


Maria Claudia Almeida Issa1; Mariana Boechat2; Aline Cairo Fassini3
Introduction: Daylight photodynamic therapy (PDT) is a recent therapeutic modality for actinic keratoses and field cancerization. The association of techniques to PDT for transepidermal delivery of the photosensitizer is a new option for the treatment of photodamaged skin with actinic keratosis.
Objective: To evaluate the clinical efficacy and the adverse events of photodamaged skin treatment through the transepidermal drug delivery and daylight-PDT.
Methods: Seven patients with phototype II and III, aged 60-73 years, with photodamaged skin, with and without actinic keratoses, were submitted to the association of methods (CO2 laser, micro-abrasion or microneedling) and daylight-PDT. Two sessions were performed with two weeks intervals. MAL was applied after micro-abrasion and after CO2 laser, but before the micro-needling. All patients were exposed to daylight for a period of 2 hours. Clinical evaluations were performed before, 15 days and three months after treatment.
Results: CO2 laser associated with daylight-PDT was more effective in overall improvement of the skin (texture, pigmentation and wrinkles). Microneedling associated with daylight-PDT was effective in improving texture and pigmentation. Micro-abrasion proved to be effective when combined with microneedling. Excellent improvement of actinic keratosis lesions was achieved with all associations of techniques. Adverse events were transient and more intense with the association of CO2 Laser.
Conclusion: Association of TDD with daylight-PDT was effective in the treatment of photodamaged skin and safe in all protocols.
Keywords: PHOTODYNAMIC THERAPY, PHOTOSENSITIZER, LIGHT, ACTINIC KERATOSIS, PHOTOAGING.
Chronic exposure to sunlight increases the incidence of nonmelanoma skin cancer, to be included of actinic keratosis (AK), basal cellular carcinoma and spinocellular carcinoma. It is also responsible for the photoaging of the skin, observed clinically by the presence of wrinkles, erythema, coarseness, telangiectasia and irregular pigmentation.1 Among treatment options for photodamaged skin with AK, conventional photodynamic therapy (c-PDT) stands out due to its high efficacy and excellent cosmetic results. Some factors, such as side-effects (pain, erythema and edema), the incubation time of the methyl aminolevulinate (MAL) lasting 3 hours under an occlusive dressing and the need of an artificial lamp for the lighting, may be limiting for patients and doctors.2, 3
Over the last few years, studies have reported the efficacy of a new technique, which follows the same principle of c-PDT, but uses daylight as a source of light (fraction of visible sunlight). Daylight Photodynamic Therapy (DLPDT) is well tolerated by the patient. Pain is either absent or discrete during the lighting, and cutaneous reaction in the period following the procedure, such as erythema and edema, are minimal.4-11
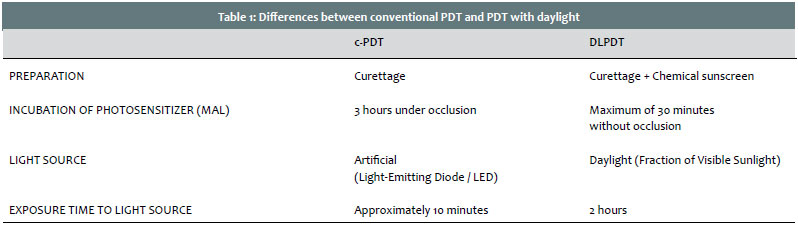
The treatment protocols of the conventional form and with the sunlight differ in several aspects (Table 1). With c-PDT, the MAL must be applied to the previously curetted skin, and maintained under occlusion for a period of 3 hours. After this incubation period, the skin is exposed to a source of artificial light (red LED) for approximately 10 minutes, which is equivalent to a dose of 37J/cm2. With the DLPDT, the MAL is applied without occlusion over the previously curetted area and with the chemical sunscreen. The patient must be exposed to daylight, in up to 30 minutes after the procedure, and remain under it for a period of 2 hours. DLPDT minimizes the disadvantages of c-PDT, and maintains its efficacy in the treatment of actinic keratosis and cutaneous field cancerization.4-11
Regardless of the type of light that is being used, artificial or daylight, the penetration of the photosensitizer through the stratum corneum layer in the area of the skin that is to receive treatment remains a limiting factor of the technique. Inasmuch, a new possibility for the PDT is the association of techniques that may augment the penetration of the photosensitizer. This new therapeutic modality is called transepidermal drug delivery (TED). Among the most recently described techniques for performing TED are microneedling12-14 and the fractional ablative methods, such as fractional ablative radiofrequency and the CO2 and Erbium lasers.15-19 Microneedling acts by "pushing" the medication through the perforations caused during its application on the cutaneous surface. The fractional ablative methods promote the production of pathways within the epidermis all the way to the papillary dermis, depending on the parameters being used, which permeate the substances applied topically. Microdermabrasion collaborates with simple curettage in order to remove the topmost layers of the epidermis.
