


Maria Claudia Almeida Issa1; Mariana Boechat2; Aline Cairo Fassini3
Conventional Photodynamic Therapy (c-PDT), approved in Brazil since 2006 for non-melanoma skin cancer, is a well-established treatment worldwide. The evolution of PDT, in the last 10 years, includes its use in other indications, its association with techniques that promote increased photosensitizer permeation and use of daylight instead of artificial light. This new method, which uses daylight, was approved in Brazil in 2014 for the treatment of actinic keratosis and field cancerization, with the benefit of maintaining c-PDT's efficacy without adverse events.
Keywords: PHOTOCHEMOTHERAPY; LIGHT; SKIN NEOPLASMS; KERATOSIS, ACTINIC
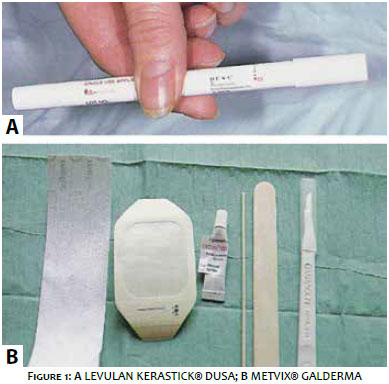
Topical Photodynamic Therapy (PDT) is defined as a photochemical reaction used to cause selective destruction of a tissue through the formation of singlet oxygen and other reactive oxygen species, which accumulate in malignant and premalignant cells, producing a cytotoxic effect. In order for this reaction to take place, a photosensitizer on the target tissue, a specific light source to excite the photosensitizer, and the presence of oxygen are needed.1,2 The most commonly used topical photosensitizers are Aminolevulinic Acid (ALA) and Methyl Aminolevulinate (MAL) (Figure 1). Both are prodrugs, and need to be modified enzymatically within the cell into protoporphyrin IX (PpIX), which is the endogenous photosensitizer. For the procedure, a mild curettage should be performed prior to the application of the photosensitizer (either ALA or MAL), which will remain on the skin under occlusion, before exposure to light (Figure 2). Among light sources used in conventional Photodynamic Therapy (c-PDT), broad-spectrum light emitting diodes (LEDs), Intense Pulsed Light (IPL) and lasers are available.3-5
c-PDT has a more precise indication in the treatment of Non-Melanoma Skin Cancer (NMSC), and is approved for Actinic Keratosis (AK), low-risk superficial Basal Cell Carcinoma (BCC), and Bowen's Disease.6-8 Among the off-label indications, the photoaging treatment that was based on the findings of overall skin quality improvement (wrinkles, texture and pigmentation) during the treatment of the field cancerization.9-15
A new technique that uses the fraction of visible light from solar radiation is called Daylight Photodynamic Therapy (DLPDT). Several studies report that DLPDT has the same efficacy as c-PDT in the treatment of AK lesions and field cancerization, but with fewer side effects. This new therapy is not indicated for treatment of carcinomas.16-23
More recently, fractional ablative methods (Radiofrequency Ablation, and Erbium Laser or CO2) and microneedling have been used for Transepidermal Drug Delivery (TED).24-42 The use of TED has been related for the treatment of different dermatoses, and its combination with PDT in order to increase the penetration of ALA or MAL seems to potentialize the results of c-PDT or even PDT with sunlight.
In 1999, the Food and Drug Administration (FDA) approved 5-Aminolaevulinic Acid ALA (Levulan Kerastick®, DUSA Pharmaceuticals, Massachusetts, USA) for multiple actinic keratoses. In 2002, the esterified derivative of ALA, Methyl Aminolevulinate -MAL (Metvix ®, Galderma, Paris, France) was approved in Europe for Actinic Keratoses and Basal Cell Carcinoma. MAL was later approved in the USA in 2004 for actinic keratoses. In 2006, the MAL had its approval widely diffused in the world. At that time, it was approved in Brazil for actinic keratoses and basal cell carcinoma. It was only in 2008 that Levulan arrived in Brazil, having been distributed for a short period. In 2009, MAL was also approved for Bowen's Disease in our country. The innovation of the technique by using daylight for MAL activation was approved in Brazil in 2014 and in Europe in 2015.
