


John Verrinder Veasey1; José Antonio Jabur da Cunha2; Marina Pipa3; Carla Russo Zukanovich Funchal4; Rute Facchini Lellis5
Introduction: Subcutaneous mycoses caused by dematiaceous fungi are classified according to their characteristics in the tissue: chromoblastomycosis (with the presence of fumagoid corpuscles), phaeohyphomycosis (with dematiaceous septate hyphae) and eumicetoma (with grains composed of septate hyphae). Several treatments are proposed, among them, surgical excision. Surgical treatment is more indicated in cases where there is localized infection and where excision is possible, yielding good therapeutic outcomes and low recurrence rates.
Objective: To describe the experience of a dermatological service in the surgical treatment of subcutaneous mycosis cases caused by dematiaceous fungi, discussing the surgical approach and its results.
Methods: A retrospective study was carried out with the descriptive analysis of cases treated from April 2014 to December 2016, at a dermatological clinic in the Brazilian Southeast city of São Paulo. All cases diagnosed with subcutaneous mycoses caused by dematiaceous fungi were included and surgically treated with total exeresis of the lesion.
Results: A total of 7 cases were analyzed – 2 eumicetomas, 1 chromoblastomycosis and 4 phaeohyphomycoses. Only one on the cases was not treated at an ambulatory surgical center. All cases progressed without sequelae or recurrences during the clinical follow-up.
Conclusions: When surgical treatment is possible, the exeresis of the lesion is a good therapeutic option in cases of subcutaneous mycoses caused by dematiaceous fungi.
Keywords: CHROMOBLASTOMYCOSIS; PHAEOHYPHOMYCOSIS; BACTERIAL INFECTIONS AND MYCOSES; MYCOSIS; MYCETOMA; AMBULATORY SURGICAL PROCEDURES; BLOODLESS MEDICAL AND SURGICAL PROCEDURES; HISTOLOGY; THERAPEUTICS
Subcutaneous mycoses are fungal infections located in the deep layers of the skin. They can be caused by both hyaline fungi, with no pigment in their structure, and by dematiaceous fungi that present melanin in their cellular wall.1,2 Dematiaceous fungi are found throughout the planet, with a predilection for tropical areas, inhabiting the soil and vegetables (geophilic fungi).3-5
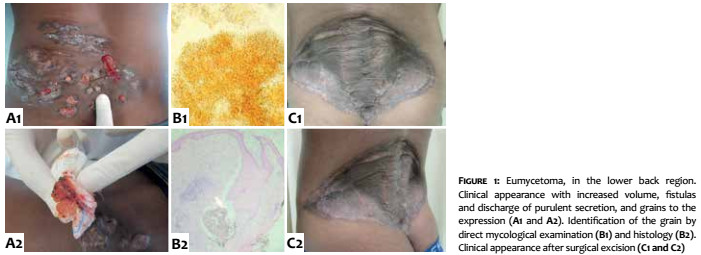
Subcutaneous mycoses caused by dematiaceous fungi (SMCDF) are classified according to their appearance in the tissue: chromoblastomycosis with presence of fumagoid corpuscles, phaeohyphomycosis with dematiaceous septate hyphae and eumycetoma with grains composed of dematiaceous septate hyphae.1,6 These structures can be visualized in the direct mycological examination of the material harvested from the lesion or in the tissue biopsy histological analysis. Fungus culture is required to determine the agent’s species.2,3,6,7
Several treatments are proposed in these cases, from the use of antifungals to thermotherapy and surgical excision. The choice between these therapies is made based on the analysis of several factors, such as manifestation of the lesion, clinical conditions and the patient’s comorbidities, in addition to the availability of treatment when medical advice is sought.2,4,8-10
The present study is aimed at describing the experience of a dermatological clinic in the city of São Paulo (SP) - Brazil, in the surgical treatment of SMCDF cases, discussing surgical approaches and results.