Several studies have reported the association of fractional ablative methods with a method for potentializing the efficacy of the c-PDT.20-24 Also, it is mentioned that this clinical response, potentialized by the association of TED with c-PDT may be attained even with a time reduction in the incubation of MAL to one hour.15 The association of TED with DLPDT however, is still rarely mentioned in the medical literature. The efficacy in the association of the CO2 laser with the DLPDT in the treatment of actinic keratosis in transplanted patients was recently reported by Togsverd-Bo et al in 2015.25
Based on recent data found in the medical literature, we have proposed this pilot study, which seeks to clinically evaluate the modifications induced by this association (TED + DLPDT), by comparing different protocols and techniques.
CLINICAL TRIAL STUDY DESIGN
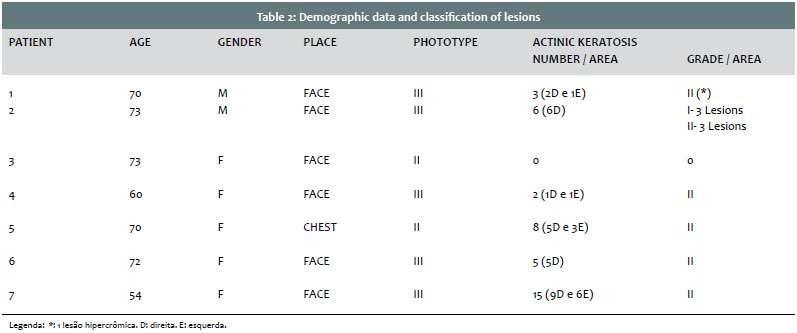
A non-randomized prospective pilot study was done with 7 patients from both genders, phototypes II and III, aged between 60 and 73 years old, presenting photodamaged skin on the face and chest (degrees III and IV on the Glogau scale), with and without actinic keratosis. Patients who were smokers, pregnant, diagnosed with photosensitivity, malignant neoplasm, collagenosis, local or systemic infections, immunodepression or were making use of photosensitive substances. All patients were photographed and signed a consent and clarification form in order to take part in the study. The procedures took place at the researcher's private clinic, which allowed for the usage of her own CO2 laser (I-Pixel CO2 – Alma Lasers, Caesarea, Israel), her crystal peeling device (by the company Pan Electronic, Rio de Janeiro, Brazil), and donated the derma rollers (Doctorroller-2,5mm, Moohan Enterprise Ltd, Gwangju, South Korea). The MAL was donated by Galderma Pharmaceutical Industry (Galderma Indústria Farmacêutica). The patients had no financial expenditures but their transportation costs. The researchers involved received no remuneration.
The treatment was comprised of undergoing one or two MAL-TFD sessions with daylight, two weeks apart, in combination with the transepidermal application techniques of MAL (aluminum oxide crystal microdermabrasion – crystal peeling; microneedling; and fractional CO2 ablative laser). In some cases, cosmeceuticals, such as vitamin C and depigmenting agents (Skinceuticals, L'Oréal, Paris, France) were combined with the MAL for drug delivery. After each session, the patients were told to apply a wound healing cream that contained dexpanthenol (3x/day for 7 days) and SPF50 sunscreen (Actinica® Galderma, Paris, France). Prophylaxis was carried out using an antiviral (acyclovir) at its full dosage for five days in all patients who underwent laser and microneedling procedures. Applying the sunscreen was the first step of the protocol, even before all other procedures, except for those cases in which microdermabrasion with crystal peeling was used.