Conventional Photodynamic Therapy in the Treatment of Non-Melanoma Skin Cancer
AK presents molecular and genetic alterations similar to Squamous Cell Carcinoma (SCC) lesions, and some authors consider it a carcinoma in situ. Others consider it a premalignant lesion, with an annual transformation rate into SCC of between 0.25% and 16% within 10 to 25 years.43,44 Among the treatments used for AK are cryosurgery, electrocoagulation, topical medications, surgical excision, and PDT. In general, the use of topical PDT for treatment of AK has a cure rate between 73% and 100%. PDT has similar or superior efficacy when to compared to conventional treatments, as well as being a quick and easy-to-apply method with a short recovery time and excellent cosmetic result.45-47 In a study conducted by Freeman et al48, MAL-PDT was statistically more effective than a single freeze-thaw cycle with liquid nitrogen spray.
Dragieva et al49 evaluated the efficacy of PDT with MAL in transplant patients. The double-blind study with 2 sessions of MAL-PDT or placebo, with a 1-week interval, was performed in 17 patients with a total number of 129 AK lesions. The study concluded that treatment with MAL-PDT is safe and effective in treating AK in transplanted patients and may reduce the risk of transformation to invasive Squamous Cell Carcinoma.
Basal Cell Carcinoma (BCC) is the most common cutaneous malignant tumor (70%) in adulthood. Its treatment should be chosen according to the clinical type, histology, size and location of the tumor. Among the therapeutic options are surgical excision (gold standard), electrocoagulation and curettage, cryotherapy, immunomodulators, cytotoxic agents and radiotherapy. Although a better result is described with MAL, possibly due to the greater lipophilicity, greater selectivity and penetration capacity,50 the clinical and histopathological characteristics, and aggressive nature of the tumor are important factors for the correct indication of PDT. Statistical data based on multicenter, multi-patient, five-year follow-up studies reveal that PDT with MAL-Red Light achieves a cure rate of approximately 95% in the treatment of superficial BCC, and 73% to 94% for nodular BCC at the evaluation after 3 months. The recurrence rate for superficial BCC is approximately 22%, similar to conventional treatments, such as cryotherapy with a recurrence rate of around 19%. For nodular BCC, in the long term, the rate of recurrence is close to 14%, higher when compared to a recurrence of only 4% of the surgery.46,51
With regard to Bowen's disease, comparative studies between MAL-PDT, cryotherapy and 5-fluorouracil (5-FU) showed superior cosmetic outcome with MAL-PDT, and, after 24 months, cure rates of 68% for MAL-PDT, 60% for Cryotherapy, and 59% for 5-FU. c-PDT is well indicated for the treatment of large-diameter lesions located in the lower limbs, which present great difficulty in cicatrization after surgical procedure or cryotherapy.51
Conventional Photodynamic Therapy: Off-Label Indications
Exposure to ultraviolet radiation is the leading cause of skin disorders such as sunburn, photodamage, and skin cancer. The visible signs of photodamaged skin are characterized by wrinkles, rough skin texture, altered pigmentation, telangiectasias and, in some cases, AK and carcinomas (BCC and SCC).14, 15, 52 Light-based technologies (LEDs, LIP and Laser) in an isolated way, without photosensitizer, act on the pigmentary and vascular alterations, in addition to inducing the synthesis of collagen in the photodamaged skin. However, only PDT, in combination with the light and photosensitizer, also treats AK.11, 53, 54
In addition to the clinical improvement of photodamaged skin, which is widely reported in the literature, some authors have described histological and immunohistochemical modifications induced by c-PDT, such as: better organization of elastic fibers, increased density of collagen fibers, increased metalloproteinases.14, 15, 55
Other off-label indications include the treatment of inflammatory acne, viral warts, leishmaniasis, necrobiosis lipoidica, granuloma annulare, mycosis fungoides, and extramammary Paget's disease.24, 25 For all these indications, the mechanisms of action are poorly understood and results are varied. Therefore, PDT should not be considered as the first choice treatment, and should be indicated in specific cases.
