


Marina de Souza Barletta2; Leticia Arsie Contin1; Fernanda Freitas de Brito2; Gabriela Nero Mitsuushi2; Kedima Caldeira Nassif2; Livia Mendes Sabia2
Introduction: Microneedling has been performed in several areas of Dermatology, including the treatment of androgenetic alopecia. However, one of its major limitations is pain, which occurs both with the use of rollers with multiple fine needles and with motorized devices equipped with microneedles.
Objective: To describe a new technique aimed at minimizing pain during the microneedling in the scalp.
Methods: An observational, prospective and comparative study of the microneedling effects was performed with a motorized device, with and without folding the skin by using the thumb and index finger of the surgeon’s non-dominant hand. This procedure was termed “pinch technique” by the authors. The pain was assessed by the patient based on a visual analogue scale, and the data analyzed with the Student’s t-test, in order to verify the existence of statistical difference between the data sets.
Results: Fourteen patients bearers of androgenetic alopecia (13 men and 1 woman) were treated. The analysis of the data on the pain reported by the patients suggested that the arithmetic mean of the data obtained from the areas where the technique was not applied was greater than that obtained in areas where the technique was employed.
Conclusions: The described technique was proven effective in reducing pain during the microneedling procedure. That outcome resulted from the alteration of the perception of pain due to the tactile stimulus and the increase in the distance of the needles regarding the galea, which is richly innervated.
Keywords: AMBULATORY SURGICAL PROCEDURES; ALOPECIA; NEEDLES
Microneedling is part of the therapeutic armamentarium of contemporary dermatology. It has recently gained an important role in trichology, emerging as an excellent method to be combined with the clinical treatment of androgenetic alopecia. Studies show that microneedling releases platelet-derived and epidermal growth factors by activating the wound regeneration process that takes place after the skin undergoes perforation caused by microneedling. They also show that microneedling promotes stimulation and overexpression of genes related to hair growth, such as those of Wnt3a and Wnt10 path.1 The procedure is straightforward and can be performed with cylinders or motor-powered devices containing microneedles, with the patient’s pain and anxiety being challenges to be overcome.
In both types of devices, it is possible to use needles 0.5 to 2.5mm long, with the intensity of the pain being proportional to the length of the used needle. When needles penetrate up to 0.25mm into the skin, the procedure is painless, however with longer needles, the pain varies from mild to severe.
The present study was aimed at evaluating a procedure termed the pinch technique by the authors. In this technique, digital pressure is applied in order to fold the skin of the area to be treated as a way to decrease the pain described by the patient during the microneedling procedure.
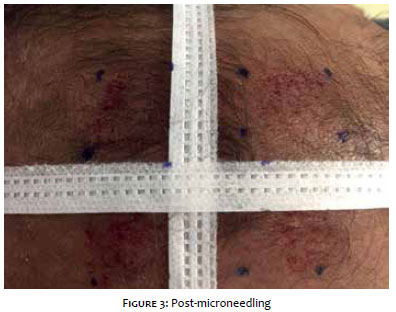