The photosensitizer used was the 16% MAL cream (Metvix®, GALDERMA, Paris, France) in the amount of 1 gram per session (face or cleft) in all patients. However, the order it was applied varied according to the method of TED that was used. Thus, the MAL was applied after the microdermabrasion and after the CO2 laser, however it was always applied before the microneedling. It was only in one patient that two TED techniques were used in the same area in one single session. In this case, the MAL was applied after the microdermabrasion and before the microneedling. In every situation, however, the MAL was applied after the sunscreen.
All patients were exposed to daylight within 30 minutes of the MAL application, remaining exposed for 2 hours (open and well-lit space) before returning to the clinic for the skin cleansing with 0.9% Saline, reapplication of sunscreen and clinical evaluation of the immediate effects.
TECHNIQUES FOR TRANSEPIDERMAL APPLICATION OF DRUGS
1. Aluminum Oxide Crystal Microdermabrasion (Crystal Peeling):
Before the simple curettage and the application of MAL, many scrubs in different directions were performed (vertical, horizontal and oblique) until a homogeneous erythema in the entire area was reached.
2. Microneedling:
The derma roller with 2.5mm needles was used immediately after the application of the MAL photosensitizer. Several scrubs in different directions were performed (like an asterisk), without causing bleeding.
3. Fractional Ablative CO2 Laser:
It was applied after the curettage of the lesions, and immediately before the application of MAL, with the following parameters: 60 watts of power, fluence of 20 mJ/pixel, spacing of 3 mm in between the pixels, with one single scrub of the whole area, using a roller tip.
CLINICAL EVALUATION
The patients had follow-ups for a period of 3 months in order to evaluate the cure rate of the actinic keratoses and the overall degree of improvement of the skin (texture, wrinkles and pigmentation). Evaluations took place before the procedures first began, 15 days after the first session and 3 months after the treatment.
Texture (coarseness), color (pigmentation) and wrinkles analysis were conducted by the means of qualitative parameters, using the Glogau Aging Scale. The degree of improvement was evaluated in accordance to the quartile scale proposed by Alster et al26, which considers improvement as minimal (<25%); moderate (25%-50%); significant (51%-75%), and excellent (>75%).
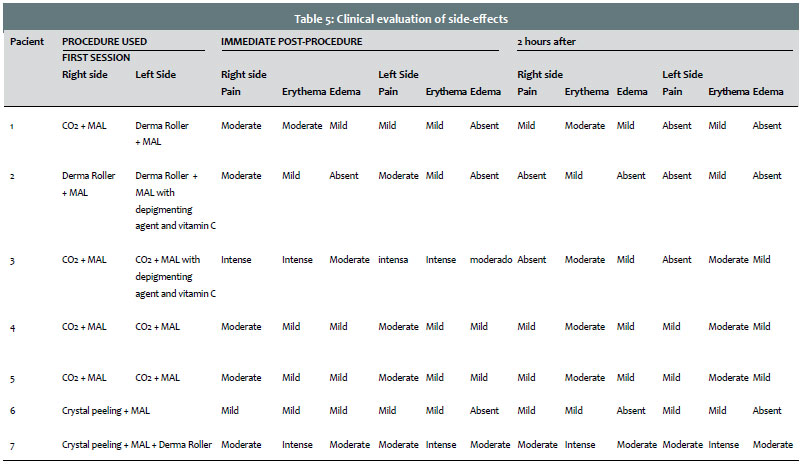
The evaluation concerning the improvement in the actinic keratosis lesions was done with quantitative parameters (lesion count), and also qualitative in accordance to thickness levels (grades 1, 2 and 3). The side effects (pain, erythema and edema) were evaluated by an intensity scale varying from absent, mild, moderate and intense, in the periods immediately following the procedure and two hours after having been exposed to sunlight.
CLINICAL CASES
Case 1:
ID: Male, 70 years old, phototype III (Table 2).
Actinic Keratosis: 3 AK lesions, grade II (2 on the right side, one being hyperchromatic; and 1 on the left side).
Aging Grade: Glogau Type III.