A retrospective study was conducted with the descriptive analysis of cases treated from April 2014 to December 2016, at a tertiary dermatologic clinic in the city of São Paulo, Brazil. All cases diagnosed with SMCDF that underwent surgical treatment with total lesion excision were included.
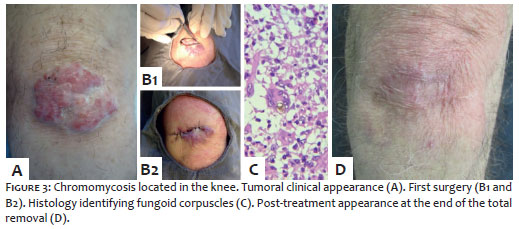
Case 1 consisted of a eumycetoma initially treated with antifungals for 24 months, without success. After having been treated surgically by the plastic surgery team, it progressed with healing (Figure 1). Case 2 consisted of a nodular lesion that was promptly removed after eumycetoma diagnosis (Figure 2). Case 3 involved a chromomycosis located in the patient’s knee, that was not treated in a single surgical time due to the possibility of dehiscence: three sessions were performed, with an excellent final outcome (Figure 3).
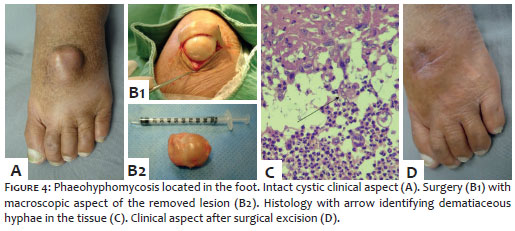
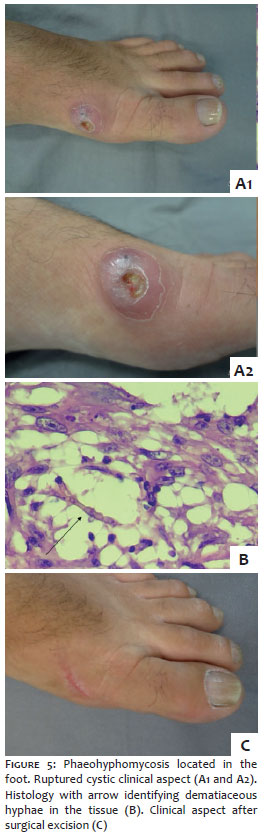
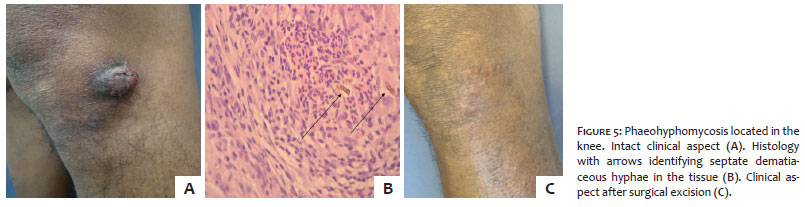
Cases 4, 5 and 6 had lesions similar to each other, easily removed with surgical technique. Cases 4 and 5 showed cystic lesions on the feet – a classic symptom of phaeohyphomycosis (Figures 4 and 5). In case 4, there was an attempt of using drug therapy prior to the procedure, without any response. Case 6 presented a solid tumor near the knee (Figure 6) that was approached with total lesion excision (fusiform excisional biopsy). This patient had other cystic phaeohyphomycosis lesions in the limbs that were not surgically accessible, having been treated with antifungal after biopsy, which explains the prolonged medication time after the approach.
Case 7 had multiple phaeohyphomycosis lesions on the dorsum of the hand, for the patient used plants’ thorns to puncture lesions, inoculating new dematiaceous hyphae with this habit. Several excisional sessions were carried out with a sterile needle up until healing was achieved (Figure 7).
There were seven cases in total: 2 eumycetomas, 1 chromoblastomycosis and 4 phaeohyphomycosis. Only one of these cases was not treated in ambulatorial surgical center setting. None presented recurrence after the surgical treatment. The characteristics of the seven cases are detailed in Table 1. The diagnoses were defined based on the association of the clinical appearances, isolation of the etiological agents and the morphology observed in the histology of the tissues.
