


Carlos Roberto Antonio1; Lívia Arroyo Trídico2; Cíntia Maria Garcia Marchi3; João Roberto Antonio4; Solange Corrêa Garcia Pires D'Ávila5
Introduction: Acne scars result from inflammation of acne vulgaris and are a frequent cause of complaints in dermatology practices. Atrophic scars are the most common, and may be classified into superficial, medium, and deep. There are several treatment options for deep atrophic scars, however they have limited efficacy in general, undesirable side effects and are expensive.
Objective: To evaluate the treatment of deep atrophic scars with high frequency electrosurgery.
Methods: Ten patients with deep atrophic acne scars received 3 high frequency electrosurgery treatment sessions with intervals of 1 month. The following were used to evaluate the outcome 1 month after the last session: histological aspects of selected scars as compared to the baseline; ratings attributed to the results by the patients (worsened, unchanged or improved); and standardized photographs at baseline and 1 month after the last session performed by a physician not related to the study, who also rated the results (worsened, unchanged or improved).
Results: Histological analysis evidenced a reduction in local fibrosis. All patients noticed improvement in the lesions. The evaluator dermatologist physician verified the presence of clinical improvement in all patients.
Conclusion: High frequency electrosurgery is a straightforward, inexpensive and effective method for the treatment of atrophic deep acne scars.
Keywords: CICATRIX; ACNE VULGARIS; ELECTROSURGERY
Acne is a common condition that affects roughly 80% of adolescents,1 and permanent scars may arise as a result of the inflammatory process that occurs in acne vulgaris, 2 affecting up to 95% of acne patients. Their cause is associated with both the severity of the underlying condition and the delay in beginning the treatment.3 Depressed atrophic scars are classified as non-distensible (superficial, medium and deep) and distensible.4 This is the most common type of scar, which occurs due to the action of inflammatory mediators and enzymatic degradation of collagen fibers and subcutaneous fat, resulting in lesions that often have a whitish background caused by deep fibrosis.5
According to the depth of the damage, atrophic non-distensible scars can be superficial, medium or deep, the latter being known as ice picks (up to 1mm in diameter) or dystrophic (above 1mm). They compromise the dermis in its full extension, reaching the subcutaneous. The various treatment options for this type of scar include chemical peeling, dermabrasion, ablative and non-ablative fractional lasers, punch excision, grafts, subcision, and combined methods, nevertheless these methods are generally associated with limited effectiveness, undesirable side effects and high costs.1
The search for treatment for acne scars is a frequent cause of consultation with Dermatologists since there is a negative impact on the affected patient’s quality of life.6 It is known that acne scars are associated with frustration, sadness and anxiety, and might even constitute a risk factor for suicide.7
In light of those facts and in order to find a new treatment option for atrophic and deep acne scars, the authors of the present article evaluated the use of high frequency electrosurgery (HFES) applied with a needle punctually to the scar, in order to promote immediate retraction and decrease of local fibrosis. The method is simple, cost effective, and easy to apply, yielding positive results by destroying the scar, decreasing its diameter and stimulating local tissue regeneration.
A prospective, non-randomized study was carried out with 10 patients from the Dermatologic Surgery Ambulatory of the Facudade de Medicina de São José do Rio Preto (Famerp) clinically diagnosed with deep atrophic acne scars (Figure 1). The selected patients did not bear active acne, with some bearing Grade I lesions only. Higher-grade acne lesions were excluded from the selection. The patients were not receiving any type of treatment for scars and were in use of sunscreen. For the control of facial oiliness, only soap was used.
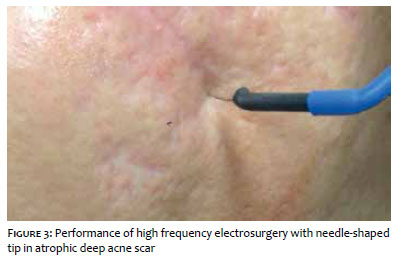
The selected patients received HFES treatment performed with the assistance of a fine tip in the shape of a needle. The application was carried out with a Wavetronic® device (Loktal, São Paulo, Brazil) in a way that the needle-shaped tip or a 30G needle (13 x 0.3mm) was placed in the center of the atrophic scar, exerting pressure on the skin, with the 5W electric current being subsequently activated, with the device set at the mode “Blend/Low Blend” (Figures 2 and 3). Immediately after the electrical discharge, the scar underwent retraction, elevation and whitening (Figures 4 and 5).
Three sessions were performed in each patient at one-month intervals. The evaluation methods employed were: i) biopsies of selected scars for anatomopathological study, before and one month after the last session; ii) subjective evaluation of the patients’ opinion (outcomes received one of the following ratings: worsening, absence of improvement or improvement of the lesions); and iii) evaluation of standardized photographs before and one month after the last session. A physician not related to the study evaluated the images, also attributing the ratings worsening, absence of improvement or improvement to the lesions.
The objective analysis of the photographs, performed by a dermatologist physician not related to the study, attributed the rating improvement to the scars of all participants. Reduction of local fibrosis and scar elevation were observed after the procedure (Figure 6).
In addition, in the subjective evaluation carried out by the patients, all participants attributed the rating improvement of the lesion to the final outcomes.
After the electrosurgery session, mild local erythemas emerged, with the subsequent formation of a discrete crust on the scar that resolved within 7 to 9 days after the procedure. The patients were instructed not to manipulate the crusts and to use sunscreen in the lesion’s location.
