


Vando Barbosa de Sousa1; Vanessa de Carvalho Lacerda1; Marcella Leal Novello D'Elia2; Natália Ribeiro de Magalhães Alves3; Juãn Manuel Piñeiro-Maceira4; Solange Cardoso Maciel Costa Silva5
Nodular hidradenoma is a benign adnexal neoplasia. Recently a subdivision in two groups has been suggested: tumors with eccrine differentiation or poroid hidradenoma and tumors with apocrine differentiation or clear cell hidradenoma. They present as well delimited dermal nodule, with a variable dimension between 0.5 and 3 cm, asymptomatic, slow growing and endophytic. Histopathology shows typical biphasic cell pattern, with polyhedral cells with eosinophilic cytoplasm and large cells with abundant clear cytoplasm and small nucleus. Malignant transformation is rare. We report a case of clear cell hidradenoma with unusual clinical characteristics and a review of the literature.
Keywords: NEOPLASMS, ADNEXAL AND SKIN APPENDAGE; SKIN NEOPLASMS; ACROSPIROMA; SURGICAL FLAPS
Initially described by Mayer1 in 1941, nodular hidradenoma is a benign adnexal neoplasm, of eccrine or apocrine differentiation. Due to different interpretations of its histological characteristics, several denominations and classifications have been suggested throughout the years, thus causing controversies. More recently a sub-division into two subgroups has been suggested: tumors with eccrine or poroid hidradenoma differentiation and tumors with apocrine or hidradenoma differentiation of clear cells.2 It is found in middle-aged adults, being more prevalent in women. Clinically, it manifests as a solid or cystic, well-delineated nodule, with a variable diameter of 0.5 to 3cm, asymptomatic, of slow growth and endophytic. The most commonly affected places are the scalp, the face, the chest and the proximal extremities.3 Cases of clear cell hidradenoma in the scalp with uncommon clinical characteristics have been reported.
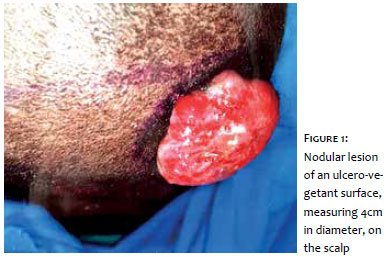
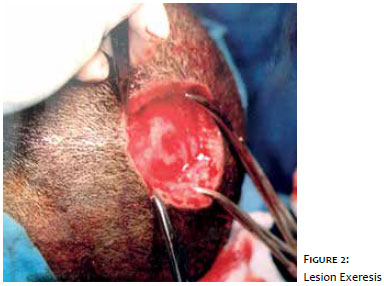
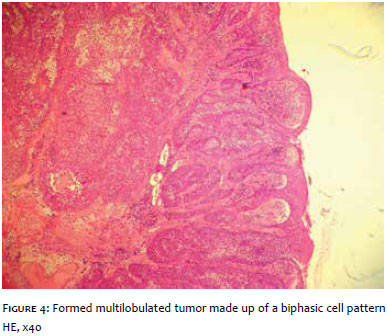
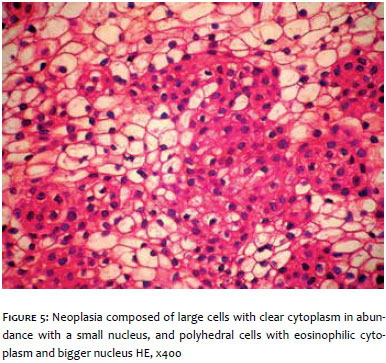
A 32-year-old male, first reported the development of an ulcero-vegetant nodular lesion on the surface of the scalp a year and a half ago, with progressive growth, reaching 4cm in diameter (Figure 1). Drainage of serous discharge was also reported. He denies comorbidities, uses medication, presents allergies, and has family or personal history with skin diseases. Skull CT scan has shown an expansive formation with soft tissues density, heterogeneous contrast enhancement, in topography adjacent to the occipital bone, thus causing the skin surface to bulge, with bone cortical intact. It has been theorized that epidermoid carcinoma, basal cell carcinoma, cutaneous metastasis, cutaneous lymphoma and amelanotic melanoma. Lesion excision was performed with a 5mm margin and closed with an O-to-Z double rotation flap (Figures 2 and 3). Histological examination has shown multilobulated, well circumscribed tumor, constituted by a biphasic cell pattern, with polyhedral cells of eosinophilic cytoplasm and cells with clear cytoplasm in abundance, as well as cystic spaces (Figures 4 and 5). The final diagnosis was clear cell hidradenoma.