All cases progressed without sequelae and absence of recurrences in the clinical follow-up.
Currently, SMCDF treatment can be divided into medicament and / or surgical based. Surgical treatment is more indicated in cases where there is localized infection and exeresis is feasible.1,10 Although widely used, medicament based treatment should be introduced with caution, since it is protracted, and patients with SMCDF frequently are elderly and have conditions that alone require their own daily doses of medication.3,8
In the cases presented in this paper, surgical removal was proven a safe option. The authors did not observe any perioperative complications, such as infection, dehiscence or collections formation. In addition, despite the advanced age or immunosuppression associated with most cases, it was not possible to observe any clinical complication resulting from the operative event. Except for Case 1 (Figure 1), all patients were operated in an ambulatorial basis under local anesthesia, which simplified the treatment and considerably reduced the morbidity and risk of procedure.
Surgical treatment of SMCDF, regardless of whether or not it was associated with systemic antifungal therapy, did not predispose to the dissemination or implantation of the infectious agent. In the period of clinical follow-up ranging from 14 to 70 months (mean = 38.4 months), no new lesions were observed at the site of surgical treatment.
Due to the multiplicity of clinical presentations, the surgical techniques employed varied according to the specificities of each case. Cases characterized by subcutaneous nodules or cysts (Cases 2, 4 and 5) were well delimited, which facilitated dissection and the complete removal of the lesion. Tumor-like cases (Cases 3 and 6) were removed using fusiform excision and direct closure. Due to the size and anatomical location of the lesion in Case 3, a decision was made for a three-stage excision. This approach did not trigger the cutaneous implantation of the agent or any other postoperative complication.
In the authors’ experience, surgical treatment was proven effective, simple and safe in cases where the infection is anatomically delimited. The antifungal agents’ toxicity associated with the usually affected patient’s clinical / immunological profile, makes surgery an optimal therapeutic option, which should be regarded as the first-choice treatment whenever surgical removal is feasible.
1. Hoffmann CC, Danucalov IP, Purim KSM, Queiroz-Telles F. Infecções causadas por fungos demácios e suas correlações anátomo-clinicas. An Bras Dermatol. 2011;86(1):138-41.
2. Revankar SG. Phaeohyphomycosis. Infect Dis Clin North Am. 2006;20(3):609-20.
3. Nenoff P, van de Sande WW, Fahal AH, Reinel D, Schöfer H. Eumycetoma and actinomycetoma - an update on causative agents, epidemiology, pathogenesis, diagnostics and therapy. J Eur Acad Dermatol Venereol. 2015;29(10):1873-83.
4. Correia RTM, Valente NYS, Criado PR, Martins JEC. Cromoblastomicose: relato de 27 casos e revisão da literatura. An Bras Dermatol. 2010;85(4):448-54.
5. Zijlstra EE, van de Sande WW, Welsh O, Mahgoub ES, Goodfellow M, Fahal AH. Mycetoma: a unique neglected tropical disease. Lancet Infect Dis. 2016;16(1):100-12.
6. Wong EH, Revankar SG. Dematiaceous molds. Infect Dis Clin North Am. 2016;30(1):165-78.
7. Revankar SG, Sutton DA. Melanized fungi in human disease. Clin Microbiol Rev. 2010;23(4):884-928.
8. Oliveira WRP, Borsato MFL, Dabronzo MLD, Festa Neto C, Rocha LA, Nunes RS. Feoifomicose em transplante renal: relato de dois casos. An Bras Dermatol. 2016;91(1):93-6.
9. Welsh O, Al-Abdely HM, Salinas-Carmona MC, Fahal AH. Mycetoma medical therapy. PLOS Negl Trop Dis 2014;8(10):e3218
10. Silveira F, Nucci M. Emergence of black moulds in fungal disease: epidemiology and therapy. Curr Opin Infect Dis. 2001;14(6):679-84.
This study was carried out at the Dermatology Service, Santa Casa de São Paulo - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}