


Cândida Naira Lima e Lima Santana1; Daniele do Nascimento Pereira1; Jaqueline Barbeito de Vasconcellos1; Vanessa de Carvalho Lacerda1; Barbara Nader Vasconcelos2
Acne scars present at the end of the inflammatory phase of acne vulgaris have been treated with procedures that stimulate the production of collagen, such as microneedling. Six patients with acne scars were selected. Microneedling was performed with 2.5 mm needles. Subjective improvement was observed in all patients. In the technique of percutaneous collagen induction there is release of cytokines, growth factors and angiogenesis, with final production of type I collagen, making microneedling an excellent option for the treatment of acne scars, both for its cost/ benefit and for not drawing patients away from their daily activities.
Keywords: ACNE VULGARIS; CICATRIX; TREATMENT OUTCOME
Acne vulgaris is one of the most common skin diseases. After the end of the active inflammatory phase, most patients have atrophic scars.1 Studies have confirmed its psychosocial impact demonstrating a higher incidence of disorders such as introverted personality and depression in patients with severe acne scars,2 and thus an aesthetic and psychological problem. Ablative procedures aimed at stimulating and remodeling collagen have long been advocated in Dermatology. Currently, there is a trend towards less invasive procedures, aiming at reducing complications and promoting the patient's rapid return to daily activities. Microneedling has been described as a practically painless, simple and minimally invasive technology.3 It is a good option in this context and it is based on the stimulation of collagen production, without causing total de-epithelialization, which is observed in some ablative techniques.
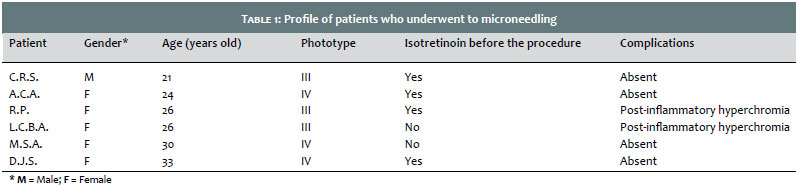
The procedure was performed in six patients (five females and one males). Their ages ranged from 21 to 33 years old, with an average of 26.6 years old. The phototype (Fitzpatrick's classification) in four patients was IV, and in two was III (Table 1). Four of the six patients took isotretinoin orally before the procedure, with a target dose between 120 and 150mg/kg. They underwent microneedling at least six months after the end of the medication. None of the patients presented comorbidities or used any systemic medication. At the physical examination, they presented distensible and non-distensible acne scars distributed mainly in the malar and temporal regions, including some icepick scars. There were no inflammatory lesions at the time of the procedure.
Initially, the areas with the highest concentration of scars were demarcated for the procedure. The patients were then submitted to tumescent anesthesia (2% lidocaine 20mL, 20mL distilled water, 0.4mL 1mg/mL adrenaline, 4mL 8.4% sodium bicarbonate). A device with 2.5mm needles was used in multidirectional movements until Auspitz signs were observed. The occlusive dressing was carried out with a combination of clobetasol and neomycin, with an initial change after 24 hours (Figure 1). Reassessments were performed after seven, 30 and 60 days.
All patients reported subjective improvement of the lesions, which was also observed by the medical team. On a visual scale of 1 to 10 (1 being completely dissatisfied and 10 being completely satisfied), all patients were graded above 5. The best outcome was observed for distensible scars, with little difference in the aspect of the ice-pick scars (Figure 2). None of the patients developed infectious intercurrences. The only complication was post-inflammatory hyperchromia, which affected two patients (Table 1). Whitening creams in combination with hydroquinone, corticoid and retinoic acid were used, yielding progressive improvement.
Acne scars can result from increased tissue proliferation or tissue loss. Atrophic scars are usually caused by loss of collagen after acne inflammatory process. They can be classified as icepick, rolling and boxcar acne scars. There is no standard therapy.4 There are a range of options, such as peelings, punch techniques, subcision, dermabrasion, cutaneous fillers,4 that have a low rate of success; and ablative lasers, with a high success rate, however at a high cost and demanding a longer recovery time.