Transepidermal Application of Medicine Associated with Conventional Photodynamic Therapy
TED is a new therapeutic modality in Dermatology used to increase the penetration of drugs through the more superficial layers of the skin. In the literature, old techniques with poorly understood mechanisms are cited with the objective of transposing this cutaneous barrier at different depths, including iontophoresis, electroporation and photomechanical waves.37-42 The use of ultrasound (U/S) for transepidermal administration of different molecules, such as insulin, mannitol, glucose, heparin, morphine, caffeine and lidocaine,56 both in vitro and in vivo have been described in the literature.57, 58 More recent studies on TED report the use of ablative methods for drug permeation in the treatment of various dermatological diseases, such as actinic keratosis, hypertrophic scars, stretch marks and alopecia areata.59, 60
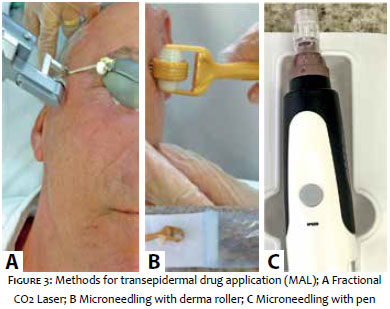
By the means of fractional ablative methods (ablative radiofrequency, Erbium laser and CO2) and microneedling (Figure 3), micro-perforations permeate drugs applied topically to the surface of the skin, surpassing its main cutaneous barrier, the stratum corneum.24-31 Fukui et al25 reported the association of fractional CO2 Laser to c-PDT for the treatment of non-melanoma skin cancer, extra-mammary Paget's disease and parakeratosis. Kassuga and Issa61 reported the clinical effects of isolated c-PDT compared to the combination of PDT with the fractional ablative radiofrequency (RF) treatment. They revealed that, even by reducing the incubation time of the photosensitizer (MAL) from 3 hours to 1 hour, this combination was more effective in reducing the number of AK lesions in the forearms than the PDT alone. In addition to improved AK, there was improvement in texture and pigmentation of all treated areas, with better rejuvenation of the side treated by RF associated with PDT.
The microneedling technique used for TED in combination with PDT has also been reported. Available in the market, there are some derma roller brands for microneedling that are rolled on the cutaneous skin, as well as motorized pens with disposable needles for stamp-type microneedling. Torezan et al 36 compared c-PDT with PDT in combination with the use of microneedles. There was no evidence of an increase in the efficacy of PDT associated with microneedles in relation to the number of AKs. However, this association improved the overall quality of the skin, reduced hyperpigmentation and sagging, and reduced deep wrinkles.
Daylight Photodynamic Therapy
Daylight PDT has been studied in Europe and Australia in recent years and was approved in Brazil in 2014, with the aim to reduce side effects and preparation time of c-PDT, while maintaining its effectiveness in the treatment of AK and field cancerization. There are no studies indicating the use of DLPDT for carcinomas.18-23
For daylight PDT to be performed, all exposed skin should be covered with pure chemical sunscreen without physical blockers. In this manner, only visible light action will be allowed on the skin while maintaining protection against ultraviolet radiation.18 After approximately 15 minutes, curettage is performed with a dermal curette. In case of discreet bleeding, gauze compression should be performed prior to the application of the MAL photosensitizer, which should not be occluded. The patient should be exposed to daylight within 30 minutes. This exposure should be performed for a period of 2 hours (Figure 4). For the whole face treatment, the amount of 1g of MAL (half a tube) is sufficient in each session.
Daytime PDT should not be performed on rainy day or on days with dark clouds that may disrupt light. However, it can be performed in other climatic conditions, such as with the presence of clear clouds. In cold-weather countries, the temperature should be adequate for patient comfort and should not be less than 10ºC so that there is no interference in the production of PpIX during the sun exposure period. Similar efficacies were achieved despite cloudy or sunny weather in studies evaluating the treatment of actinic keratoses in different countries with different latitudes and altitudes, including Brazil.18-20 In Brazil, the average luminance emitted in all months of the year and in all regions from North to South was similar to the brightness of the Australian studies, which gives us the information that DLPDT will have the same effectiveness throughout the national territory.
