


Ticiana de Andrade Castelo Branco Diniz1; Maria Isabel Ramos Saraiva2; Marcella Amaral Horta Barbosa3; Larissa Karine Leite Portocarrero4; Priscila Kakizaki5; Neusa Yuriko Sakai Valente6
Dermatofibrosarcoma protuberans is an uncommon and relapsing fibrohistiocytic tumor of intermediate malignancy. Its rarest variant is known as atrophic, morphea type or dermatofibrosarcoma non protuberans and its clinical diagnose is difficult. There are not well established dermatoscopic criteria, so the diagnosis is histopathologic. There are advances in immunohistochemical and genetic that help the diagnosis and complete surgical excision. It is reported a case of atrophic dermatofibrosarcoma in a 27 years patient ant it is reviewed the clinical, dermoscopic, histological and genetic aspects.
Keywords: DERMOSCOPY; NEOPLASMS; DERMATOFIBROSARCOMA
Dermatofibrosarcoma protuberans (DFSP) is a relatively uncommon fibro-histiocytic tumor of intermediate malignancy. It is often locally aggressive, with high-risk of recurrence and low risk of metastasis. 1 The initial clinical appearance is that of a hardened, violet or reddish-brown, keloid-like plaque. 2 Being asymptomatic and slow growing, there may be a delay in diagnosis. When the lesion is already established, the diagnosis is facilitated by its specific appearance. The initial lesion is rarely atrophic or depressed; however when this is the case it is called atrophic dermatofibrosarcoma (ADFSP) and diagnosis is difficult. 3,4
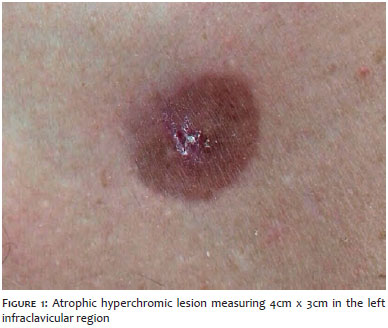
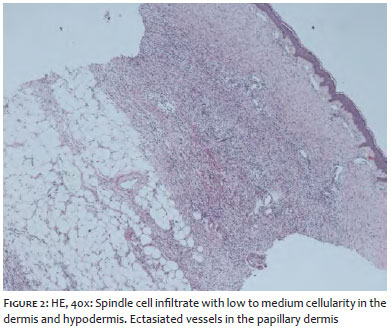
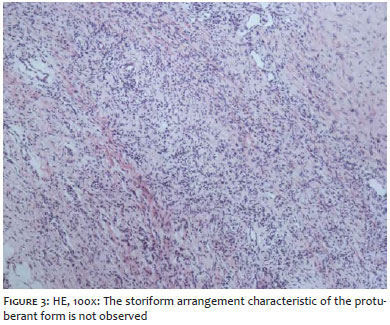
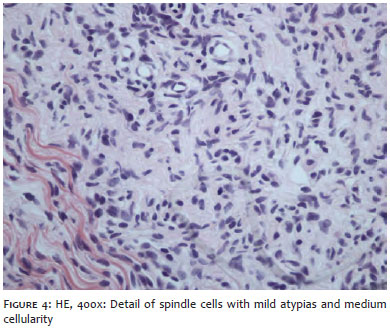
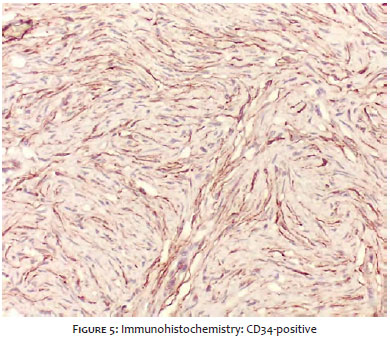
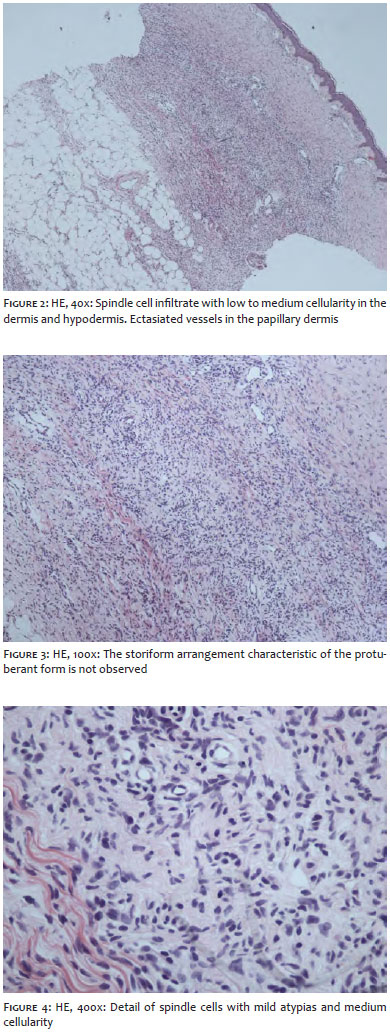
A 27 year-old male patient had been bearing a lesion in the left infraclavicular region for 10 years. The examination revealed an atrophic hyperchromic lesion measuring 4x3cm (Figure 1). An incisional biopsy allowed to observe the presence of neoplastic infiltration in the superficial / deep dermis and hypodermis, with proliferation of fusiform cells with a mild degree of nuclear polymorphism and hyperchromasia forming multidirectional bundles, sometimes parallel to the epidermis, which had atrophy of the stratum spinosum (Figures 2,3 and 4). The immunohistochemistry's results were positive for CD34 and negative for XIIIa factor (Figure 5). The histological diagnosis was of dermatofibrosarcoma, however the final diagnosis after clinical correlation was that of ADFSP. The surgical excision of the lesion was performed with 5cm margins.
