


Thaís Martins Tonso1; Caroline Romanelli2; Ana Laura Rosifini Alves Rezende3; Cínthia Mendes4; Ana Helena Kalies Oliveira4
Alopecia areata is a relatively common autoimmune condition. It has an unpredictable course and its etiology has not yet been fully elucidated. Its treatment must be individualized, and aims at suppressing the phase of activity of the disease. Thus, many alternatives are available; however, none of them have been curative or preventive so far. We report the cases of two patients, aged 18 and 43 years, diagnosed with alopecia areata, who underwent topical immunotherapy with diphencyprone, and obtained different results. The application procedures, the results obtained and the clinical follow-up are described.
Keywords: THERAPEUTICS; IMMUNOTHERAPY; ALOPECIA AREATA; AUTOIMMUNE DISEASES
Alopecia Areata (AA) is a systemic, autoimmune condition characterized by loss of hair, without any association with scarring or inflammatory processes.1 Its course is unpredictable, and the response to treatments is extremely variable.
The worldwide prevalence of AA ranges from 0.1% to 0.2%; 85.5% of cases occur in patients aged up to 40 years. The incidence is equal in both genders; extensive cases, however, are predominant in men.1, 2 Its etiology remains uncertain; it is known that it is influenced by genetics, autoimmune and environmental factors.
The influence of genetic factors is evident when the incidence in first-degree relatives, the concordance between monozygotic twins, and the genetic linkage analysis are observed. Madani et al. have demonstrated that AA is a polygenic disease of incomplete penetrance.3 The association of human leukocyte antigens (HLA) with susceptibility to AA (HLA-DRB1 *0401 and DQB1 *0301) has also been noted.4
The autoimmune character of the condition is strengthened by the concomitance of AA with other autoimmune disorders and by the therapeutic response to immunosuppressants. Studies have shown that environmental factors can trigger autoimmune aggression; Among them, emotional or physical stress, infections and hormone activity.4 The corticotrophin releasing hormone and the α-Melanocyte-stimulating hormone stand out; both have increased expression in individuals with AA.1
In summary, genetically predisposed individuals, when exposed to environmental factors, develop autoimmune disorders with T-lymphocyte-mediated inflammation against the capillary bulb, generating dysregulation in the follicular cycle.
The diagnosis of this entity is clinical; trichoscopy and anatomopathological examination may help. During the trichoscopy it is possible to find black dots, yellow dots and exclamation mark hairs. In the anatomopathological examination, in the acute phase, there is lymphocytic infiltrate (CD4+ T and CD8+ T) peribulbar in anagen hairs, with a "swarm of bees" aspect. During activity, the CD4 / CD8 ratio is increased and is responsible for maintaining the follicles in the dystrophic state in the anagen phase, leading them into early telogen phase.1 In the subacute phase, a large number of hairs in the catagen and telogen phases are found, and in the chronic phase the miniaturization of the follicles can be observed. The treatment for AA is aimed at suppressing the activity phase. The options are numerous, although no therapy has proven to be curative or preventative.3
Two AA patients with more than 50% of the scalp area compromised, were treated at the Trichology Outpatient Clinic of the Dermatology Service at Celso Piero Hospital, Pontifícia Universidade Católica de Campinas (PUC-Campinas), between December 2012 and June 2015.
Patient 1: 43-year-old female, Caucasian, previously diagnosed with anxiety disorder. She reported progressive hair loss over the previous two years, and denied having undergone any previous treatment.
Patient 2: 18-year-old female, brown-skinned, student; during the first visit, reported progressive capillary loss for one year, and previous use of topical minoxidil, without clear signs of improvement.
After clinical diagnosis, photographic documentation of the lesions and advice regarding the character of the condition and its possible treatment paths, both of them underwent topical diphencyprone (DPCP) immunotherapy.