Daytime PDT provides excellent patient tolerability, with reports typically describing minimal pain or total absence of pain during the procedure. This can be explained by the fact that, in c-PDT, there is a large formation of PpIX during the occlusion of MAL in the treated area for 3 hours before exposure to LEDs, with subsequent great excitation of PpIX and free radical production. In contrast, in Daytime PDT, the MAL incubation time is at most 30 minutes, without occlusion, before exposure to daylight. In this manner, PpIX excitation and degradation occurs during light exposure, with gradual production of the photochemical response in this period and consequent reduction of the intensity of the inflammatory response (pain, erythema and edema).19-22
Transepidermal Drug Application in combination with Daylight Photodynamic Therapy
The clinical response of AK and the field cancerization of DLPDT is similar to the clinical response to the c-PDT with artificial light.20,21 However, the improvement of other aspects of photodamaged skin, such as wrinkles, pigmentation and sagging, appear to be less evident when compared to that of c-PDT. This fact is probably due to the lower inflammatory response induced by the visible light of the solar radiation spectrum on Protoporphyrin IX, formed simultaneously with the period of daylight exposure.
Based on studies about TED in combination with c-PDT,36,61 the authors of the present study believe that TED in combination with Daylight PDT can also bring benefits to the overall photodamaged skin treatment, with improvement not only to actinic keratosis but also to texture, wrinkles and skin pigmentation. Pilot cases, performed by us, show this new therapeutic possibility, combining Daylight PDT with TED techniques in overall skin rejuvenation (refer to article #10 published in this journal).
Topical PDT is a very useful tool for dermatology around the world, and has been approved in Brazil since 2006 for the treatment of non-melanoma skin cancer. In this period, the technique has undergone innovations and new indications that are based on international and national studies. Currently, a new PDT modality that uses daylight is also approved in our country, bringing benefits, such as the treatment of large areas, in a practical and effective way, with short recovery time and without side-effects. The combination of techniques to increase the permeation of the photosensitizer is a very recent subject and seems to complement the benefits of day-to-day c-PDT and PDT.
1. Kalka K, Merk H, Mukhtar H. Photodynamic Therapy In Dermatology. J Am Dermatol 2000; 42 (3): 389-413.
2. Allison RR, Mota HC, Sibata CH. Clinical PD/PDT in North America. Photodiagnosis Photodyn Ther. 2004;1(4):263-77.
3. Kurwa HA, Barlow RJ. The role of photodynamic therapy in dermatology. Clin Exp Dermatol.1999; 24(3): 143-8.
4. Morton CA. Photodynamic therapy for nonmelanoma skin cancer— and more?. Arch Dermatol. 2004;140(1):116-20.
5. Issa MCA, Manela-Azulay M. Terapia fotodinâmica: revisão da literatura e documentação iconográfica. An Bras Dermatol. 2010;85(4):501-11.
6. Varma S, Wilson H, Kurwa HA, Gambles B, Charman C, Pearse AD, et.al. Bowen's disease, solar keratoses and superficial basal cell carcinomas treated by photodynamic therapy using a large field incoherent light source. Br J Dermatol. 2001; 144(3): 567–74.
7. Peng Q, Soler AM, Warloe T, Nesland JM, Giercksky KE. Selective distribution of porphyrins in skin thick basal cell carcinoma after topical application of methyl 5-aminolevulinate. J Photoche Photobiol B: Biol. 2001; 62(3): 140–5.
8. Soler AM, Warloe T, Berner A, Giercksky KE. A follow-up study of recurrence and cosmesis in completely responding superficial and nodular basal cell carcinomas treated with methyl-5-aminolevulinate-based photodynamic therapy alone and with prior curettage. Br J Dermatol. 2001; 145(3): 467–71.
9. Raulin C, Greve B, Grema H. IPL technology: A review. Lasers Surg Med. 2003;32(2):78-87.
10. Avram DK, Goldman MP. Effectiveness and safety of ALA-IPL in treating actinic keratoses and photodamage. J Drugs Dermatol. 2004; 3(1 Suppl): S36-39.
11. Nestor MS. Combination therapy in clinical and cosmetic dermatology: the marriage of device and drug. J Drugs Dermatol. 2004; 3(5 Suppl): S4-11
12. Touma DJ, Gilchrest BA. Topical photodynamic therapy: a new tool in cosmetic dermatology. Semin Cutan Med Surg. 2003; 22(2):124-130.