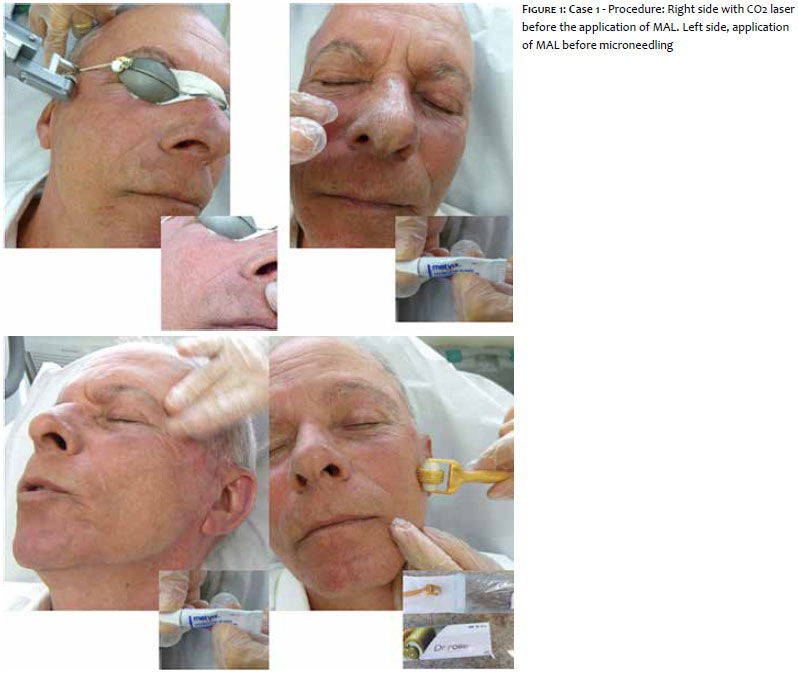
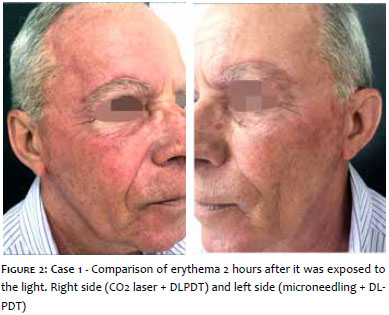
Procedure: face: Two sessions of MAL-DLPDT in combination with the fractional CO2 ablative laser on the right hemiface and microneedling on the lift hemiface (Figure 1).
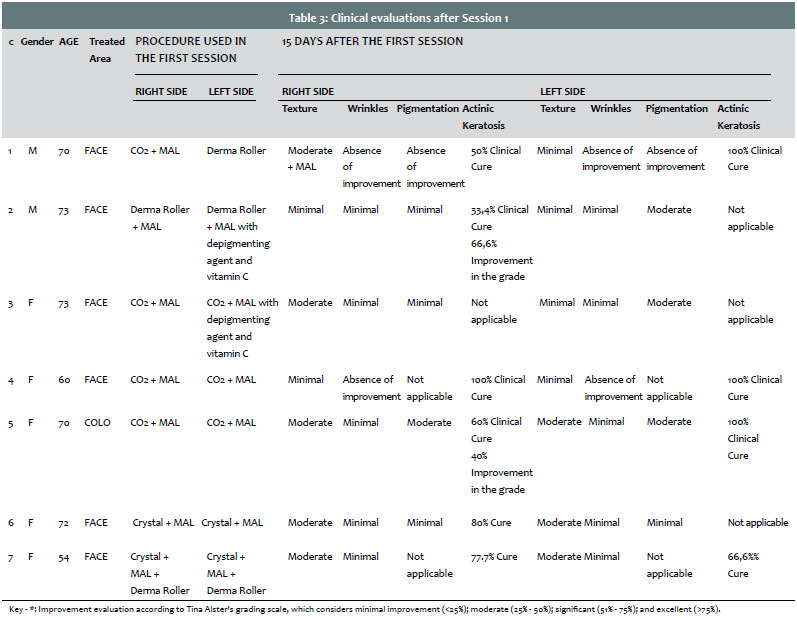
Post Immediate: Side treated with the CO2 laser (right): moderate pain; moderate erythema; mild edema. Side treated with the microneedling (left): mild pain; mild erythema; absence of edema (Table 3).
After 2 hours: Side treated with the CO2 laser (right): mild pain; moderate erythema; mild edema. Side treated with the microneedling (left): absence of pain; mild erythema; absence of edema (Figure 2). (Table 3).
After 15 days: Side treated with the CO2 laser (right): showed moderate improvement in texture; showed no improvement in wrinkles and pigmentation; and 50% clinical cure of the actinic keratosis lesions. Side treated with the microneedling (left): showed minimum improvement in texture; absence of improvement in wrinkles and pigmentation; and 100% clinical cure of actinic keratosis (Table 4).