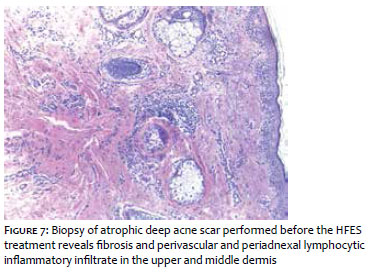
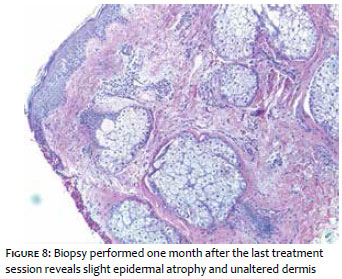
In the anatomopathological study of the biopsies performed before the procedure, fibrosis and perivascular and periadnexal lymphocytic inflammatory infiltrate were observed in the upper and middle dermis (Figure 7). It was possible to observe only epidermal atrophy in the biopsy performed one month after the last treatment session, with the dermis remaining unaltered, with absence of fibrosis and inflammatory infiltrate (Figure 8).
For being a simple and traditional procedure, HFES has been used to treat several skin conditions for more than 50 years, having become part of the routine of most dermatologist physicians. It acts by means of a high-frequency electromagnetic wave, which is transformed into heat due to local resistance when penetrating the tissues, resulting in the boiling of the intracellular water, causing the rupture of the cell due to an increase in its internal pressure, in turn generating tissue clotting and coagulation.4,8,9
As a result, when HFES is applied to atrophic and deep acne scars, destruction of local fibrosis and consequent tissue remodeling takes place, which can be seen in the biopsies performed after the procedure.
There are other options, simpler and less expensive than laser therapy, for treating atrophic scars, however they may be associated with some undesirable side effects. The CROSS technique (Chemical Reconstruction of Skin Scars) consists in the spot application of trichloroacetic acid on atrophic scars in order to stimulate neocollagenesis. However, this technique may be associated with adverse events such as hypopigmentation, hyperpigmentation and formation of residual scars on normal skin around the initial scar. 10,11
The technique that employs full thickness skin micrografts performed with minipunchs consists of the excision of the atrophic scars using punchs, followed by the implantation of micrografts at the site of excision. The scar is removed and replaced by a slightly larger skin graft, usually harvested from the postauricular area. Some grafts will level with the skin’s surface; others will remain elevated, meaning that a new therapeutic intervention is often necessary to achieve leveling.
The application of HFES with the needle-shaped tip allows that the electrosurgery’s action be restricted to the site of fibrosis, avoiding possible complications secondary to the application in the healthy skin around the lesion. Also, it provides enhanced safety in higher phototypes. In this manner, the present study allowed the observation of a new, straightforward and cost effective option for efficaciously treating acne scars, which is one of the major causes of consultations to dermatologist physicians.
Based on the reported cases, HFES was proven effective and safe in the treatment of atrophic and deep acne scars. As a result, it emerges as a more accessible treatment option for both patients and physicians, since it employs a technology that is widely used in dermatology practices and can contribute to the treatment of an important complaint that has a considerable psychosocial impact.
Carlos Roberto Antonio:
Study guidance, creator of the described technique.
Lívia Arroyo Trídico: Patient follow-up.
Cíntia Maria Garcia Marchi:
application of the technique on the selected patients.
Joao Roberto Antonio:
Head of the ambulatory where the study was carried out, preparation of the paper.
Solange Corrêa Garcia Pires D'Ávila:
Histological analysis of biopsies performed before and after the procedure.
1. Gozali MV, Zhou B. Effective treatments of atrophic acne scars. J Clin Aesthet Dermatol. 2015;8(5):33-40.
2. Fabbrocini G, Annunziata MC, D'Arco V, De Vita V, Lodi G, Mauriello MC, Pastore F, Monfrecola G. Acne scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010;2010:893080.
3. Goodman GJ. Postacne scarring: a review of its pathophysiology and treatment. Dermatol Surg. 2000;26(9):857-71.
4. Palermo EC. Eletrocirurgia de Alta Freqüência (ECAF). Ipele Dermatologia livro online. São José do Rio Preto: Ipele Network; 2002 [cited 2016 Oct 10]. Available from: https://www.ipele.com.br/livro/
5. Fife D. Practical evaluation and management of atrophic acne scars: tips for the general dermatologist. J Clin Aesthet Dermatol. 2011;4(8):50-7.
6. Dréno B, Tan J, Kang S, Rueda MJ, Torres Lozada V, Bettoli V, et al. How people with facial acne scars are perceived in society: an online survey. Dermatol Ther (Heidelb). 2016;6(2):207-18.
7. Cotterill JA, Cunliffe WJ. Suicide in dermatological patients. Br J Dermatol. 1997;137(2):246–50.
8. Hainer BL. Fundamentals Of Electrosurgery. J Am Board Farm Pract. 1991;4(6):419-26.
9. Massarweh NN, Cosgriff N, Slakey DP. Electrosurgery: history, principles, and current and future uses. J Am Coll Surg. 2006;202(3):520-30.
10. Rose AE. Therapeutic update on acne scarring. J Drugs Dermatol. 2014;13(6):651-4.
11. Khunger N, Bhardwaj D, Khunger M. Evaluation of CROSS technique with 100% TCA in the management of ice pick acne scars in darker skin types. J Cosmet Dermatol. 2011;10(1):51-7.
12. Gozali MV, Zhou B. Effective treatments of atrophic acne scars. J Clin Aesthet Dermatol. 2015;8(5):33-40.
This study was carried out at the Faculdade de Medicina de São José do Rio Preto (Famerp) - São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}