


Camila Araujo Scharf Pinto1; Priscila Regina Orso Rebellato2; Juliano Vilaverde Schmitt3; Deborah Skusa de Torre4
Introduction: The application of botulinum toxin in the perioral region is a minimally invasive procedure that leads to substantial improvement in the signs of aging in addition to increasing the volume of the lips. However literature on this procedure is still scarce.
Objective: To evaluate changes in shape and volume of the lips, as well as the patients' satisfaction after the application of botulinum toxin in perioral lines.
Methods: Nineteen patients underwent evaluation, photographic record and measurements following the application of botulinum toxin in the perioral region, being subsequently assessed for changes in the lips and satisfaction.
Results: Most of the patients rated their lips as moderately or significantly more attractive after the application of botulinum toxin (p = 0.039). Fifteen women deemed the changes in the lips as a major factor in the overall improvement of their faces.
Conclusions: The use of botulinum toxin in the perioral region leads to the elevation of the upper lip, causing the shortening of the philtrum and the extension of the vermilion. The application of botulinum toxin in the vermilion's border leads to the relaxation of the orbicularis muscle, favoring a more intense tonus effect arising from the upper lip lifting muscles. The patients' satisfaction with the appearance of their lips was evaluated by four additional questions (linked to the lip's shape, volume, attraction and beauty), receiving positive answers. Side effects were minimal.
Keywords: LIP; BOTULINUM TOXINS, TYPE A; BOTULINUM TOXINS
Botulinum toxin is an exotoxin produced by Clostridium botulinum, a gram-positive anaerobic bacterium. There are eight bacterial serotypes (A, B, C alpha, C beta, D, E, F and G) that produce seven distinct exotoxins. Type A, B and E are most commonly associated with botulism in humans. The toxin’s action’s final path is to prevent the release of acetylcholine at the neuromuscular junction of the striated muscles thus producing chemical denervation and resulting muscular paralysis.1
In the last three decades, botulinum toxin has been used for therapeutic purposes in a number of conditions. Botulinum toxin type A was first approved in 1989 for use in strabismus, blepharospasm and hemifacial spasm. Then types A and B were approved for the treatment of cervical dystonias. More recently, type A has been approved for aesthetic purposes, palmoplantar hyperhidrosis and treatment of migraine and chronic tension headache.2
The application of botulinum toxin in the perioral region is a rapid and minimally invasive procedure. In addition, recent studies have shown substantial improvement in the signs of aging, including increased lip volume.3,4 There are reports of botulinum toxin use for other purposes, such as gingival smile correction or perioral synkinesia, however there is scarce literature on the evaluation of the increase in the lip’s volume with the application of the toxin in the perioral rythids.5,6
To evaluate changes in shape and volume of the lips after the application of botulinum toxin in the perioral ridges, as well as the patients’ satisfaction with the shape of the lips.
A prospective, interventional, uncontrolled and non-randomized study was carried out. An already established technique was evaluated by this study. The patients were selected at the Dermatology Ambulatory of the Hospital Universitário Evangélico de Curitiba (Curitiba city, PR, Brazil), from July 2014 to August 2015. Adults who already wanted to undergo the application of botulinum toxin for aesthetic purposes were selected. There was no gender or phototype restriction, and only patients older than 18 were included.
Patients who had already undergone another type of treatment for increasing the volume of the lips were excluded. Other exclusion criteria were: history of intolerance to the drug, pregnancy, difficulty to communicate clearly, active use of anticoagulants, presence of scars, deformities or pathological anatomical alterations in the lips and autoimmune diseases.
After signing the Informed Term of Consent, the patients were evaluated with the assistance of a questionnaire containing questions related to the satisfaction with their lips. Also, measurements and standardized photographs of the lips were taken.
Botulinum toxin was then applied for aesthetic purposes, at individually defined sites in the patients, totaling 4 points in the upper lip.
The Dysport® 500U toxin (Ipsen®, Paris, France) was used diluted in 0.9% saline in the ratio 1:1.7 and kept under refrigeration (2°C to 8°C). Zero point five (0.5) UI was applied in each of the four points of the upper lip’s perioral rhytids, along the vermilion border.
The selected patients returned for reassessment after 3 weeks, when measurements were repeated and standardized photographs were taken for comparative purposes.
Evaluation criteria
The evaluation of the outcomes was performed through the analysis of categorical and continuous variables. Changes in the lip’s shape and size were gauged through measurements taken with a pachymeter, while the patient’s satisfaction with the treatment was assessed using semi-quantitative questionnaires, and the impression of the blinded specialist physicians through the evaluation of standardized photographs.
Statistical evaluation
The data were compared between the different experimental timepoints of the evaluation and clinical re-assessment. The chi-squared test was used for analyzing the adherence and trend, while the Fisher’s exact test was used to compare categorical variables. The data was expressed in absolute values and proportions, and the associations, in odds ratios. The paired Student’s t-test and Wilcoxon’s test were used for comparing continuous variables. The normality of distributions was assessed using the Shapiro-Wilk test. Semiquantitative questions (Likert scale) linked to the satisfaction with the lip’s anatomy were evaluated for consistency using the Cronbach’s alpha test. The authors prepared a score based on the four questions related to the satisfaction with the shape of the lips.