Results after 3 months: On the side treated with the CO2 laser (right), there was significant improvement in texture, minimum improvement in wrinkles and pigmentation (Figure 3). The cure rate of the AK was 50%, without improvement of the hyperchromatic lesion. On the side treated with microneedling (left), there was moderate improvement in texture. There was no improvement in wrinkles nor in pigmentation. The AK lesion was cured (Table 5).
Case 2:
ID: Male, 73 years old, phototype III (Table 2).
Actinic Keratosis: 6 AK lesions on the right hemiface (3 grade II and 3 grade III).
Aging Grade: Glogau Type III.
Procedure: face: Two sessions of MAL-DLPDT in combination with microneedling on both hemifaces. On the right hemiface, MAL was used isolatedly, and on the left hemiface, MAL was combined with a depigmenting agent and vitamin C.
Post immediate: Moderate pain; mild erythema; absence of edema on either side. (Table 3).
After two hours: Absence of pain; mild erythema; absence of edema on either side. (Table 3).
After 15 days: On the side treated with a combination of microneedling and MAL (right), there was minimum improvement in texture, wrinkles and pigmentation; 33.4% clinical cure and 66.6% improvement in the actinic keratosis grade. On the side treated with a combination of microneedling and MAL + depigmenting agents with vitamin C (left), there was minimum improvement in texture and wrinkles, and moderate improvement in pigmentation. (Table 4).
Results after 3 months: On the side treated with a combination of microneedling and MAL (right), there was significant improvement in texture, and minimum improvement in wrinkles and pigmentation. The cure rate of the AK was 83.3%, with 16.7% being reduced from grade III to grade II (Figure 4). On the side treated with a combination of microneedling and MAL + depigmenting agents with vitamin C (left), (Figure 5), there was significant improvement in texture; minimum improvement in wrinkles; moderate improvement in pigmentation (Table 5).
Case 3:
ID: Female, 73 years old, phototype III (Table 2).
Actinic Keratosis: absent.
Aging Grade: Glogau Type III.
Procedure: face: Two sessions of MAL-DLPDT in combination with the fractional CO2 ablative laser on both hemifaces. On the right hemiface, the MAL was applied isolatedly, on the left hemiface the MAL was combined with a depigmenting agent + vitamin C.
Post immediate: Intense pain and erythema and moderate edema on either side. (Table 3).
After 2 hours: Absence of pain; mild edema; moderate erythema on either side. (Table 3).
After 15 days: On the side treated with a combination of CO2 and MAL (right), there was moderate improvement in texture; and minimum improvement in wrinkles and pigmentation. On the side treated with a combination of CO2 and MAL + depigmenting agent + vitamin C (left), there was moderate improvement in texture; minimum improvement in wrinkles and pigmentation. (Table 4).
Results after 3 months: On the side treated with a combination of CO2 and MAL (right), there was significant improvement in texture and in wrinkles, with moderate improvement in pigmentation.
On the side treated with a combination of CO2 and MAL + depigmenting agent + vitamin C (left), (Figure 6), there was significant improvement in texture, wrinkles and pigmentation. (Table 5).
Case 4:
ID: Female, 60 years old, phototype III (Table 2).
Actinic Keratosis: 2 AK lesions, grade II (1 on the right side and 1 on the left side).
Aging Grade: Glogau Type IV.
Procedure: face: Two sessions of MAL-DLPDT in combination with the fractional CO2 ablative laser on both hemifaces.
Post immediate: Moderate pain; mild erythema; mild edema, on both sides. (Table 3).
After 2 hours: Mild pain; moderate erythema; mild edema, on both sides. (Table 3).
After 15 days: There was minimum improvement in texture; there was no improvement in wrinkles nor in pigmentation; and 100% clinical cure of the actinic keratosis on both sides (Table 4).
Results after 3 months: Moderate improvement in texture, minimum improvement in wrinkles. The cure rate of the AK was 100% on both sides (Table 5).
Case 5:
ID: Female, 70 years old, phototype II (Table 2).
Actinic Keratosis: 8 AK lesions, grade II (5 on the right side and 3 on the left side).
Aging Grade: Glogau Type III.