13. Gold MH, Bradshaw VL, Boring MM, Bridges TM, Biron JA. Split-face comparison of photodynamic therapy with 5-aminolevulinic acid and intense pulsed light versus intense pulsed light alone for photodamage. Dermatol Surg. 2006; 32(6):795-801; discussion 801-793.
14. Almeida Issa MC, Piñeiro-Maceira J, Farias RE, Pureza M, Raggio Luiz R, Manela-Azulay M. Immunohistochemical expression of matrix metalloproteinases in photodamaged skin by photodynamic therapy. Br J Dermatol. 2009; 161 (3): 647-53.
15. Issa MCA, Pineiro-Maceira J, Vieira MTC, Olej B, Mandarim-de-Lacerda CA, Luiz RR, et al. Photorejuvenation with Topical Methyl Aminolevulinate and Red Light: A Randomized, Prospective, Clinical, Histopathologic, and Morphometric Study. Dermatol Surg. 2010;36(1):39-48.
16. Braathen LR. Daylight Photodynamic Therapy in Private Practice in Switzerland: Gain Without Pain. Acta Derm Venereol. 2012; 92(6):652-3.
17. Wiegell SR1, Wulf HC, Szeimies RM, Basset-Seguin N, Bissonnette R, Gerritsen MJ, et al. Daylight photodynamic therapy for actinic keratosis: an international consensus: International Society for Photodynamic Therapy in Dermatology. J Eur Acad Dermatol Venereol. 2012; 26(6): 673–9.
18. Morton CA, Wulf HC, Szeimies RM. Practical approach to the use of daylight photodynamic therapy with topical methyl aminolevulinate for actinic keratosis: a European consensus. J Eur Acad Dermatol Venereol. 2015;29(9):1718-23.
19. Rubel DM, Spelman L, Murrell DF, See JA, Hewitt D, Foley P, et al. Daylight PDT with methyl aminolevulinate cream as a convenient, similarly effective, nearly painless alternative to conventional PDT in actinic keratosis treatment: a randomized controlled trial. Br J Dermatol. 2014; 171(5): 1164–71.
20. Lacour J. Results of 2 randomised, controlled, phase III studies with Daylight- PDT in Australia and Europe. Euro-PDT 14th Annual Congress; April 4th–5th, 2014; Nice, France.
21. Wiegell SR, Haedersdal M, Philipsen PA, Eriksen P, Enk CD, Wulf HC. Continuous activation of PpIX by daylight is as effective as and less painful than conventional photodynamic therapy for actinic keratoses – a randomized, controlled study. Br J Dermatol 2008; 158(4): 740–6.
22. Wiegell SR, Haedersdal M, Eriksen P, Wulf HC. Photodynamic therapy of actinic keratoses with 8% and 16% methyl aminolaevulinate and home-based daylight exposure: a double-blinded randomized clinical trial. Br J Dermatol 2009; 160(6):1308–14.
23. Wiegell SR1, Fabricius S, Stender IM, Berne B, Kroon S, Andersen BL, et al. A randomized, multicenter study of directed daylight exposure times of 1½ vs. 2½ h in daylight-mediated photodynamic therapy with methyl aminolaevulinate in patients with multiple thin actinic keratoses of the face and scalp. Br J Dermatol 2011; 164(5):1083–90.
24. Yoo KH, Kim BJ, Kim MN. Enhanced efficacy of photodynamic therapy with methyl 5-aminolevulinic acid in recalcitrant periungual warts after ablative carbon dioxide fractional laser: a pilot study. Dermatol Surg 2009; 35(12):1927-32.
25. Fukui T, Watanabe D, Tamada Y, Matsumoto Y. Photodynamic therapy following carbon dioxide laser enhances efficacy in the treatment of extramammary Paget's disease. Acta Derm Venereol 2009;89(2):150-4.
26. Letada PR, Shumaker PR, Uebrlhoer NS. Demonstration of protoporphiryn IX (PpIX) localized to ares of palmar skin injected with 5 aminolevulinic acid (ALA) and pre-treated with a fractionated CO2 laser prior to topically applied ALA. Photodiagnosis Photodyn Ther. 2010;7(2):120-2.
