


Mauricio de Quadros1; Analupe Webber2; Mariana Silveira Ferreira3; Ana Paula Schwarzbach4
Introduction: Standard dilution of botulinum toxin is performed with 0.9% saline solution. Some studies show that when diluted in lidocaine and epinephrine, the toxin preserves its function without compromising effectiveness or safety.
Objective: To establish whether the paralyzing effect of ona-toxin type A reconstituted in anesthetic (2% lidocaine) and vasoconstrictor agent (1: 50,000 epinephrine) is as effective as that of the same toxin reconstituted in saline solution, at 48 hours, 1 week, 2, 4, 12 and 24 weeks, for the treatment of periocular lines. To compare the tolerance to pain between the two reconstitution alternatives.
Methods: Fifteen patients with periocular wrinkles were randomized to receive onabotulinum toxin diluted in lidocaine with epinephrine or in saline. Re-evaluations were carried out in 48 hours, 1 week, 2, 4, 12 and 24 weeks.
Results: The data indicate that there was no difference in the symmetry and durability of the botulinum toxin, nor in the pain during the application.
Conclusions: There was no statistically significant difference in the frequency of lateral periocular muscle paralysis and symmetry resulting from the applications of onabotulinum toxin reconstituted in lidocaine with epinephrine or in saline solution. This outcome is consistent with those of previous studies.
Keywords: BOTULINUM TOXINS, TYPE A; DILUTION; LIDOCAINE
The injection of botulinum toxin (BT) aimed at treating facial wrinkles is one of the most widely performed procedures worldwide.1 Botulinum toxin is a powerful neurotoxin derived from the bacterium Clostridium botulinum that acts on the neuromuscular junction by inhibiting the release of acetylcholine, causing a temporary neuromuscular blockade.2 The bacterium produces several BT serotypes — namely A, B, Ca, Cb, D, E, F, G 3 — of which the strongest is serotype A, which is most commonly used for cosmetic treatments.4 Serotype A BT cleaves Snap-25 (25KDa synaptosome-associated protein), from the Snare complex (soluble NSF attachment receptor).5 The effects of BT on the target muscles decrease over time as Snap-25 protein regenerates and muscle contractility is restored.6
Botulinum toxin was approved by the US’ FDA (Food and Drug Administration) for cosmetic use in 2002 regarding the treatment of the glabellar complex muscles, and in 2013 for periocular lines. It is used off-label for all other facial cosmetic indications.7 There are currently 3 types of A toxins approved by the FDA for cosmetic use in the glabellar lines: onabotulinum toxin A, abobotulinum toxin A and incobotulinum toxin A.8
The standard dilution of BT is carried out with 0.9% saline.9-11 Some studies show that when diluted in 1% lidocaine and 1:100,000 epinephrine, BT keeps its function without compromising effectiveness or safety.12-14 The advantage of reconstituting it in lidocaine and epinephrine is that there is an increase in its short-term efficacy, accelerating the onset of the effect and reducing the discomfort associated with injections.15 In most patients, the full effect of botulinum toxin-induced paralysis is imperceptible before 48 to 72 hours after application,12 and the effect lasts for 3 to 4 months.15
The present study was carried out to establish whether the paralyzing effect of the onabotulinum toxin type A reconstituted in anesthetic (2% lidocaine) and vasoconstricting agent (1:50,000 epinephrine) is as effective as that of the same toxin reconstituted in saline solution after 48 hours, 1 week, 2 weeks, 4 weeks, 12 weeks and 24 weeks, for the treatment of periocular lines, and to compare pain tolerance in the two possibilities.
A randomized, double-blind clinical trial was conducted between June 2016 and February 2017. Patients aged 25-55 years with lateral periocular wrinkles treated at the Dermatology Ambulatory of the Santa Casa de Porto Alegre were invited to take part in the study. Fifteen individuals were selected using a convenience sampling method. All signed a Free and Informed Term of Consent and completed the study. Patients meeting the following criteria were excluded: bearers of neuromuscular disease, allergy to botulinum toxin type A, lidocaine, or epinephrine, facial paralysis or asymmetric mimicry, with history of botulinum toxin application in the periocular region less than 12 months before, history of facelift, use of medications that interfere with the neuromuscular junction (aminoglycosides and calcium channel blockers).
A blinded investigator applied 6U of onabotulinum toxin A diluted in saline to the lateral part of the orbicularis oculi muscles on one of the sides. On the other side, the same amount was applied, however the substance was reconstituted in 2% li-docaine and 1:50,000 epinephrine. Two U of BT were applied in three points. Patients were instructed to avoid manipulation or massage at the treated site, lying flat for 4 hours, and perform physical exercises during the 24 hours after the applied.
In order to evaluate the functional state of the mimetic musculature, photographs were taken and videos made of the patients’ faces at rest and forcing the smile to the maximum, before and after the procedure. The same records were taken in the 6 subsequent experimental timepoints (48 hours, 1 week, 2 weeks, 4 weeks, 12 and 24 weeks after). Questionnaires aimed at assessing satisfaction, adverse effects, pain, and treatment durability were answered by the patients throughout the study. Following the procedure, an evaluator blinded to the difference in dilutions between the treated sides (standard solution and experimental dilution) analyzed the photographs, videos and answers to the questionnaires at each step.