Procedure: cleft: Two sessions of MAL-DLPDT in combination with the fractional CO2 ablative laser on both sides of the cleft (divided by an imaginary line between the sternum furcula and the xiphoid process).
Post immediate: Moderate pain; mild erythema; mild edema on both sides. (Table 3).
After 2 hours: Mild pain; moderate erythema; mild edema on both sides. (Table 3).
After 15 days: On the right side, there was moderate improvement in texture and pigmentation, and minimum improvement in wrinkles; with 60% clinical cure and 40% improvement actinic keratosis grading. On the left side, there was moderate improvement in texture and pigmentation; and minimum improvement in wrinkles; with 100% clinical cure of actinic keratosis (Table 4).
Results after 3 months: Significant improvement in texture, moderate improvement in wrinkles and pigmentation on both sides (Figure 7). The cure rate of AK was 80%, with 20% improvement in the reduction grading of the keratosis (from II to I) on the right side. On the left side, the cure rate was 100% (Table 5).
Case 6:
ID: Female, 72 years old, phototype III (Table 2).
Actinic Keratosis: 5 AK lesions, grade II, right side.
Aging Grade: Glogau Type III.
Procedure: face: One single session of MAL-DLPDT in combination with microdermabrasion (crystal peeling) on both hemifaces.
Post Immediate: Mild pain and erythema; absence of edema on either side. (Table 3).
After 2 hours: Mild pain and erythema; absence of edema on either side. (Table 3).
After 15 days: There was moderate improvement in texture, and minimal improvement in wrinkles and pigmentation on both sides.
On the right side, there was 80% clinical cure and 20% improvement in the actinic keratosis grading. (Table 4).
Results after 3 months: Moderate improvement in texture, minimal improvement in wrinkles and pigmentation. The cure rate of the AK was of 100% (Table 5).
Case 7:
ID: Female, 54 years old, phototype III (Table 2).
Actinic Keratosis: 15 AK lesions, grade II (9 on the right side and 6 on the left side).
Aging Grade: Glogau Type III.
Procedure: face: One single session of MAL-DLPDT in combination with microdermabrasion (crystal peeling) + microneedling on both hemifaces.
Post Immediate: Moderate pain and edema; intense erythema on both sides. (Table 3).
After 2 hours: Moderate pain and edema; intense erythema on both sides. (Table 3).
After 15 days: For both hemifaces, there was moderate improvement in texture; and minimal improvement in wrinkles. On the right side, there was 77.7% clinical cure and 22.3% improvement in the actinic keratosis grading. On the left side, there was 66.6% clinical cure and 33.4% improvement in the actinic keratosis grading (Table 4).
Results after 3 months: Significant improvement in texture and in wrinkles on both sides (Figures 8 and 9). The cure rate of the AK was 88.8% on the right side, with an improvement in the actinic keratosis grading (from II to I) in 11.2%. On the left side, the cure rate of the keratosis was 100% (Table 5).
The CO2 Laser in combination with DLPDT was more effective in the overall improvement of the skin, mainly in the improvement of wrinkles, when compared to microneedling. Microneedling in combination with DLPDT has proven to be effective in the improvement of texture and pigmentation, mainly when combined with cosmeceutical depigmenting agents. The combination of two TED (microdermabrasion with microneedling) techniques with DLPDT was more effective in the improvement of texture, pigmentation and wrinkles when compared to the use of techniques isolatedly. Excellent improvement in the actinic keratosis lesions was attained with techniques that were combined with TED and DLPDT.
Among all possible side-effects, pain, erythema and edema were observed in most patients. However, these side-effects were observed with greater intensity (moderato to intense) with protocols in which the CO2 Laser was used. Side effects were mild to moderate when using microdermabrasion or microneedling. The case in which two techniques were combined, microdermabrasion and microneedling to DLPDT, erythema, edema and pain were more intense.
Several studies have already shown an increase in effectiveness of conventional PDT in the treatment of actinic keratosis and field cancerization, in combination with methods to increase the permeation of the photosensitizer.22-24 However, there is a lack of studies regarding the combination of TED with PDT while using daylight. This pilot study is the first of its kind to be conducted in Brazil with the goal to evaluate TED technique with DLPDT.
