


Caroline Silva Pereira1; Erica Bruder Botero2; Gabriela Cristina Nascimento dos Reis3; Fernanda Sayuri Ota4
Basal cell carcinoma corresponds to the majority of malignant cutaneous malignancies in Brazil, predominating in middle-aged white individuals, mainly affecting the upper two-thirds of the face and occurring due to several etiological factors. The ideal treatment consists of complete removal with free lesion margins. For better functional and aesthetic results, reconstruction of the surgical wound with flaps or grafts may be necessary. Two types of reconstruction are described in patients with double surgical defects on the face, close to each other: one with a single rotation flap and another with a double rotation flap, also called Yin-Yang.
Keywords: SKIN NEOPLASMS; CARCINOMA, BASAL CELL; SURGICAL FLAPS
Basal Cell Carcinoma (BCC) accounts for 70% of [all] malignant skin neoplasms in Brazil, mainly affecting middle-aged white individuals.1 BCC preferably affects the upper two thirds of the face (60 [to] 80%), and its main etiology is attributed to exposure to ultraviolet radiation. Other risk factors were taken into account, to be inclusive of personal and family history of skin cancer, immunosuppression, exposure to fluorescent radiation, smoking, radiotherapy, PUVA Therapy and exposure to arsenic, coal tar and organophosphorus compounds.1 Despite its low mortality rate (0.05% to 0.08%), once the diagnosis of the lesion has been defined by anatomopathological examination, appropriate treatment must be established, because recurrent BCC or late treatment thereof presents high rates of therapeutic failure. The ideal treatment consists in a complete removal of the lesion with free margins. For a better functional and aesthetic result, the reconstruction of the surgical wound or grafts may be needed. There are two types of reconstruction, which are recommended for patients with surgical defects that are bilateral or close to each other. resulting from the removal of BCCs. A simple rotation flap was used on the first patient and a dual rotation flap, also known as "yin-yang rotation flap" was used on the second patient.
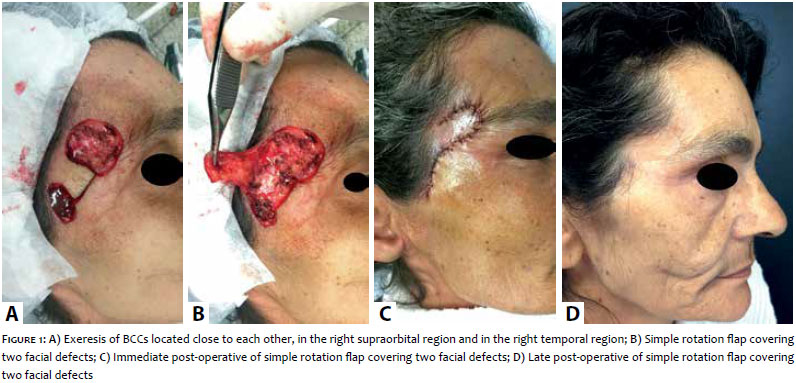
A 53-year-old female patient, Phototype III, originally from Impirá, Bahia (NE of Brazil), with positive personal history of skin cancer. The dermatological examination indicated the presence of two asymptomatic lesions for two years, one measuring 3cm on the right supraorbital region, and another measuring 1cm on the right temporal region. During the dermoscopy, it was possible to observe absence of pigmentary network, ulcerations, maple leaf-like lesions and arboriform telangiectasias. Incisional biopsy was performed in the lesions, confirming BCCs via the anatomopathological study. The exeresis was designed to have 4mm margins, marked by dermoscopy (Figure 1A). For the closure, a simple rotation flap was performed, with the secondary defect being approximated by primary suture (Figure 1B). The patient showed good progression during the immediate (Figure 1C) and late post-operative (Figure 1D). The anatomopathological exam for both lesions confirmed the free margins.
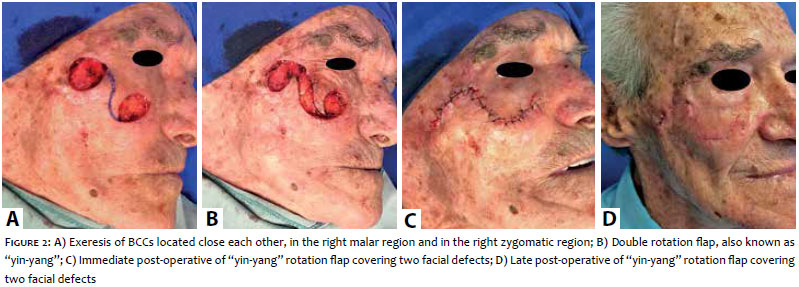
An 85-year-old male patient, Phototype II, originally from Campinas, São Paulo (SE of Brazil), with a current personal history of skin cancer. During the dermatological examination, two asymptomatic lesions (with onset three years before) were observed, one measuring 1cm on the right malar region, and another measuring 0.8cm on the right zygomatic region. During the dermoscopy of both lesions, arboriform telangiectasias, ovoid nests and white amorphous areas were evidenced. Incisional biopsy was performed in the lesions, confirming BCCs via the anatomopathological study. Both lesions were removed during the same surgery, with 4mm margins, after pre-operative marking by dermoscopy (Figure 2A). During the procedure, the defects were closed using the healthy skin in between them, with two rotation flaps, thus constituting a double rotation flap, whose is similar in shape to the Chinese "yin-yang" symbol (Figure 2B). The patient showed good progression during the immediate (Figure 1C) and late post-operative (Figure 1D). Following the exeresis, the anatomopathological exam for both lesions confirmed free margins.
