


Valéria Romero1; Lucas Offenbecker Guerra2; Laura Aiello3; Gislaine Ricci Leonardi4
Introduction: Overexposure of the skin to the sunlight can cause photoaging and promote the emergence of malignant neoplasms. Sunscreens are used to prevent these alterations and may occasionally cause adverse reactions in children and adults.
Objective: To analyze the frequency and types of adverse reactions caused by sunscreens in adults and children.
Methods: Data analysis of in vivo, non-invasive clinical studies performed at a clinical research institute.
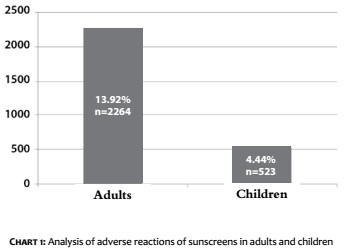
Results: Data from 2,263 adults and 523 children were evaluated, with 13.92% and 4.44%, respectively, presenting some type of reaction.
Conclusions: Sunscreens are effective in preventing photoaging and skin cancer. Cosmetic formulations containing sunscreens may cause adverse reactions with low prevalence.
Keywords: SUNSCREENING AGENTS; CONTROL AND SANITARY SUPERVISION OF COSMETICS; SUN PROTECTION FACTOR; COSMETICS
The skin is the human body’s organ that comes in contact with the internal and external environments, thus exerting protective functions against microorganisms, harmful substances and radiations, in addition to helping to keep body temperature constant, preventing excessive loss of water, and producing vitamin D.1 The skin’s degree of exposure to the sun and its constant tanning can influence photoaging. Individuals exposed to sunny climates, living in regions where the ultraviolet (UV) radiation index is normally high, and who lack photoprotection habits may experience a higher degree of photoaging.2 Another long-term consequence of excessive UV exposure is linked to cutaneous malignant neoplasms, which range from precancerous lesions – such as actinic keratosis – to invasive cancers – such as melanoma.3
Ultraviolet radiation is classified into A (UVA), B (UVB) and C (UVC), with UVC radiation being filtered by the Earth’s ozone layer. Ultraviolet radiation type A (320nm-400nm) has a greater ability to penetrate the skin and is involved in most photoallergic reactions, some phototoxic reactions, carcinogenesis, and cutaneous photoaging.4 Ultraviolet radiation was classified as a Class I carcinogen by the International Agency for Research on Cancer.5 The adverse effects range from cell necrosis to genomic instability.6,7 Although UVB has been classified as a “causer of sunburn” and UVA as a “causer aging” by the lay public, a photobiological research focused on genotoxicity and immunomodulation found that skin cancer can be caused by both UVA and UVB radiation.8,7
Epidemiological data show a significant increase in the incidence of cutaneous neoplasms, especially non-melanoma epidermal tumors, in several countries. In 2016, the Brazilian National Cancer Institute (Inca) estimated 80,850 new cases of nonmelanoma skin cancer in men and 94,910 in women. These figures correspond to an estimated risk of 81.66 new cases per 100,000 men and 91.98 per 100,000 women.
Sunscreens have become widely used for the prevention of sun damage in the short and long terms, and are classified and regulated as medicaments in the USA, Canada and Australia, and as cosmetics in Europe.9,10 In Brazil, according to the National Sanitary Surveillance Agency (ANVISA), a sunscreen is any cosmetic preparation intended to come into contact with the skin and lips for the exclusive or main purpose of protection against UVB and UVA rays by absorbing, dispersing or reflecting the radiation.11 Sunscreens are currently influenced by the fast paced emergence of innovations, meaning that their formulations may present multiple UV blocks, in addition to excipients and other ingredients.12 The use of sunscreens has been considered one of the most effective measures in the prevention of cutaneous neoplasias. Public health authorities recommend regular use in activities that imply exposure to the sunlight, such as working and practicing sports outdoors. However, the use of sunscreen alone should never be combined with increased exposure to the sunlight.13 Some studies have suggested the existence of correlation between the use of sunscreen and melanoma, suggesting that the use of sunscreen increases the users’ time of exposure to the sunlight, due to the fact that they would deem themselves exempt from the potential damage caused by the sun. It is possible to conclude, therefore, that the greater exposure to UV rays would lead to malignant alterations.14,15 For this reason, photo-education campaigns have been stimulated and carried out, mainly in tropical countries. A recent European study evidenced that 87.1% of 1,816 dermatological patients reported the use of sunscreen.16
For adequate efficacy, a sunscreen formulation must contain chemical elements with absorption spectrum in the UVA and UVB radiation bands, in addition to being photostable. Moreover, for the ideal protective effect, the filter must be able to form a homogeneous film, distributing its ingredients evenly across the skin’s surface.17 Children need special photoprotection, as they are more susceptible to environmental threats than adults. Exposure to the sun during childhood and adolescence seems to set the conditions for the development of both melanoma and non-melanoma epidermal tumors in adulthood.13 A study on the use of sunscreens in children included 157 patients aged three to 17 years. Ten children (6.4%) presented positive responses to contact phototesting when a standardized sequence of nine UV filters –or their own sunscreens – were applied: 4.5% reacted to UV filters and 5.7% reacted to their own sunscreens. The UV filters that caused reactions more frequently were benzophenone-3 and octyl methoxycinnamate.18
Photo-education campaigns have been important due to the fact that currently there is a lack of knowledge about photoprotection, justifying the necessity of an educational effort linked to the subject. Photo-education shows that sunscreens are not the only way to protect human skin from excessive exposure to the sun and that there are other forms of protection, such as the use of tents, sunglasses, photoprotective clothing and observation of the hours of risky exposure (10:00 am to 4:00 pm). Protection will be very effective when the various measures to reduce exposure to sunlight are used in combination.