In this context, microneedling emerges as a cost effective technique, with a good response while not demanding patients to keep away from their daily activities. It is a safe procedure that can be performed at the practice without complications.5
The Dermaroller device is a cylinder with 192 microneedles (ranging from 0.25 to 3mm in length and with diameters of 0.1mm) that is used only once. It must be firmly pressed and rolled against the skin.2, 6 The needles penetrate the stratum corneum and create microducts that reach the dermis, causing minimal damage to the epidermis, which recovers rapidly.5, 6
The procedure can be performed with topical anesthesia applied about 45 minutes before, and the Dermaroller should be rolled 15 to 20 times horizontally, vertically and obliquely, under an average vertical pressure estimated around 6N.7 By applying the device 15 times in the area, approximately 250 holes/cm2 will be inflicted. The bleeding that occurs is easily controlled. Three or four sessions are required, with intervals ranging from two to six weeks.6 Erythema may occur for up to two days.2 The most evident results begin to be observed at between four and six weeks, nevertheless the deposition new collagen is slow and the skin's texture may keep on improving over the 12 following months.8
This technique works by trying to create multiple small lesions in the papillary dermis, triggering a cascade of growth factors and cytokine release – mainly Interleukin 1α, 8 and 6, tumor necrosis factor α, and granulocytes and macrophages colony stimulation factor – resulting in dermal vasodilation, migration of keratinocytes, neocollagenesis, and neoangiogenesis.9
Three phases of the healing process, following the trauma with the needles, can be delineated. During the first one (injury phase), there is the release of platelets and neutrophils responsible for the release of growth factors acting on keratinocytes and fibroblasts, such as the growth and transformation factors α and β (TGF-α and TGF-β), the platelet derived growth factor, connective tissue-activating protein III (CTAP-III), and connective tissue growth factor.7 In the second phase (healing phase), neutrophils are replaced by monocytes, and angiogenesis, epithelization and fibroblast proliferation occur, followed by the production of type III collagen, elastin, glycosaminoglycans and proteoglycans. At the same time, the fibroblast growth factor, TGF-α and TGF-β are secreted by monocytes. Approximately five days after the injury has been inflicted, the fibronectin matrix is formed, thus allowing the deposition of collagen just below the basal layer of the epidermis. In the third phase (maturation phase), type III collagen, which is predominant in the early stage of the healing process, is slowly replaced by type I collagen – which is more durable, lasting for a period ranging from five to seven years.7 Microneedling also has the advantage of combining the transdermal delivery of selected drugs, thus optimizing the desired results.3, 5 Chawla et al. carried out a microneedling study with platelet-rich plasma (PRP) and vitamin C, with superiority of PRP. Fabbrocini et al. also combined PRP with microneedling with a good response.8
Garg and Baveja carried out a study that combined the use of subcision, Dermaroller and 15% TCA peel, with the use of topical tretinoin, which led to good results even in acne scars Grades 3 and 4.4 It is also possible to perform the delivery of energy into the dermis with the association of radiofrequency, which leads to good results when treating scars, hyperhidrosis and rhytides.10
Microneedling is becoming an excellent option for the treatment of acne scars, with overall improvement of the skin's texture and attenuation of the atrophic scars, presenting good clinical outcomes, without any serious complication after the procedure, in addition to the patient's personal satisfaction.
1. Liebl H, Kloth LC. Skin cell proliferation stimulated by microneedles. J Am Coll Wound Spec. 2012;4(1):2-6.
2. Majid I. Microneeddling therapy in atrophic facial scars: an objective assessment. J Cutan Aesthet Surg. 2009;21(1):26-30.
3. Kalil CLPV, Frainer RH, Dexheimer LS, Tonoli RE, Boff AL. Estudo comparativo, randomizado e duplo-cego do microagulhamento associado ao drug delivery para rejuvenescimento da pele da região anterior do tórax. Surg Cosmet Dermatol. 2015;7(3):211-6.
4. Garg S, Baveja S. Combination Therapy in the Management of Atrophic Acne Scars. Journal of Cutaneous and Aesthetic Surgery. 2014; 7(1):18-23.
5. Chawla S. Split face comparative study of microneedling with PRP versus microneedling with vitamin C in treating atrophic post acne scars. J Cutan Aesthet Surg. 2014;7:209-12.
6. El-Domyati M, Barakat M, Awad S, Medhat W, El-Fakahan H, Farag H. Microneedling Therapy for Atrophic Acne Scars - An Objective Evaluation. J Clin Aesthet Dermatol. 2015;8(7):36-42.
7. Lima, EVA, Lima, MA, Takano, D. Microagulhamento: estudo experimental e classificação da injúria provocada. Surg Cosmet Dermatol. 2013;5(2):110-4.
8. Fabbrocini G, Annunziata MC, D´Arco V, De Vita V, et al. Acne Scars: pathogenesis, classification and treatment. Dermatol Res Pract. 2010; 2010:893080.
9. Bal SM, Caussian J, Pavel S, Bouwstra J A. In vivo assessment of safety of microneedle arrays in human skin. Eur J Pharm Sci. 2008;35(3):193-202.
10. Kim ST, Lee KH, Sim HJ, Suh KS, Jang MS. Treatment of acne vulgaris with fractional radiofrequency microneedling. J Dermatol. 2014;41(7): 586-91.
This study was performed at the Universidade do Estado do Rio de Janeiro (Uerj) – Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}