The nodular hidradenoma, described in 1941 by Mayer,1 is a benign adnexal neoplasm, which is not clearly identified in the medical literature. Some authors consider it is a rare entity,2 others mention it as being relatively common.4, 5 There is considerable confusion in the literature regarding the appropriate designation, and it has already been called nodular hidradenoma, clear cell hidradenoma, cystic nodule hidradenoma, clear cell myoepithelioma, and eccrine acrospiroma. This reflects different approaches among authors regarding its histological characteristics and histogenesis.4 Even though it is traditionally classified as an eccrine differentiation, the idea that these tumors may show eccrine or apocrine differentiation is now accepted.6 More recently, a subclassification into two different groups has been suggested: tumors with eccrine differentiation or poroid hidradenoma, and tumors with apocrine differentiation or clear cell hidradenoma.2 Some authors, however, classify the poroid hidradenoma separately from the nodular hidradenoma.4
Present mainly in middle-aged adults, it is more commonly found in women. It is arises as a well-delineated, solid or cystic skin nodule, with a dimension varying between 0.5 and 3cm, on the scalp, face, chest and proximal extremities. In general, it is asymptomatic, rarely includes pain and drainage of serous discharge. The growth is slow and endophytic, but there are rare cases in which the growth is exophytic.3 Traditionally, the differential diagnosis includes other adnexal tumors, being clinically indistinguishable. Uncommon appearances include tumors with more than 3cm in diameter,7 tumors with eroded surface, tumors with predominant cystic component and in uncommon places, such as the plantar region.8
The histopathology of the clear cell hidradenoma is characterized by the presence of a well circumscribed, but not encapsulated, tumor. Two cell types are predominant: polyhedral cells with eosinophilic cytoplasm, and large cells with clear cytoplasm in abundance with a small nucleus. Cystic spaces are common, as a result of tumor cell degeneration. Apocrine secretion due to decapitation can be observed. Some tumors may present squamous, sebaceous or mucinous epithelial differentiation.2 There is a variable proportion among cell types, but the clear cells predominate in one-third of the cases.3
The case that was reported presents the typical histopathology of the clear cell hidradenoma, thus showing an uncommon clinical presentation, given the dimensions of the tumor and its exophytic growth with eroded surface. The surgery is curative, but reoccurrence may happen even in the case of incomplete excision.9 A malignant transformation is very rare, being that most hidradenocarcinoma recurr.10
1. Mayer I. Zur histologie der hidroadenome. Frankfurter Zeit f Pathol. 1941;55:548-80.
2. Nandeesh BN, Rajalakshmi T. A study of histopathologic spectrum of nodular hidradenoma. Am J Dermatopathol. 2012;34(5):461-70.
3. Winkelmann R, Wolff K. Solid - cystic hidradenoma of the skin. Arch Dermatol. 1968;97(6):651-61.
4. Kazakov DV, McKee PH, Michal M, Kacerovska D. Lesions with Predominant Apocrine and Eccrine Differentiation. In: Dmitry V. Kazakov MD PhD, Cutaneous adnexal tumors. Wolters Kluwer Health: 2012. p1-171.
5. Hernandez-Perez E, Cestoni-Parducci R. Nodular hidradenoma and hidradenocarcinoma. A 10-year review. J Am Acad Dermatol. 1985;12(1 pt 1):15-20.
6. Gianotti F, Alessi E. Clear cell hidradenoma associated with the folliculosebaceous apocrine unit. Histologic study of five cases. Am J Dermatopathol 1997;19(4):351-7.
7. Demirci GT, Atis G, Altunay IK, Sakiz D. A giant benign clear cell hidradenoma on the anterior trunk. Dermatol Reports. 2011;3(3):e45.
8. Shin HT, Clear cell hidradenoma on the palm. Ann Dermatol. 2014;26(3):403-4.
9. Will R, Coldiron B. Recurrent clear cell hidradenoma of the foot. Dermatol Surg. 2000;2697):685-6.
10. Yildrim S, Akoz T, Apaydin I, Ege G, Gideroglu K. Malignant clear cell hidradenoma with giant metastasis to the axilla. Ann Plast Surg. 2000;45(1):102.
This study was performed at the Hospital Universitário Pedro Ernesto, Universidade do Estado do Rio de Janeiro (Hupe/Uerj) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}