The proximity of both surgical defects offers a reconstructive challenge, mainly due to the primary closure.2, 3 Therefore, in cases like these, a decision is made to use skin flaps or grafts is many times made aiming at achieving better aesthetic and functional outcomes.4 Grafts are skin fragments removed from donor areas and transferred to the surgical wound, from whence new blood supply is obtained. They may be classified according to 1) their composition, as: full-thickness, split-thickness or composite skin graft; 2) the genetic origin of the graft's tissue: as autologous, allogeneic, isogeneic, and xenogeneic; 3) its shape, as: stamp skin graft, mesh skin graft or chip skin graft. The most common complications in the use of grafts are the hematomas. Flaps are skin and subcutaneous segments with their own vascular bed, adjacent to the surgical wound, and used to fill it when primary closure of the edges is not possible. The donor region should contain excess skin with enough mobility to reach the receiver area without excessive traction or vascular distress to the pedicle. They are classified under several criteria: advancement, rotation or transposition (regarding the main movement); arterial or random (depending on blood supply to the flap); and rhomboid (Limberg), bilobed and others (regarding the shape). The most common complications are necrosis and infection.5, 6 Reconstruction of nearby surgical defects on the face varies significantly depending on the location and distensibility of adjacent tissue.3, 7 The defects of the aforementioned surgical cases were reconstructed by simple and dual rotation flaps, used to repair large tissue losses or entire aesthetic units. The movement of the flap for the surgical defect was basically that of rotation, creating, thus, a secondary defect adjacent to the first, as demonstrated in Case 1, which was approximated by a primary suture. As for the double skin flap (Case 2), also known as "yin-yang", a curved line is drawn by joining the lower portion of the first defect to the upper portion of the second, creating a figure similar to that of the Chinese "yin-yang" symbol, followed by a double rotation.8 It was necessary to remove two small compensation triangles, superior to the medial defect and inferior to the lateral defect.9
The dual "yin-yang" rotation flap has already been used for the closure of major face defects, in combination with the Mustardé flap, leading to excellent results in a series of nine cases.10 It has also been applied for surgical closure in the sacral region, by using two trapeze-shaped flaps with a subcutaneous pedicle.
In both surgical cases aforementioned, the execution of skin flaps progressed without any complications, both with favorable aesthetic and functional outcomes.
Flaps are preferably used due to preservation of skin color, texture and thickness, in addition to the facts that they avoid the formation of a secondary surgical wound, which emerges when a graft is harvested. Several techniques are described for the closures of facial defects nevertheless, there are few that focus on the simultaneous closure of wounds located close to each other. The proximity of two defects means a surgical challenge in the management of the lesion's closure, bearing in mind that the aesthetic and functional outcomes are of paramount importance.
1. Chinem VP, Miot HA. Epidemiology of basal cell carcinoma. An Bras Dermatol. 2011;86(2):292-305.
2. Mureau MAM, Hofer SOP. Maximizing results in reconstruction of cheek defects. Clin Plastic Surg. 2009;36(3):461-76.
3. Comparin C, Filho GH, Freitas CAF. Reconstrução complexa de hemiface direita: o desafio de dois carcinomas basocelulares. XXVI Cong Brasileiro de Cirurgia Dermatológica - Porto Alegre, 2014.
4. Bernstein G, Senkarik M. Surgical Anatomy of the skin. Connecticut: Appleton & Lange; 1988. p.217-22.
5. Baker SR. Retalhos locais em reconstrução facial. Rio de Janeiro: Di Livros; 2009. p.585-603.
6. Kopke LFF. Retalhos. In: Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de Cirurgia Dermatológica, Cosmiatria e Laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Elsevier; 2012. 56:724-9.
7. Dobratz EJ, Hilger PA. Cheek defects. Facial Plast Surg Clin North Am. 2009;17(3):455-67.
8. Behan FC, Rozen WM, Tan S. Yin-Yang flaps: the mathematics of two Keys toneis land flaps for reconstructing increasingly large defects. ANZ J Surg. 2011;81(7-8):574-5.
9. Boggio P, Gattoni M, Zanetta R, Leigheb G. Burow's triangle advancement flaps for excision of two closely approximated skin lesions. Dermatol Surg. 1999;25(8):622-5.
10. Belmahi A, Oufkir A, Bron T, Ouezzani S. Reconstruction of cheek skin defects by the 'Yin-Yang' rotation of the Mustarde´ flap and the temporo parietal scalp. J Plast Reconstr Aesthet Surg. 2009;62(4):506-9.
This study was performed at the Dermatology Service of the Pontifícia Universidade Católica de Campinas (PUC-Camp) - Campinas (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}