The objective of the present study was to analyze adverse reactions caused by sunscreens in adults and children, based on the results of in vivo, non-invasive clinical studies, performed at the Instituto de Pesquisa Dermato-Cosmética, located in the city of Campinas, São Paulo (SP), Brazil.
An open, prospective clinical study was carried out from January 2014 to December 2015.
The recruitment of participants was conducted by Allergisa - Pesquisa DermatoCosmética Ltda., located in Campinas, São Paulo (SP), Brazil, where the analysis of the database relating to the results also took place. All clinical trials analyzed were conducted in accordance with the Declaration of Helsinki, the Brazilian National Health Council (CNS) Resolution No. 466/12 ANVISA, and the Document of the Americas and ICH E6 of Good Clinical Practice, complying with the directives established by the Research Ethics Committee of the Institution. A total of 2,263 adults over the age of 18 and 523 children over 6 years of age were evaluated. The different clinical trials were based on the dermatological tests model described in ANVISA’s safety evaluation guide for cosmetic products (Brazil, 2003).19
The volunteers were informed of the purpose, methodology and duration, advantages and clinical restrictions related to the study. Participants confirmed their interest in taking part by signing a Term of Consent. The technical documentation and database were made available to the researchers conducting the present study and will be kept on file for 5 years.
The participants of the analyzed surveys are healthy individuals, without complaints or reports of exacerbated cutaneous sensitivity and absence of history of reactions to the studied product’s category. The products were used for a minimum of 21 days. The sunscreens application areas were the body and face. The volunteers were instructed on use of the products, with those observing the guidelines continuously throughout the proposed period having been selected for analysis. In cases of adverse events, dermatologist physician physicians evaluated the participants.
Based on the tabulation of the results analyzed, it was found that 13.92% of the adults and 4.44% of the children presented adverse reactions to the sunscreens (Figure 1).
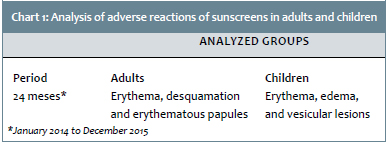
During the course and at the end of each noninvasive clinical trial of the sunscreens, participants were given the opportunity to report possible adverse reactions. All possibilities of adverse reactions or clinical signs (depicted in Chart 1) were evaluated, diagnosed and treated by a dermatologist physician.
Adverse reactions diagnosed in adults by the dermatologist physician during the study period were: erythema, desquamation and erythematous papules and, in children, erythema, edema and vesicles. Adverse reactions were reported by the participants, however the final clinical diagnosis and treatment were conducted and completed by a dermatologist of the institution where the study was carried out.
The sunscreens market is constantly growing due to the fact that people are increasingly aware of the harmful effects of UV radiation, and also because of scientific progress and the emergence of new active principles, excipients and UV blockers.12
The compatibility among the components of a sunscreen, its effectiveness and safety are of paramount importance for safe use. The adverse reactions to these formulations are not frequent; nonetheless, the sensitization to a sunscreen’s components may occur. It is worth noting that the use of sunscreens does not enable prolonged exposure to the sunlight, meaning that it is necessary to avoid exposure between 10:00am and 04:00pm in addition to make use of physical methods of protection against the sun, such as gloves and hats, among others.9
Regarding children, especially those under six years of age, photoprotection should be sought by associating the use of sunscreens with protective clothing, avoiding exposure at peak times of solar radiation.20-22 This is due to the fact that some factors, such as the correct amount used and homogenization of the sunscreen over the entire body surface that will be exposed, are implied in the effectiveness of the photoprotection. Despite the fact that tests are performed prior to releasing the products in the marketplace, adverse reactions to cosmetics due to individual susceptibility to formulation components should also be considered,.23,24
Adverse reactions to sunscreens are described as sensations of local heat, erythema and pruritus, which may or may not disappear after a few hours. These phenomena were well documented, especially regarding sunscreens used in the 1990s.25,26
Several UV filters that are marketed as organic products are known to trigger allergic and photoallergic reactions, accounting for 55% to 80% of these cases.27-29 The lipophilic nature of organic UV blockers as well as their small molecules allow greater penetration into the skin, a basic requirement for the onset of an allergic response.30 Adverse reactions usually occur in the face, in special around the eyes.26 Pustisek et al. 9 reported that adverse reactions to sunscreens are relatively rare and include irritation, and contact urticaria and dermatitis by primary, allergic, phototoxic and photoallergic irritations.