The data were entered in an MS Excel spreadsheet and then exported to the SPSS v.20.0 software for statistical analysis. The categorical variables were described by frequency and percentage, while the quantitative variables were described by mean values and standard deviations. The McNemar test was used to compare variables between the sides treated with the different dilutions. A significance level of 5% was considered. The study project was approved by the institution’s Research Ethics Committee (n. 58100316.8.0000.5335) and in compliance with the Declaration of Helsinki.
Data were collected from 15 female patients. The mean age was 39.1 years (SD = 7.9, min = 25, max = 52). Regarding previous treatments, 9 (60%) patients had never undergone the procedure before, 2 (13.3%) had undergone it once, 1 (6.7%) had undergone it twice, 2 (13.3%) had undergone it five times and one (6.7%), six times.
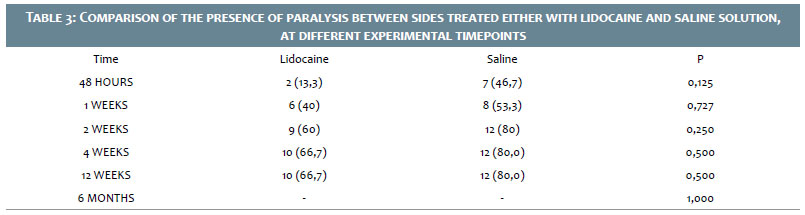
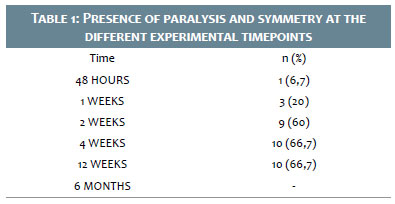
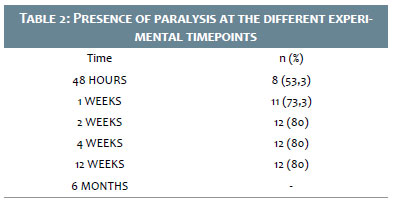
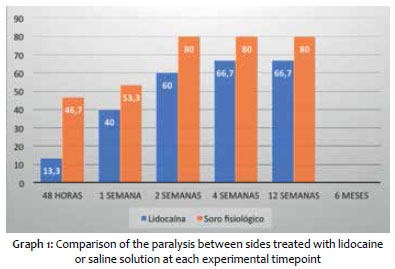
The majority of patients had paralysis within 48 hours (Table 1), and both paralysis and symmetry within 2 weeks (Table 2). The sides applied with lidocaine and saline solution were compared at each experimental timepoint of the evaluation (Graph 1). There was no statistically significant difference between the sides in any of the evaluated timepoints.
Ten (66.7%) patients reported pain. Three (20.0%) patients reported pain regarding the side treated with lidocaine, while 8 (53.3%) reported pain in the side diluted with saline. There was no statistically significant difference (P = 0.180).
Whitening effect was observed in 6 (40.0%) patients, all on the side treated with lidocaine. It is important to note that it was not possible to compute the statistical significance, since no patient showed whitening on the side treated with saline solution.
The present study’s main objective was to establish whether the paralyzing effect of onabotulinum toxin A reconstituted with anesthetic (2% lidocaine) and vasoconstrictor agent (1:50,000 epinephrine) is as effective as that of the same toxin reconstituted with saline solution at 48 hours, 1 week, 2 weeks, 4 weeks, 12 weeks and 24 weeks, for the treatment of periocular lines. This study found no statistically significant difference in the paralyzing effect in any of the experimental timepoints in which the patients in both groups (lidocaine and saline solution) were evaluated and compared with the assistance of photographs and videos. Other authors have reported symmetry when comparing the two types of dilution 1 week after the application.12,16
The present study also assessed the tolerance to pain, evidencing that there was no decrease in pain on the side treated with saline when compared to the side treated with lidocaine. Lidocaine tends to be painful due to its acid pH, which does not seem to offer an advantage regarding the minimization of pain during the application of BT.17 Gassner et al. studied 10 volunteers, reporting an immediate and statistically significant paralyzing effect when BT was diluted in 1% lidocaine and 1:100,000 epinephrine.12 Kim et al. investigated the satisfaction of 181 patients who received BT type A reconstituted in 1% lidocaine with 1:100,000 epinephrine, describing the immediate paralytic effect caused by the anesthetic as positive.18 In addition, epinephrine is mentioned in some articles as beneficial for minimizing the diffusion of BT.12,13,19
The present study’s results are limited due to the small sample size. In this manner, a non-significant value allowed to state that there was no difference between the different types of dilutions or, alternatively, the sample was too small to allow detection of any difference. The present study used 2% lidocaine and 1:50,000 epinephrine, while other studies found in the literature employed 1% lidocaine and 1:100,000 epinephrine. The study did not propose to evaluate the doses necessary to achieve better clinical outcomes in the periocular region, since it used similar doses in all patients, aiming at verifying the paralysis and symmetry effects related to the two different types of dilution. Finally, the blinded evaluator carried out a subjective assessment of the photographs and videos due to the fact that there was no objective scale of measurement.