27. Haedersdal M, Sakamoto FH, Farinelli WA, Doukas AG, Tam J, Anderson RR. Fractional CO2 laser-assisted drug delivery. Laser Surg Med. 2010;42(2):113-22.
28. Shen SC, Lee WR, Fang YP, Hu CH, Fang JY. In vitro percutaneous absorption and in vivo protoporphiryn IX accumulation in skin and tumors after topical 5-aminolevulinic acidapplication with enhancement using an Erbium:YAG laser. J Pharm Sci. 2006; 95(4):929-38.
29. Stumpp OF, Welch AJ, Milner TE, Neev J. Enhacement of transepidermal skin clearing agent delivery using a 980 nm diode laser. Lasers Surg Med. 2005;37(4):278-85.
30. Fang JY, Lee WR, Shen SC, Fang YP, Hu CH. Enhancement of topical 5-aminolevulinic acid delivery by Erbium:YAG laser and microdermoabrasion: a comparison of iontophoresis and electroporation. Br J Dermatol. 2004 ;151(1): 132-40.
31. Wang KF, Fang JY, Hu CH, Lee WR. Erbium:YAG laser pretreatment accelerates the response of Bowen´s disease treated by topical 5-flouracil. Dermatol Surg. 2004; 30(3): 441-5.
32. McAllister DV, Allen MG, Prausnitz MR. Microfabricated microneedles for gene and drug delivery. Annu Rev Biomed Eng. 2000; 2: 289-313.
33. Henry S, McAllister DV, Allen MG, Prausnitz MR. Microfabricated microneedles: a novel approach to transdermal drug delivery. J Pharm Sci. 1998; 87(8): 922-5.
34. Donnelly RF, Morrow DI, McCarron PA, Woolfson AD, Morrissey A, Juzenas P, et al. Microneedle-mediated intradermal delivery of 5-aminolevulinic acid: potential for enhanced topical photodynamic therapy. J Control Release. 2008;129(3):154-62.
35. Mikolajewska P1, Donnelly RF, Garland MJ, Morrow DI, Singh TR, Iani V, et al. Microneedle pre-treatment of human skin improves 5-aminolevulininc acid (ALA)- and 5-aminolevulinic acid methyl ester (MAL)-induced PpIX production for topical photodynamic therapy without increase in pain or erythema. Pharm Res. 2010;27(10):2213-20.
36. Torezan L, Chaves Y, Niwa A, Sanches JA Jr, Festa-Neto C, Szeimies RM. A pilot split-face study comparing conventional methyl aminolevulinate- photodynamic therapy (PDT) with microneedling-assisted PDT on actinically damaged skin. Dermatol Surg. 2013;39(8):1197-201.
37. Curdy C, Kalia YN, Guy RH. Non-invasive assessment of the effects of iontophoresis on human skin in vivo. J Pharm Pharmacol. 2001;53:769-77.
38. Li GL, van der Geest R, Chanet L, van Zanten E, Danhof M, Bouwstra JA. In vitro iontophoresis of R-apomorphine across human stratum corneum. Structure–transport relationship of penetration enhancement. J Control Release. 2002;84(1-2): 49-57.
39. Prausnitz MR. A practical assessment of transdermal drug delivery by skin electroporation. Adv Drug Delivery Rev. 1999;35(1): 61-76.
40. Vanbever R, Preat V. In vivo efficacy and safety of electroporation. Adv Drug Deliv Rev. 1999; 35(1):77-88.
41. Lee S, Kollias N, McAuliffe DJ, Flotte TJ, Doukas AG. Topical drug delivery in humans with a single photomechanical wave. Pharm Res. 1999; 16(11): 1717-21.
42. Lee S, McAuliffe DJ, Kollias N, Flotte TJ, Doukas AG. Permeabilization and recovery of the stratum corneum in vivo: the synergy of photomechanical waves and sodium lauryl sulfate. Lasers Surg Med. 2001;29(2): 145-50.
43. Malvehy, J. A new vision of actinic keratosis beyond visible clinical lesions. J Eur Acad Dermatol Venereol. 2015;29 Suppl 1:3-8.
