


John Verrinder Veasey1; Marina Dall'Antonia2; Barbara Arruda Fraletti Miguel3; Silvia Assumpção Soutto Mayor4; Adriana Bittencourt Campaner5; Thiago da Silveira Manzione6
Introduction: The occurrence of anogenital warts in children is relatively rare, however it generates distress for the family and the physician regarding the possible association with sexual abuse.
Objective: To demonstrate cases of anogenital wart in children and the therapeutic options used.
Methods: Retrospective descriptive study of anogenital warts in children under 12 years of age, with a mean age of 4 years, treated between 2011 and 2015, in a sexually transmitted diseases public outpatient clinic in the Brazilian Southeast city of São Paulo.
Results: The authors demonstrated 20 cases — of which 12 were female and 8 were male. The preferred location for the lesions was the perianal region (70%), with 30% of the children presenting extragenital warts. The treatment of choice in 65% of cases was the application of topical medication (podophyllin and imiquimod). The longest time to cure was 20 weeks.
Conclusions: Anogenital condyloma was more frequent in girls, the mean age was 4 years, and the most affected site was the perianal region. The lesions had good therapeutic response with the application of the topical treatment of choice.
Keywords: CONDYLOMATA ACUMINATA; WARTS; CHILD; CHILD ABUSE, SEXUAL; THERAPEUTICS
Anogenital warts result from human papillomavirus (HPV) infection.1 Reports of pediatric cases have been increasingly published in the medical literature,1 however little is known about the actual epidemiology of HPV in this age group.2 The diagnosis of anogenital condyloma causes distress to both the physician and the patient’s family in the face of possible association with sexual abuse. Knowledge about HPV infection through nonsexual contact is important when considering the implications of an investigation of sexual abuse.3 The interpretation of anogenital condyloma in children as evidence of sexual abuse is controversial, since the prevalence of HPV in sexually abused children ranges from 5% to 33% while in children without suspected abuse is roughly 16% .2 In light of this fact, the presence of anogenital warts in children may be the result of sexual abuse, which, however, does not seem to be the main means of contagion of these lesions. Other manners of transmission can not be excluded or forgotten at the time of the investigation.2,3
The objective of the present study was to review the cases of genital warts in children treated at a public ambulatory specializing in a sexually transmitted diseases outpatient public unit, their clinical characteristics and therapeutic responses.
A retrospective descriptive study analyzed cases of anogenital warts in children of up to 12 years of age treated at the Sexually Transmissible Disorders (STD) Ambulatory in the city of São Paulo, between 2011 and 2015.
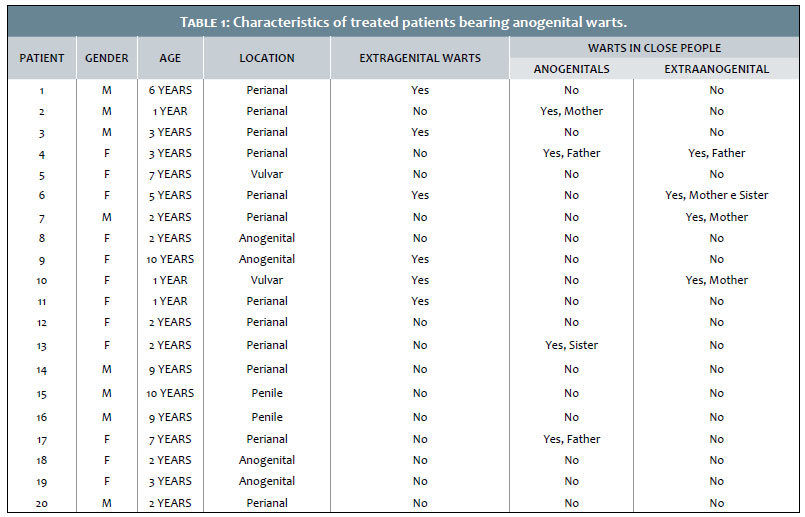
Twenty patients were treated (12 female and 8 were male), of whom 60% (12) presented exclusively perianal warts, 20% (4) had warts concomitantly affecting genital and anal regions, and 20% (4) had warts only in the genitalia (10% penile and 10% vulvar, with 2 patients each). Of the patients evaluated, 30% (6) had extragenital warts. People who had close contact with the patients were also evaluated for the presence of warts. Four relatives (20%) had genital warts (2 fathers, 1 mother and 1 sister), and 4 relatives (20%) had extragenital warts (Table 1). In 55% of cases, diagnosis was achieved by the association of clinical and dermoscopic methods, without confirmatory histological examination. Histological examination was performed in 9 children. Of the 20 children studied, 18 had their lesions treated, while 1 was still being followed up, and 1 did not attend the follow up session. The treatment of choice in 65% of the cases employed topical medication (20% podophyllin and 5% imiquimod), meaning : 6 children (30%) were treated with imiquimod alone, 3 (15%) were treated with podophyllin, and 4 (20%) with imiquimod and