. J Eur Acad Dermatol Venereol. 2003;17(5):585-7.
9. Inn FX, Imran FH, Ali MF, Ih R, Z Z. Penile augmentation with resultant foreign material granuloma and sequalae. Malays J Med Sci. 2012;19(4):81-3.
10. Dewandre M, Brasseur E, Andrianne R. À propos d'un cas d'auto-injection pénienne de vaseline. Rev Med Liège. 2014;69(2):94-6. French.
11. Testut L, Latarjet A. Tratado de Anatomía Humana. 9th ed. Barcelona: Salvat; 1959.
12. Platzer W, editor. Pernkopf Anatomy: Atlas of Topographic and Applied Human Anatomy. 3th ed. Munich: Urban & Schwarzenberg; 1989.
Study conducted at the Service of Dermatolgy at Hospital Universi- tário Antônio Pedro da Universida- de Federal Fluminense (Huap/UFF) – Niterói (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}