The initial sample size was determined based on a paired Student’s-t test with a 80% strength and 0.05 alpha error for detection of a mean difference similar to the standard deviation of the quantitative measurements.
Values of two-tailed p <0.05 were deemed significant.
The study was duly approved by the Research Ethics Committee of the Institution and registered under the number 34745714.9.0000.0100. The authors funded expenses incurred with the study, with absence of conflicts of interest.
A total of 19 female patients were evaluated (mean age = 47 years, SD =12.1). The mean value for the total dose of toxin units applied was 43U (SD = 3,4), with the amount injected in the lips being always the same – 0.5U per point – in the four points.
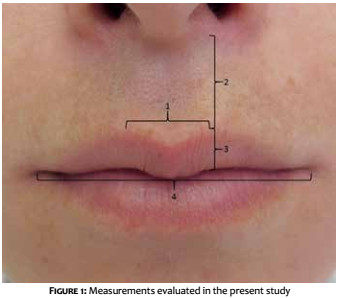
The lip’s measurements were taken according to the segments seen in Figure 1.
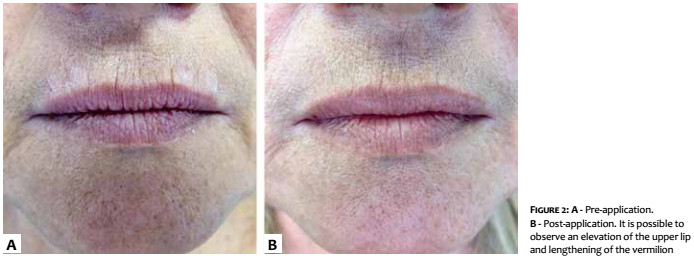
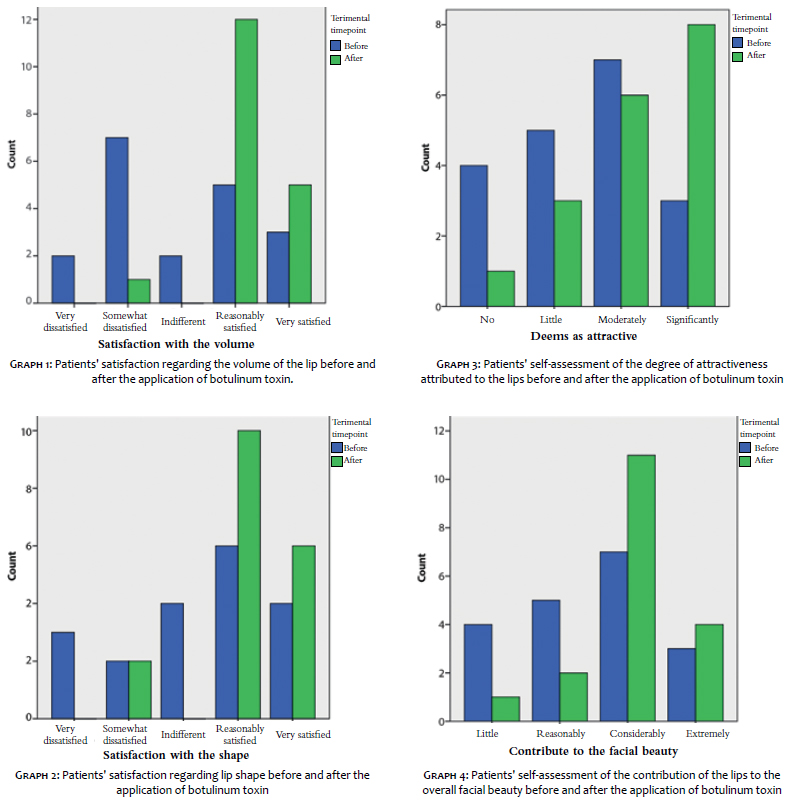
It was possible to note a statistically significant (p = 0.002) increase in Segment 3, in the post-procedure evaluation. Similarly, the vermilion/philtrum ratio (Segment 4 / Segment 2) was also greater after the procedure (p = 0.001). Most of the patients (n = 10) were dissatisfied with or indifferent to their lip’s volume previously to the procedure, with 17 saying they were satisfied or very satisfied after the application of toxin (p = 0.003) (Figure 2).
The same was true for the evaluation of the lip’s shape, where 16 patients said they were reasonably or very satisfied after the procedure (p = 0.048), as shown in the graphs below (Graphs 1 to 4).
Most patients deemed their lips as moderately or significantly more attractive after the treatment with toxin (p = 0.039), and 15 women perceived the change in their lips as a major contributor to the overall improvement of their faces. The perception of volumization was present in in all except for 1 patient.
Regarding side effects, no patient had difficulty to speak, 2 had some difficulty to eat in the first two weeks, and 4 had difficulty to smile. The patients were followed up, and after 30 days none of them sustained their complaints.