podophyllin. Imiquimod at a 5% concentration was used in cream (one sachet applied in the affected region at night on Mondays, Wednesdays and Fridays, washing 8 hours after). Podophyllin at a 20% concentration was used in in solid petrolatum, applied weekly by the physician at the outpatient clinic, with instructions for cleansing the region 4 hours after the application. Four patients (20%) underwent the combined therapy of one of the topical agents followed by a destructive method (chemosurgery with 90% trichloroacetic acid, electrocauterization or cryotherapy), with complete resolution of the picture. One patient had been taken by her mother to another medical service, where electrocauterization was performed with unsatisfactory aesthetic outcome, prompting the search for our service. The maximum time to achieve cure was 20 weeks.
Non-sexual HPV transmission can occur in a number of ways that include direct or indirect personal contact with contaminated objects or surfaces and vertical transmission. Syrjänen and Puranen conducted a review of the various acquisition modes of HPV and anogenital warts in children (from birth to 12 years of age), demonstrating the presence of a high prevalence of disease transmitted by means other than sexual contact.4 In 185 patients with anogenital warts, 67 (36%) had a known source of acquisition, such as autoinoculation, nonsexual transmission from other family members, and possible vertical transmission from the mother.4 In a study by Jones et al., the suspicion of sexual abuse was reported in only 3 (2%) of 131 patients, showing that clinical evidence of HPV does not usually correlate with that occurrence.3 It is important to note that the existence of people who have close contact with the patients or even caregivers with warts on the hands does not rule out the possibility of abuse, since abuse is not limited to sexual contact. In addition, children are not cared for only by family members. Many are under the care of others, making research extremely complex and invasive. In the present study, a multidisciplinary team evaluated patients and their families, and psychological and pediatric evaluations were included to address the psychosocial and family contexts, aiming at avoiding the possibility of abuse.
The prevalence of other STDs in the context of child sexual abuse is 4%. This investigation is mandatory in the declared or evident cases, with positive results being a strong indication of its occurrence in all other cases.1 All 20 patients in the present study underwent serology tests for HIV, syphilis, hepatitis B and C, with absence of diagnosis of any of these infections in the studied population.
The diagnostic method used in the study was an association of clinical and dermoscopic techniques in 55% of the cases, without confirmatory histological examination. As described by Verasey Veasey et al., clinical and dermoscopic examinations yield sufficient criteria to confirm the diagnosis of anogenital warts.5 In the case of lesions in children, reaching diagnosis while avoiding invasive procedures is an advantage.
There is no consensus for the treatment of anogenital warts, including those that affect children.6,7 The therapeutic choice should be individualized, and in the experience of the medical service in question, preference is given to topical, less traumatizing treatments that evolve with fewer sequelae (Figure 1). In the patients studied in this paper, the topical therapies used included 5% imiquimod in cream and 20% podophyllin in solid petrolatum. Although there are restrictions on the use of these therapies in patients under 12 years of age, some studies indicate their use in children at lower ages.7-10 The therapy of choice was 5% imiquimod, with 20% podophyllin therapy being chosen when there was no possibility of buying the product. In patients whose topical therapy was proven ineffective, destructive therapies were associated with resolution of the condition. Four patients (20%) underwent combined topical therapy followed by destructive therapy, with total resolution of the condition.