In an Australian study, 703 individuals applied a water-resistant sunscreen containing SPF 15 on a daily basis. The results indicated that 114 (18.9%) of them developed adverse reactions to the sunscreen, with these reactions being diagnosed as inflammatory or acneiform eruptions, as well as contact urticarias.31
In the present study, the clinical signs of adverse reactions in children assessed and exposed to sunscreens were erythema, edema and vesicular lesions. In adults, clinically evident adverse reactions were erythema, desquamation and papules (Chart 1). The Brazilian National Sanitary Surveillance Agency (ANVISA) stated in 2013 that 7% of the 136 notifications of adverse events received by its cosmetics oversight sector referred to sunscreens.32
Despite adverse effects, sunscreens are important for protecting the skin from UVA and UVB radiation, and are effective in preventing damage caused by the sun, however they should be combined to other protective measures. Photo-education campaigns should be encouraged, as they are effective in preventing serious damage to the skin caused by excessive exposure to the sunlight. There is a clear need for mobilization of health authorities and governments, which should turn their attention to the treatment, as well as to the prevention and education of the general population regarding diseases of the skin.20,33
Sunscreens are effective in preventing photoaging and skin cancer, and their use has increased over the last decade, as people are increasingly aware of the harmful effects of excessive UV radiation. Diverse solar radiation blockers contained in the cosmetic formulation of sunscreens can cause adverse reactions, with low prevalence.
1. Campos PMBGM, Mercúrio DG. Farmacologia e a pele. Rev Bras Med. 2009;66(4):15-21.
2. Rabe JH, Mamelak AJ, McElgunn P J, Morison WL, Sauder D N. Photoaging: mechanisms and repair. J Am Acad Dermatol. 2006;55(1):1-19.
3. Kim RH, Armstrong AW. Nonmelanoma skin câncer. Dermatol Clin. 2012;30(1):215-39.
4. Schalka S, Villarejo-Vitale MA, Agelune CM, Bombarda PCP. Benefícios do uso de um composto contendo extrato de polypodium loucotomos na redução da pigmentação e do eritema decorrentes da radiação ultravioleta. Surg Cosmet Dermatol. 2014;6(4):344-8.
5. El Ghissassi F, Baan R, Straif K, Grosse Y, Secretan B, Bouvard V et al. A review of human carcinogens--part D: radiation. Lancet Oncol. 2009;10(8):751-2.
6. González E, González S. Drug photosensitivity, idiopathic photodermatoses, and sunscreens. J Am Acad Dermatol. 1996;35(6):871-885.
Matts PJ. Solar ultraviolet radiation: de¿nitions and terminology. Dermatol Clin. 2006;24(1):1-8.
8. Agar NS, Halliday GM, Barnetson RS, Ananthaswamy HN, Wheeler M, Jones AM. The basal layer in human squamous tumors harbors more UVA than UVB fingerprint mutations: a role for UVA in human skin carcinogenesis. Proc Natl Acad Sci U S A. 2004;101(14):4954-9.
9. Pustisek N, Lipozenicic J, Ljubojevic S. A review of sunscreens and their adverse reactions. Acta Dermatovenerol Croat. 2005;13(1):28-35.
10. FDA.gov. [Internet]. U.S. Food and Drug Administration. Consumer Washington: The FDA Sheds Light on Sunscreens. [updated 2012 May 17; cited 2016 Nov 12]. U.S. Food and Drug Administration Website. Available from: http://www.fda.gov/forconsumers/consumerupdates/ucm258416.htm.
11. ANVISA.org [Internet]. Brasília: Agência Nacional de Vigilância Sanitária. Resolução - RDC n° 30 de 1° de junho de 2012 Regulamento técnico Mercosul sobre protetores solares em cosméticos. [acesso 23 Dez 2016]. Disponível em: www.portal.anvisa.gov.br
12. Hong H, Rua D, Sakkia S, Selvaraj C, Ge W, Tong W. Consensus modeling for prediction of estrogenic activity of ingredients commonly used in sunscreen products. Int J Environ Res Public Health. 2016;13(10):958.