The authors used DPCP in acetone vehicle, stored in an amber bottle. Available concentrations are: 0.001%, 0.025%, 0.05%, 0.1%, and 2%; the drug was obtained in a compounding pharmacy in the aforementioned dilutions (Figure 1).
The applications were performed on the scalp, with swab soaked in the solution (Figure 2). In all sessions, the patients were instructed to avoid exposure to the sun and keep the substance in place, without contact with water for 48 hours. After this period, it was recommended they removed it under running water.
The first application (sensitization) was performed with 2% DPCP, in a 2cm diameter area.5 After two weeks, adequate response was observed (mild erythema and mild pruritus in the treated area, 36 hours after the application), and weekly applications ipsilateral to the sensitized side begun with 0.001% DPCP. The concentration of the substance was gradually increased during each application (0.001%, 0.025%, 0.05%, 0.1%) up until the patient had a more intense response than the one defined as adequate; at this point, the concentration was established for each of the patients, and the treatment continued with weekly applications.
After the appearance of re-epilation on the side initially treated, bilateral treatment was started.
Patients presented onset of re-epilation after two months of treatment, with an cosmetically acceptable appearance after nine months. Both patients tolerated a maximum concentration of 0.05% and had no side effects.
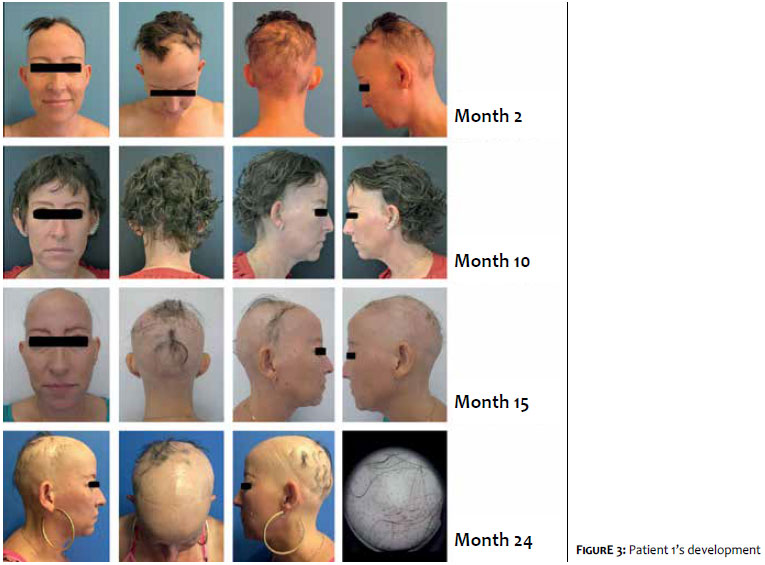
An excellent response was reached in both cases, however Patient 1, after 11 months of treatment, with almost complete re-epilation, abandoned the follow-up for two months. During that period, she abruptly stopped DPCP applications.
Upon her return, she presented again diffuse capillary loss, and DPCP applications were restarted. However, given the inefficacy of the treatment, other drugs were combined: intralesional 5mg/ml methylprednisolone acetate, 1mg/kg/day prednisone for 60 days and 15mg/week methotrexate for 120 days. Despite these measures, the patient still coursed with progressive capillary loss (Figure 3).
Patient 2 attended regular follow-up sessions without complications. She presented complete re-epilation, and is in a slow and gradual process of drug withdrawal (Figure 4).