44. Erlendsson AM, Egekvist H, Lorentzen HF, Philipsen PA., Stausbøl-Grøn B., Stender IM, et al. Actinic keratosis: a cross-sectional study of disease characteristics and treatment patterns in Danish dermatology clinics. International Journal of Dermatology, 55(3): 309–16.
45. Goldman M, Atkin D. ALA/PDT in the treatment of actinic keratosis: spot versus confluent therapy. J Gosmet Laser Ther. 2003;5(2):107–110.
46. Braathen LR, Szeimies RM, Basset-Seguin N, Bissonnette R, Foley P, Pariser D, et al. Guidelines on the use of photodynamic therapy for nonmelanoma skin cancer: An international consensus. J Am Acad Dermatol. 2007;56(1):125–43.
47. Fink-Puches R, Soyer HP, Hofer A, Kerl H, Wolf P. Long-term follow-up and histological changes of superficial nonmelanoma skin cancers treated with topical delta-aminolevulinic acid photodynamic therapy. Arch Dermatol. 1998; 134(7):821-6.
48. Freeman M, Vinciullo C, Francis D, Spelman L, Nguyen R, Fergin P, et al. A comparison of photodynamic therapy using topical methyl aminolevulinate (Metvix) with single cycle cryotherapy in patients with actinic keratosis: a prospective, randomized study. J Dermatolog Treat. 2003 ;14(2):99-106.
49. Dragieva G, Prinz BM, Hafner J, Dummer R, Burg G, Binswanger U, et al. A randomized controlled clinical trial of topical photodynamic therapy with methyl aminolaevulinate in the treatment of actinic keratoses in transplant recipients. Br J Dermatol. 2004;151(1):196-200.
50. Szeimies RM. Methyl aminolevulinate-photodynamic therapy for basal cell carcinoma. Dermatol Clin. 2007; 25(1):89-94.
51. Lehmann P. Methyl aminolaevulinate-photodynamic therapy: a review of clinical trials in the treatment of actinic keratoses and nonmelanoma skin cancer. Br J Dermatol. 2007; 156(5):793-801.
52. Cesarini JP, Michel L, Maurette JM, Adhoute H, Bejot M. Immediate effects of UV radiation on the skin: modification by an antioxidant complex containing carotenoids. Photodermatol Photoimmunol Photomed. 2003;19(4):182-9.
53. Ruiz-Rodriguez R, Sanz-Sanchez T, Cordoba S. Photodynamic photorejuvenation. Dermatol Surg. 2002; 28(8):742-744; discussion 744.
54. Alster TS, Tanzi EL, Welsh EC. Photorejuvenation of facial skin with topical 20% 5-aminolevulinic acid and intense pulsed light treatment: a split-face comparison study. J Drugs Dermatol. 2005; 4(1):35-38.
55. Szeimies RM, Torezan L, Niwa A, Valente N, Unger P, Kohl E, et al. Clinical, histopathological and immunohistochemical assessment of human skin field cancerization before and after photodynamic therapy. Br J Dermatol. 2012;167(1):150-9.
56. Lavon I, Kost J. Ultrasound and transdermal drug delivery. Drug Discov Today 2004;9(15):670-6.
57. Tachibana K, Tachibana S. Transdermal delivery of insulin by ultrasonic vibration. J Pharm Pharmacol 1991;43(4):270-1.
58. Sintov AC, Krymberk I, Daniel D, Hannan T, Sohn Z, Levin G. Radiofrequency-driven skin microchanneling as a new way for elletrically assisted transdermal delivery of hydrophilic drugs. J Control Release 2003; 89 (2):311-20.
59. Issa MCA, Kassuga LEBP, Chevrand NS, Pires, MTF. Topical delivery of triamcinolone via skin pretreated with ablative radiofrequency: a new method in hypertrophic scar treatment. Int J Dermatol. 2012. 52(3): 367-70.
60. Issa MC, Pires M, Silveira P, Xavier de Brito E, Sasajima C. Transepidermal drug delivery: a new treatment option for areata alopecia? J Cosmet Laser Ther. 2015;17(1):37-40.
61. Kassuga LEBP, Issa MCA, Chevrand NS. Aplicação transepidérmica de medicamento associado a terapia fotodinâmica no tratamento de ceratoses actínicas. Surg Cosmet Dermatol. 2012; 4 (1): 89-92.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}