In the international medical literature, Togsverd-Bo et al25 have compared the efficacy of isolated DLPDT with DLPDT in combination with the fractional CO2 ablative laser in the treatment of actinic keratosis with transplanted patients. In our study, we have evaluated the combination of DLPDT with the CO2 laser and, also, with microneedling and microdermabrasion in the treatment of photodamaged skin with and without actinic keratosis in immunocompetent patients. Togsverd-Bo et al25 have reported erythema and edema to be more intense in the areas treated with DLPDT when combined with the laser after the procedure, with no long-term change in pigmentation. In our cases, we have also observed a mild increase of erythema and edema immediately after the laser treatment and, also, after daylight exposure, which were transitory, not leading to postinflammatory pigmentation. We have also observed the overall improvement of the skin (texture, fine wrinkles and pigmentation) in varying intensity, according to the other techniques (laser and non-laser) in combination with DLPDT. The clinical response was more evident when combined with the CO2 laser, and also when we combined the DLPDT to the microdermabrasion with microneedling. The response in pigmentation was slightly better when we combined depigmenting agents and vitamin C to the MAL, either before the microneedling or after the CO2 laser.
Based on the methodology that was used, it is possible to state that the combination of methods such as the CO2 laser, microdermabrasion and microneedling with DLPDT has proven to be effective in the treatment of photodamaged skin, with improvement of actinic keratosis, texture, pigmentation and wrinkles. The combination of TED and DLPDT was safe in all protocols that it was used.l
1. Issa MCA, Manela-Azulay M. Terapia fotodinâmica: revisão da literatura e documentação iconográfica. An Bras Dermatol. 2010;85 (4):501-511.
2. Kalka K, Merk H, Mukhtar,H. Photodynamic Therapy In Dermatology. J Am Dermatol 2000; 42 (3): 389-413.
3. Morton CA. Photodynamic therapy for nonmelanoma skin cancer. Arch Dermatol. 2004;140(1): 116-120.
4. Braathen LR. Daylight Photodynamic Therapy in Private Practice in Switzerland: Gain Without Pain. Acta Derm Venereol. 2012; 92(6):652-3.
5. Morton CA, Wulf HC, Szeimies RM. Practical approach to the use of daylight photodynamic therapy with topical methyl aminolevulinate for actinic keratosis: a European consensus. J Eur Acad Dermatol Venereol. 2015;29 (9):1718-23.
6. Wiegell SR, Wulf HC, Szeimies RM, Basset-Seguin N, Bissonnette R, Gerritsen MJ, et al. Daylight photodynamic therapy for actinic keratosis: an international consensus: International Society for Photodynamic Therapy in Dermatology. J Eur Acad Dermatol Venereol. 2012; 26(6): 673–9.
7. Rubel DM, Spelman L, Murrell DF, See JA, Hewitt D, Foley P, et al. Daylight PDT with methyl aminolevulinate cream as a convenient, similarly effective, nearly painless alternative to conventional PDT in actinic keratosis treatment: a randomized controlled trial. Br J Dermatol 2014; 171(5): 1164–1171.
8. Lacour J. Results of 2 randomised, controlled, phase III studies with Daylight- PDT in Australia and Europe. Euro-PDT 14th Annual Congress; April 4th–5th, 2014; Nice, France.
9. Wiegell SR, Haedersdal M, Philipsen PA, Eriksen P, Enk CD, Wulf HC. Continuous activation of PpIX by daylight is as effective as and less painful than conventional photodynamic therapy for actinic keratoses – a randomized, controlled study. Br J Dermatol. 2008; 158(4): 740–6.
10. Wiegell SR, Haedersdal M, Eriksen P, Wulf HC. Photodynamic therapy of actinic keratoses with 8% and 16% methyl aminolaevulinate and home-based daylight exposure: a double-blinded randomized clinical trial. Br J Dermatol. 2009; 160(6):1308–14.
11. Wiegell SR, Fabricius S, Stender IM, Berne B, Kroon S, Andersen BL, et al. A randomized, multicenter study of directed daylight exposure times of 1½ vs. 2½ h in daylight-mediated photodynamic therapy with methyl aminolaevulinate in patients with multiple thin actinic keratoses of the face and scalp. Br J Dermatol. 2011; 164(5):1083–90.