An observational, prospective and comparative study was carried out, observing the ethical principles of the Declaration of Helsinki. The pain described as a consequence of microneedling performed with the conventional technique was compared with that resulting from the procedure performed with the pinch technique. Patients with androgenetic alopecia were selected at the trichology ambulatory of the Hospital do Servidor Público Municipal de São Paulo, Brazil. The inclusion criteria were: age above 18 years and clinically evident androgenetic alopecia. The exclusion criteria were: blood dyscrasias, history of bleeding or use of oral anticoagulants, presence of autoimmune diseases, Koebner’s phenomenon, or any health condition or use of medication that, in the opinion of the dermatologist physician, rendered them ineligible. Topical anesthesia (14% lidocaine associated with 7% tetracaine, in gel vehicle dispensed by Drogaderma, Brazil) was applied and maintained for 30 minutes in the scalp of the patients, followed by asepsis with 1% aqueous chlorhexidine. The scalp was divided into quadrants with a tape arranged linearly from the highest point of the right ear’s helix up until the corresponding point in the left ear, and another arranged from the glabellar region to the bony protuberance of the occipital region. Next, squares with sides measuring 2cm were demarcated in each of the quadrants, from the point where the tapes intersected on the scalp, forming two anterior superior quadrants and two inferior posterior quadrants (Figure 1). The patients underwent a microneedling session with the assistance of the Cheyenne® tattooing device (Cheyenne®, Germany), with the energy parameter set at 70Hz and queued needles model 17-bp-Magnum (Cheyenne®, Germany), with an adjustable depth of 1mm. The microneedling procedure, without the use of medication, was performed in the four squares previously demarcated. In the left hemicranium (T1: posterior; T3: anterior) it was performed with the conventional technique. In the right hemicranium (T2: posterior, T4: anterior), the pinch technique was used during the microneedling procedure, meaning that the area of the scalp to be treated was pinched between the surgeon’s non-dominant hand’s thumb and index finger (Figure 2). The final goal was to obtain similar bleeding dews in the quadrants (Figures 3 and 4). After 30 seconds, the pain was evaluated by the patient based on the visual analogue scale (VAS) — a simple, practical tool deemed as reproducible for the measurement of pain. In order to perform the photographic records, an 8-megapixel Apple iPhone 6’s digital camera was used under identical environmental conditions immediately after the procedure. The data were later on analyzed using the Student’s t-test (Microsoft Excel software), aimed at verifying the presence of statistical difference, with a significance level of 5%.
The patients were numbered from 1 to 14: 13 males and 1 female, minimum age = 29 years, maximum age = 70, mean age = 44 years. Fitzpatrick’s phototypes ranged from II to IV!
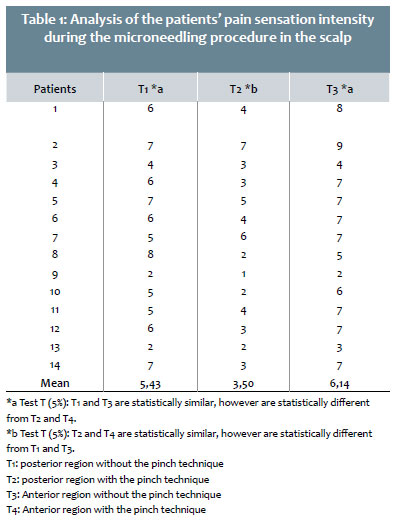
After the patients have attributed scores to their own pain sensation (Table 1) based on the VAS, it was possible to observe that the arithmetic means of the posterior quadrants (T1 = 5.43, T2 = 3.50) were statistically different from each other. A similar result was observed in the anterior quadrants (T3 = 6,14, T4 = 3,43), demonstrating the effectiveness of the pinch technique in reducing the pain during the microneedling procedure in the scalp.
Despite the fact that the arithmetic mean was higher in the anterior region, the comparison between the left (T1 and T3) and right (T2 and T4) hemicrania indicated that the results were statistically similar for a 5% level of significance. Of the 14 patients included in the study, 2 did not present altered perception of pain (patients 2 and 13) and 1 (patient number 7) reported a worsening of the pain sensation.