One patient was dissatisfied with aesthetic damage resulting from electrocauterization performed at another medical service, thus exemplifying the risk of performing destructive therapies in the treatment of anogenital warts (Figure 1). There was no correlation between the time to cure (20 weeks maximum) and the location of the lesions, nor between cure and adopted therapy. The combined treatment was longer, probably due to the fact that it was indicated in more complex cases, with a greater number of lesions and difficulty to conduct an adequate ambulatorial follow-up. The authors do not believe age is a factor of therapeutic difficulty.
Anogenital warts in children pose a challenge to the physician not only due to the diagnosis, but also for issues that accompany the picture, among them, the way of acquiring the lesion and the best therapeutic approach. It is critical to examine the child and the people who have close contact with him / her in search for lesions, and to request serologies for STD screening. According to the literature, the prevalence of sexual abuse as a means of transmission of the lesions does not seem to be the main one.
John Verrinder Veasey:
Statistical analysis, approval of the manuscript's final version, study design and planning, elaboration and writing of the manuscript, effective participation in the research guidance, intellectual participation in the propaedeutic and / or therapeutic management of the studied cases, critical review of the literature and manuscript.
Marina Dall'Antonia:
Obtaining, analyzing and interpreting data.
Barbara Arruda Fraletti Miguel:
Obtaining, analyzing and interpreting data.
Silvia Assumpção Soutto Mayor:
Intellectual participation in the propaedeutic and / or therapeutic management of the studied cases.
Adriana Bittencourt Campaner: Intellectual participation in the propaedeutic and / or therapeutic management of the studied cases.
Thiago da Silveira Manzione:
Intellectual participation in the propaedeutic and / or therapeutic management of the studied cases.
1. Rodrigues LR, Portugal V, Rodrigues N, Nápoles S, Casanova C. Verrugas anogenitais na criança: a importância da abordagem multidisciplinar. Acta Med Port. 2011;24(2):367-70
2. Unger ER, Fajman NN, Maloney EM, Onyekwuluje J, Swan DC, Howard L, et al. Anogenital human papillomavirus in sexually abused and nonabused children: a multicenter study. Pediatrics. 2011;128(3):e658-65.
3. Jones V, Smith SJ, Omar HA. Nonsexual transmission of anogenital warts in children: a retrospective analysis. ScientificWorldJournal. 2007;26;7:1896-9.
4. Syrjänen S, Puranen M. Human papillomaviruss infections in children: the potential role of maternal transmission. Crit Rev Oral Biol Med. 2000;11(2):259-74.
5. Veasey JV, Framil VMS, Nadal SR, Marta AC, Lellis RF. Verrugas genitais: correlações entre a clínica, a dermatoscopia, a microscopia confocal reflectante e a histopatologia. An Bras Dermatol. 2014;89(1):141-4.
6. Lacour DE, Trimble C. Human papillomavirus in infants: transmission, prevalence, and persistence. J Pediatr Adolesc Gynecol. 2012;25(2):93-7.
7. Forcier M, Musacchio N. An overview of human papillomavirus infection for the dermatologist: disease, diagnosis, management, and prevention. Dermatol Ther. 2010;23(5):458-76
8. Sherrard J, Riddell L. Comparison of the effectiveness of commonly used clinic-based treatments for external genital warts. Int J STD AIDS. 2007;18(6):365-8.
9. Sharquie KE, Al-Waiz MM, Al-Nuaimy AA. Condylomata acuminata in infants and young children. Topical podophyllin an effective therapy. Saudi Med J. 2005;26(3):502-3.
10. Brandt HRC, Fernandes JD, Patriota RCR, Criado PR, Belda Junior W. Tratamento do papiloma vírus humano na infância com creme de imiquimode a 5%. An Bras Dermatol. 2009;85(4):549-53
This study was carried out at the Dermatology Service of the Santa Casa de Misericórdia de São Paulo - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}