12. Donelly RF, Morrow DI, McCarron PA, Woolfson AD, Morrissey A, Juzenas P, et al . Microneedle-mediated intradermal delivery of 5-aminolevulinic acid: potential for enhanced topical photodynamic therapy. J Control Release. 2008;129 (3):154-62.
13. Mikolajewska P, Donnelly RF, Garland MJ, Morrow DI, Singh TR, Iani V, et al. Microneedle pre-treatment of human skin improves 5-aminolevulininc acid (ALA)- and 5-aminolevulinic acid methyl ester (MAL)-induced PpIX production for topical photodynamic therapy without increase in pain or erythema. Pharm Res. 2010;27(10):2213-20.
14. Torezan L, Chaves Y, Niwa A, Sanches JA Jr, Festa-Neto C, Szeimies RM. A pilot split-face study comparing conventional methyl aminolevulinate-photodynamic therapy (PDT) with microneedling-assisted PDT on actinically damaged skin. Dermatol Surg. 2013;39(8):1197-201.
15. Kassuga LEBP, Issa MCA, Chevrand NS. Transepidermal application of medication combined with photodynamic therapy in the treatment of actinic keratosis. Surg Cosmet Dermatol. 2011;3 (4):89-92.
16. Letada PR, Shumaker PR, Uebrlhoer NS. Demonstration of protoporphiryn IX (PpIX) localized to area of palmar skin injected with 5 aminolevulinic acid (ALA) and pre-treated with a fractionated CO2 laser prior to topically applied ALA. Photodiagnosis Photodyn Ther. 2010; 7(2):120-2.
17. Haerdersdal M, Sakamoto FH, FarinelliWA, Doukas AG, Tam J, Anderson RR. Fractional CO2 laser-assisted drug delivery. Laser Surg Med. 2010; 42(2):113-22.
18. Shen SC, Lee WR, Fang YP, Hu CH, Fang JY. In vitro percutaneous absorption and in vivo protoporphiryn IX accumulation in skin and tumors after topical 5-aminolevulinic acid application with enhancement using an Erbium:YAG laser. J Pharm Sci.2006; 95(4):929-38.
19. Fang JY, Shen SC, Lee WR, Fang YP, Hu CH. Enhancement of topical 5-aminolevulinic acid delivery by Erbium:YAG laser and microdermoabrasion: a comparison of iontophoresis and electroporation. Br J Dermatol. 2004 Jul; 151(1):132-40.
20. Yoo KH, Kim BJ, Kim MN. Enhanced efficacy of photodynamic therapy with methyl 5-aminolevulinic acid in recalcitrant periungual warts after ablative carbon dioxide fractional laser: a pilot study. Dermatol Surg 2009; 35(12):1927-32.
21. Fukui T, Watanabe D, Tamada Y, Matsumoto Y. Photodynamic therapy following carbon dioxide laser enhances efficacy in the treatment of extramammary Paget's disease. Acta Derm Venereol 2009;89(2):150-4.
22. Song HS, Jung SE, Jang YH, Kang HY, Lee E, Kim YC. Fractional carbon dioxide laser-assisted photodynamic therapy for patients with actinic keratosis. Photodermatol. Photoimmunol. Photomed 2015; 31(6): 296–301.
23. Jang YH, Lee DJ, Shin J, Kang HY, Lee ES, Kim YC. Photodynamic therapy with ablative carbon dioxide fractional laser in treatment of actinic keratosis. Ann Dermatol Vol. 2013; 25(4): 417-22.
24. Togsverd-Bo K, Haak CS, Thaysen-Petersen D, Wulf HC, Anderson RR, Hædesdal M. Intensified photodynamic therapy of actinic keratoses with fractional CO2 laser: a randomized clinical trial. Br J Dermatol. 2012; 166(6): 1262–9.
25. Togsverd-Bo K, Lei U, Erlendsson AM, Taudorf EH, Philipsen PA, Wulf HC, et al. Combination of ablative fractional laser and daylight-mediated photodynamic therapy for actinic keratosis in organ transplant recipients - a randomized controlled trial. Br J Dermatol 2015; 172 (2): 467-74.
26. Alster TS, Tanzi EL, Welsh EC. Photorejuvenation of facial skin with topical 20% of 5- aminolevulinic acid and intense pulsed light treatment: a split face comparison study. J Drugs Dermatol 2005;4(1):35-8.
This study was performed at a private practice in Niterói (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}