In line with the literature, the present study did not evidence statistically significant difference in the frequency of lateral periocular muscle paralysis and symmetry in the application of BT reconstituted with lidocaine and epinephrine as compared with that reconstituted only with saline solution. The data suggest that the effects durability was similar in both groups. Also, the pain sensation during the application was not inferior to that in the lidocaine group.
Maurício de Quadros
Bibliographic survey, project design, botulinum toxin application, preparation of the discussion and conclusion sections, and final editing of the paper.
Analupe Webber
Bibliographic survey, structuring of the study project, photographic and and video based evaluation of outcomes.
Mariana Silveira Ferreira
Bibliographic survey, structuring of the study project, patient randomization and selection, preparation of photographs and videos, photographic and video based reassessment of patients.
Ana Paula Schwarzbach
Bibliographic survey, structuring of the study project, patient randomization and selection, photographs and videos, preparation of photographs and videos, photographic and video based reassessment of patients.
1. Cosmetic Surgery National Data Bank Statistics. Aesthet Surg J. 2015;35 Suppl 2:1-24.
2. Wohlfarth K, Muller C, Sassin I, Comes G, Grafe S. Neurophysiological double-blind trial of a botulinum neurotoxin type a free of complexing proteins. Clin Neuropharmacol. 2007;30(2):86-94.
3. Small R. Botulinum toxin injection for facial wrinkles. Am Fam Physician 2014;90(3):168-75.
4. Carruthers J, Carruthers A. The use of botulinum toxin type A in the upper face. Facial Plast Surg Clin North Am. 2006;14(3):253-60.
5. Dressler D, Saberi FA, Barbosa ER. Botulinum toxin: mechanisms of action. Arq Neuropsiquiatr. 2005;63(1):180-5.
6. Blasi J, Chapman ER, Link E, Binz T, Yamasaki S, De Camilli P, et al. Botulinum neurotoxin A selectively cleaves the synaptic protein SNAP-25. Nature. 1993;365(6442):160-3.
7. Allergan. BOTOX COSMETIC (onabotulinumtoxinA) for injection, for intramuscular use [Internet]. Irvine: Allergan; 2013 [cited 2017 Apr 30]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/103000s5260lbl.pdf
8. Dessy LA, Fallico N, Mazzocchi M, Scuderi N. Botulinum toxin for glabellar lines: a review of the efficacy and safety of currently available products. Am J Clin Dermatol. 2011;12(6):377-88.
9. Sapra P, Demay S, Sapra S, Khanna J, Mraud K,Bonadonna J. A single-blind, split-face, randomized, pilot study comparing the effects of intradermal and intramuscular injection of two commercially available botulinum toxin a formulas to reduce signs of facial aging. J Clin Aesthet Dermatol. 2017;10(2):34-44.
10. Lee JH, Sung IY, Yoo JY, Park EH, Park SR. Effects of different diluitions of botulinum toxin type A treatment for children with cerebral palsy with spastic ankle platarflexor: a randomized controlled trial. J Rehabil Med. 2009;41(9):740-5.
11. Schantz EJ, Johnson EA. Properties and use of botulinum toxin and other microbial neurotoxins in Medicine. Microbiol Rev. 1992;56(1):80-99.
12. Gassner HG, Sherris DA. Addition of an anethetic agent to enhance the predictability of the effects of botulinum toxin type A injections: a randomized controlled study. Mayo Clin Proc. 2000;75(7):701-4.
13. Haubner F. Simultaneous injection of lidocaine improves predictability of effect of botulinum toxin. Laryngorhinootologie. 2009;88(12):764.
14. Vadoud-Seyedi J, Simonart T. Treatment of axillary hyperhidrosis with botulinum toxin type A reconstituted in lidocaine or in normal saline: a randomized side-by-side, double-blind study. Br J Dermatol. 2007;156(5):986-9.
15. Walker TJ, Dayan SH. Comparasion and overview of currently available neurotoxins. J Clin Aesthet Dermatol. 2014;7(2):31-9.
16. Güleç AT. Dilution of botulinum toxin A in lidocaine vs. in normal saline for the treatment of primary axillary hyperhidrosis: a double-blind, randomized, comparative preliminary study. J Eur Acad Dermatol Venereol. 2012;26(3):314-8.
17. Emami Zeydi A, Khezri HD. Can lidocaine be safely used to reduce pain caused by intramuscular penicillin injections? A short literature review. Oman Med J. 2012;27(4):337.
18. Kim A, Jung J, Pak A. Botulinum toxin type A reconstituted in lidocaine with epinephrine for facial rejuvenation: results of a participant satisfaction survey. Cutis. 2013;Suppl:13-8.
19. Redaelli A, Forte R. Botulinum toxin diluition: our technique. J Cosmet Laser Ther. 2003;5(3-4):218-9.
This study was carried out at the Dermatology Service of the Santa Casa de Misericórdia de Porto Alegre - Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}