In this manner, it was possible to calculate the overall satisfaction score regarding the lips’ appearance, taking into consideration their volume, shape, attraction and contribution for the overall improvement of face appearance, being this positive (p = 0.005).
Of the 19 initially included patients, 17 (89.5%) would undergo application of toxin again.
The use of botulinum toxin type A is a well-known procedure for the improvement of rhytids in the upper third of the face. Regarding the lower third of the face, despite the high frequency with which the procedure is performed, there are very few studies on the toxin’s effects on the labial region. The technique has become increasingly popular, partly due to the doctors’ confidence in the excellent efficacy and safety profile demonstrated by the botulinum toxin since 1987 in topical indications. In addition, physicians realized that muscle hyperactivity and volume depletion were important concomitant aesthetic determinants for the middle and lower face.
It is important to bear in mind that muscle anatomy and tissular relationships are very different from those found in the upper face, meaning that the doses used are smaller, and the application points must be selected more carefully in order to avoid undesirable effects.
As for the perioral region, the authors noticed that the lips are key points for the aesthetic appearance of the face. With the aging process, the lateral portions of the lips tend to become less visible and the distance between the columella and the upper lip’s vermilion increases, resulting in the appearance of thin lips. This process becomes even more visible in smokers, nonetheless hereditary factors may often be relevant.
As discussed by Carruthers & Carruthers,7 small doses of botulinum toxin can lead to localized microparesis of the orbicularis muscle, dramatically reducing the visibility of perioral lines.
However, in order to maintain the mouth’s functional competence, it is important to take a conservative approach regarding the dosage and superficial injections. The authors in question (the Carruthers) obtained satisfactory results with doses of 2 to 4U botulinum toxin per lip (without using more than 2U per lip quadrant). Due to the fact that the authors of the present article used a toxin with a higher diffusion index (Dysport), a decision was made for an even more conservative stance regarding the doses, which also yielded very satisfactory results.
The literature further emphasizes that the corners of the lips should be avoided due to the fact that injection in these sites cause undesirable weakness of the lip lift muscles, entailing difficulty to eat, whistle, and even leading to a propensity to drool. The midline is also preserved, avoiding the flattening of the cupid’s bow – which has driven the authors of the present study’s decision for applying the toxin in four points only.
Foster and Wulc 8 also described a technique for the use of botulinum toxin for perioral lines that is very similar to the one used in the present study for choosing the site of application. The patient is asked to pucker her or his lip – as in the kissing motion – so that the areas of muscular contraction adjacent to the lines become visible, facilitating the visualization and execution of the technique.
There was a change in the vertical measurements of the upper vermilion and the philtrum, with an increase in the first and a reduction in the second. In the present study, the patients had an elevation of the upper lip, which led to a shortening of the philtrum and lengthening of the vermilion. The authors believe that by applying the toxin in the vermilion’s border, it is possible to obtain relaxation of the orbicularis muscle, allowing a greater tonus in the upper lip lift muscles.
The patients’ satisfaction with their lips’ appearance was positive – mainly regarding volume – and considered attractive, as assessed by the combined answers to the four questions (shape, volume, attraction and contribution to overall appearance).
The side effects were rare and mild, arising mainly as difficulty to speak and/or smile. Notwithstanding, 89% of the patients would undergo re-application of the toxin.
In this manner, botulinum toxin was proven as an important ally in the treatment of the lips region, and should be deemed as a promising method for improving the general appearance of the face in combination with other well-established treatments for this purpose.
1. Carruthers A, Carruthers J. History of the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24(11):1168-70.
2. Carruthers A, Carruthers J. Clinical indications and injection technique for the cosmetic use of botulinum A exotoxin. Dermatol Surg. 1998;24(11):1189-94.
3. Loyo M, Kontis TC. Cosmetic botulinum toxin: has it replaced more invasive facial procedures. Facial Plast Surg Clin North Am. 2013;21(2):285-98.
4. Cavallini M, Cirillo P, Fundarò SP, Quartucci S, Sciuto C, Sito G, Tonini D, Trocchi G, Signorini M. Safety of botulinum toxin A in aesthetic treatments: a systematic review of clinical studies. Dermatol Surg. 2014;40(5):525-36.
5. Carruthers A, Carruthers J, Monheit GD, Davis PG, Tardie G. Multicenter, randomized, parallel-group study of the safety and effectiveness of onabotulinumtoxin A and hyaluronic acid dermal fillers (24-mg/ml smooth, cohesive gel) alone and in combination for lower facial rejuvenation. Dermatol Surg. 2010;36 Suppl 4:2121-34.
6. Gordon RW. BOTOX cosmetic for lip and perioral enhancement. Dent Today 2009 May;28(5):94-7.
7. Carruthers J, Carruthers A. Aesthetic botulinum A toxin in the mid and lower face and neck. Dermatol Surg. 2003;29(5):468-476.
8. Foster JA, Wulc AE. Cosmetic use of botulinum toxin. Facial Plast Surg Clin North Am. 1998;6:79-85.
This study was carried out at the Dermatology Service, Dermatology Service, Hospital Universitário Evangélico de Curitiba - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}