Alopecia areata is a relatively common condition. It does not pose a threat to life, but it causes psychological stress and impacts on the quality of life.1
Its treatment is determined by the patient's age and the condition's degree of involvement.6 For those over ten years of age, with an area greater than or equal to 50% of the scalp compromised, the first option is topical immunotherapy,7 whose mechanism of action is not elucidated. It is known that the application of a primary sensitizer causes dermatitis, with consequent deviation of the perifollicular lymphocytes involved in the pathogenesis of AA to the epidermis. This results in the alteration of the perifollicular relationship between CD4+ / CD8+ lymphocytes, causing apoptosis of autoreactive T-lymphocytes, and the modulation of proinflammatory cytokines.8 There are three primary sensitizers described: dinitrochlorobenzene (DNCB), squaric acid dibutyl ester (SADBE) and diphencyprone (DPCP), the current choice. DNCB is proscribed due to its mutagenic potential, and SADBE, being unstable in acetone, is reserved for patients not responsive to DPCP sensitization.³
The use of DPCP in the treatment of AA was described in 1983 by Happle et al.9 and several studies have proven its efficacy. The most commonly reported side effects are pruritus, moderate local eczema, regional lymphadenopathy, and contact urticaria. Rarely observed are, erythema multiforme, dyschromia and vitiligo.5, 8, 10
Response to therapy may occur up to two years after starting the treatment; 59% of patients respond within the first six months, 26% between six months and one year, 10% between one and two years, and 5% after two years.10 It is, therefore, recommended that treatment not be discontinued before two years.
Data regarding the efficacy of DPCP immunotherapy is variable. The largest clinical trial ever performed showed a total success rate of 60%; however, among those with Alopecia Totalis (AT) / Alopecia Universalis (AU), this rate was 17.4%. Still in this trial, it was found that 38% of patients with a good response maintained it after 31 months of follow-up, with this being attributed to a slow reduction in concentration, followed by drug discontinuation.7
Factors associated with worse response to topical immunotherapy were, early age at disease onset, prolonged time of hair loss, length of illness, personal history of atopy and AA, nail involvement, and other associated autoimmune disorders. The main factor associated with recurrence was abrupt withdrawal from therapy.
1. Islam N, Leung PSC, Huntley AC, Gershwin ME. The autoimmune basis of alopecia areata: a comprehensive review. Autoimmun Rev. 2015; 14(2):81-9.
2. Lundin M, Chawa S, Sachdev A, Bhanusali D, Seiffert-Sinha K, Sinha A. Gender Differences in Alopecia Areata. J Drugs Dermatol. 2014;13(4):409-13.
3. Madani S, Shapiro J, et al. Alopecia areata update. J Am Acad Dermatol 2000;42(4):549-66.
4. Alzolibani AA. Epidemiologic and genetic characteristics of alopecia areata (part 1). Acta Dermatoven APA 2011; 20(4): 191-8.
5. Donovan J, Salsberg JM. The safety and efficacy of diphencyprone for the treatment of alopecia areata in children. Arch Dermatol. 2012;148(9):1084-5.
6. Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sladden M. British association of dermatologists' guidelines for the management of alopecia areata. Br J Dermatol. 2012; 166 (5):916-26.
7. El-Zawahry BM, Azzam OA, Zaki NS, Abdel-Raheem HM, Bassiouny DA, Khorshied MM. PTPN22 gene polymorphism in Egyptian alopecia areata patients and its impact on response to diphencyprone immunotherapy. Gene. 2013; 523(2):147-51.
8. Durdu M, Özcan D, Baba M, Seçkin D. Efficacy and safety of diphenylcyclopropenone alone or in combination with anthralin in the treatment of chronic extensive alopecia areata: A retrospective case series. J Am Acad Dermatol 2015; 72(4): 640-50.
9. Happle R, Hausen BM, Wiesner-Menzel L. Diphencyprone in the treatment of alopecia areata. Acta Derm Venereol 1983;63(1):49-52.
10. Chiang KS, Mesinkovska NA, Piliang MP, Bergfeld WF. Clinical Efficacy of Diphenylcyclopropenone in Alopecia Areata: Retrospective Data Analysis of 50 Patients. J Investig Dermatol Symp Proc. 2015;17(2):50-5.
This study was performed at the Universidade Católica de Campinas (PUC-Campinas) – Campus II, and at the Hospital e Maternidade Celso Pierro, Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}