13. WHO.int [Internet]. Washington: World Health Organization (WHO). Sun Protection. [cited 2016 Oct 26]. Available from: http//www.who.int/uv/sun_protection/en.
14. Autier P, Doré JF, Négrier S, Liénard D, Panizzon R, Lejeune FJ, et al. Sunscreen use and duration of sun exposure: a double blind, randomized trial. J Natl Cancer Inst. 1999;91(15):1304-9.
15. Westerdahl J, Ingvar C, Måsbäck A, Olsson H. Sunscreen use and malignant melanoma. Int J Cancer. 2000;87(1):145-150.
16. Suppa M, Argenziano G, Moscarella E, Hofmann-Wellenhof R, Thomas L, Catricalà C, et al. Selective sunscreen applications on nevi: frequency and determinants of a wrong sunprotective behaviour. J Eur Acad Dermatol Venereol. 2014;28(3):348-354.
17. Forestier, S. Rationale for sunscreen development. J Am Acad Dermatol. 2008;58(5 Suppl 2):S133-S138.
18. Haylett A, Chiang YZ, Nie Z, Ling TC, Rhodes LE. Sunscreen photopatch testing: a series of 157 children. Br J Dermatol. 2014;171(2): 370-375.
19. ANVISA.org [Internet]. Brasília: Agência Nacional de Vigilância Sanitária. Guia para avaliação da segurança de produtos cosméticos, 2003. [acesso 23 Dez 2016]. Disponível em: http://www.anvisa.gov.br/cosmeticos/guia/index.htm>
20. Leonardi GR, Banin TM, Corazza FG, Fegadolli C. Education about protection against solar radiation for teachers teaching young children: a contribution to promote school health. Biomed Biopharm Res. 2014; (11)2:179-189.
21. Abeck D, Feucht J, Schäfer T, Behrendt H, Krämer U, Ring J. Parental sun protection management in preschool children. Photodermatol Photoimmunol Photomed. 2000;16(3):139-143.
22. Bryden AM, Moseley H, Ibbotson SH, Chowdhury MM, Beck MH, Bourke J et al. Photopatch testing of 1155 patients: results of the UK multicentre photopatch study group. Br J Dermatol. 2006;155(4):737-47.
23. Chorilli M, Scarpa MV, Leonardi GR, Franco YO. Toxicologia dos cosméticos. Lat Am J Pharm. 2007;26(1):144-54.
24. Huf G, Rito PN, Presgrave RF, Boas MHSV. Adverse reactions to cosmetic products and the Notification System in Health Surveillance: a survey. Rev Bras Epidemiol. 2013;16(4):1017-20.
25. Dromgoole SH, Maibach HI. Sunscreening agent intolerance: contact and photocontact sensitization and contact urticaria. J Am Acad Dermatol 1990;22(6 Pt1):1068-78.
26. Fischer T, Bergström K. Evaluation of customers' complaints about sunscreen cosmetics sold by the Swedish pharmaceutical company. Contact Dermatitis 1991;25(5):319-22.
27. Rodríguez E, Valbuena MC, Rey M, Porras de Quintana L. Causal agents of photoallergic contact dermatitis diagnosed in the national institute of dermatology of Colombia. Photodermatol Photoimmunol Photomed. 2006;22(4):189-192.
28. Cardoso J, Canelas MM, Gonçalo M, Figueiredo A. Photopatch testing with an extended series of photoallergens: a 5-year study. Contact Dermatitis. 2009;60(6):325-9.
29. Greenspoon J, Ahluwalia R, Juma N, Rosen CF. Allergic and photoallergic contact dermatitis: a 10-year experience. Dermatitis. 2013;24(1):29-32.
30. Stiefel C, Scwack W. Photoprtotection in changing times - UV filter efficacy and safety, sensitization processes and regulatory aspects. Int J Cosmet Sci. 2015;37(1):2-30.
31. Foley P, Nixon R, Marks R, Frowen K, Thompson S. The frequency of reactions to sunscreens: results of a longitudinal population-based study on the regular use of sunscreens in Australia. Br Dermatol. 1993;128(5):512-518.
32. ANVISA.org [Internet]. Brasília: Agência Nacional de Vigilância Sanitária: Cosmetovigilância Brasil. [acesso 26 Out 2016]. Disponível em: http://portal.anvisa.gov.br/cosmeticos
33. Pustisek N, Sikanic-Dugic N, Hirsl-Hecej V, Domljan ML. Acute skin sun damage in children and its consequences in adults. Coll Antropol. 2010;34(Suppl 2):233-237.
This study was carried out at the Instituto de Pesquisa Investiga Allergisa - Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}