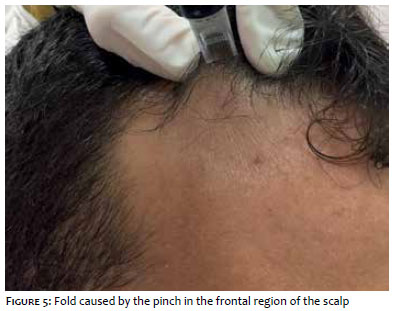
The microneedling procedure described in Dermatology as a tool in the treatment of cutaneous aging and acne scars by stimulating the synthesis of collagen has had its use expanded for treating alopecia.1 Pain during minimally invasive skin procedures is caused by the activation of two nocireceptors: the small and slightly myelinated Aδ fibers and the non-myelinated C fibers. Painful stimuli are carried by these nerve fibers to the dorsal spinal ganglion and then to the central nervous system, being received into the cortex.2,3 Pain modulation occurs mainly through the interaction of Aδ with C fibers, inhibitory interneurons of the spinal cord, and cortical control by the brain.3 Vibratory analgesia seems to be explained by the interaction between two cortical areas that encode pain and touch, respectively.4 Pain can be quantified by several described methods, the most accepted being the quantification by VAS, which assigns grades from 0 to 10 to the pain perceived during a procedure. Grades 1 and 2 refer to mild pain; Grades 3 to 7, to moderate pain; and Grades 8 to 10 to intense pain.5 Classical analgesia using topical anesthetics, such as lidocaine and prilocaine creams applied 30-60 minutes prior to microneedling, is not enough to eliminate the pain inherent in the procedure. Therefore, it is important to combine non-anesthetic analgesia techniques; such as vibratory and tactile stimuli.5 Microneedling causes pain by mechanical stimulation, and can be mechanic-chemical when associated with the infusion of low-pH drugs into the dermis. When exerting pressure or vibration during the procedure, more than one type of sensorial stimulus reaches the cortex, “deceiving” the pain bearer, which can be interpreted as a reduction of the pain sensation.3,4 In this manner, this new technique decreases the patient’s perception of pain, due to the association of another neuro sensitive stimulus at the site. Comparing the anterior and posterior regions, the perception of pain was more intense in the first, however without statistical significance. It is believed that this difference is due to the scalp’s anatomy, given the presence of a greater amount of sensory nerves in the frontal region and the smaller amount present in the parietal region. Based on the patients’ self-perceived VAS, the vast majority described improvement - with statistical significance - in the pain associated to the pinch technique. The authors of the present article believe that this technique decreases the pain caused by the procedure by altering its perception based both on the tactile stimulus and the formation of a cushion in the fold caused by the pinch, which reduces the proximity of the needles to the galea, which is richly innervated. The pinch technique is straightforward, costless, reproducible, and can be performed in any region of the scalp (Figure 5). It may, however, be more difficult to perform in some patients who have a less elastic scalp. The procedure is technician-dependent and requires adequate training for its effective implementation.
Minimally invasive procedures for treating alopecia have been shown to be effective and gaining relevance world wide, however pain remains a limiting factor to patient adherence. The use of the pinch technique allows achieving the desired result with greater patient comfort and at no additional cost.
Marina de Souza Barletta
created the technique, performed the described procedure in the patients, designed and assisted in the writing of the paper.
Leticia Arsie Contin
performed the described procedure in the patients, designed and assisted in the writing of the paper.
Fernanda Freitas de Brito
performed the described procedure in the patients, designed and assisted in the writing of the paper.
Gabriela Nero Mitsuushi
performed the described procedure in the patients, designed and assisted in the writing of the paper.
Kedima Caldeira Nassif
performed the described procedure in the patients, designed and assisted in the writing of the paper.
Livia Mendes Sabia
performed the described procedure in the patients, designed and assisted in the writing of the paper.
1. Dhurat R, Sukesh MS, Avhad G, Dandale A, Pal A, Pund P. A randomized evaluator blinded study of effect of microneedling in androgenetic alopecia: a pilot study. Int J Trichology. 2013;5(1):6-11.
2. Beiteke U, Bigge S, Reichenberger C, Gralow I. Pain and pain management in dermatology. J Dtsch Dermatol Ges. 2015;13(10):967-87
3. van der Spek FB. Methods of pain-reducing in diagnostic and therapeutic procedures in paediatric dermatology - a clinical study. The Netherlands: Erasmus University Rotterdam; 1998. Chapter 1, Aspects of pain in medical care in children; p. 9-20.
4. Hollins M, McDermott K, Harper D. How does vibration reduce pain? Perception. 2014;43(1):70-84.
5. Jeong HR, Lee HS, Choi IJ, Park JH. Considerations in the use of microneedles: pain, convenience, anxiety and safety. J Drug Target. 2017;25(1):29-40.
This study was carried out at the Hospital do Servidor Público Municipal (HSPM) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}