Sarcomas are soft tissue malignant tumors and contribute for the small percentage of cutaneous neoplasms. Dermatofibrosarcoma protuberans is most frequent cutaneous sarcoma, accounting for 1% of the conjunctive tissue sarcomas and any less than 0.1% of all malignant neoplasms 5 It is a slow growing tumor, usually asymptomatic, which might lead to late diagnosis. 2 The most common clinical development is a hardened, purplish or reddish-brown plaque, which develops into a nodule, 5 however possibly arising as an atrophic lesion. Initially described in 1985, this condition's rarest variant is known as ADFSP, a morphea-type variant of DFSP, or dermatofibrosarcoma non-protuberans. 3.4 It was once suggested that the term protuberans should be suppressed in favor of the designation atrophic dermatofibrosarcoma, since not all lesions have nodular aspect, 4 nevertheless, consensus has not been reached yet. The ADFSP has a difficult clinical diagnosis, as it may be misdiagnosed with morphea, idiopathic atrophodermia, atrophic scar, anetoderma or lipoatrophy. 6
There are still no well-established dermoscopic criteria. Different patterns have been described in the literature. It can display branching vessels over a yellow background without pigmentary network, which might be due to skin atrophy,7 or, even brown regular reticular lines corresponding to melanin accumulation in basal keratinocytes over a purplish erythematous background, resulting from dilated vessels in the dermal plexus.2 Specific findings or differentiation factors have not yet been found that would allow distinguishing ADFSP from other diagnoses. 2
In a less intense way when compared to the protruding form, cells arranged in a storiform pattern over a fibrous stroma background characterize the ADFSP's anatomopathological examination. The infiltrate tends to extend up until the subcutaneous fat. In general, there is little nuclear pleomorphism. The epidermis is usually spared, and the dermis' thickness is reduced by roughly 50% (Figures 2 to 4). 1
The use of immunohistochemistry can assist in the identification of the tumor, as well as in its delimitation for complete excision using Mohs micrographic surgery (MMS). The ADFSP is routinely CD34-positive and factor XIIIa-negative. Since the neoplasm can invade deeply along collagen bundles or connective tissue septa, the extent of the invasion might not be clinically apparent. This explains recurrence rates of 11% to 53% when 1cm to 3cm surgical margins are used (11% for 3cm margins in DFSP cases). 8,9 There is scant data available for the atrophic form. Mohs micrographic surgery using immunohistochemical staining with CD34 in frozen sections might allow the detection of the most asymmetrical tumors. 8.9
Over the past decade, advances have shown that the mutation responsible for the ADFSP is a reciprocal translocation t(17; 22) (q22; q13.1) or, more often, the creation of a supernumerary ring chromosome derived from t(17; 22). These mutations cause the chromosome 17's type 1-alpha-1 collagen (COL1A1) to merger with chromosome 22's gene chain platelet-derived growth factor (PDGFB), forming a chimeric protein, COL1A1-PDGFB. 4
After translocation, COL1A1 and its promoters replace the regulating elements that inhibit the PDGFB, allowing the production of high levels of COL1A1-PDGFB's messenger RNA. The cleavage of PDGFB by the COL1A1- PDGFB protein can lead to malignant transformation.4 In the gene translocation process, variable lengths of COL1A1 are juxtaposed to the same PDGFB gene sequence. After the cleavage of COL1A1-PDGFB, fragments of COL1A1 become trimers associated to type 1-alpha-2 collagen (COL1A2), which is secreted in the extracellular medium. 4 It is proposed that the variety of COL1A1 and COL1A2 trimers may be responsible for different stroma present in a typical DFSP and its atrophic variant, given that each tumor can have a specific length of the COL1A1 fragment. Inhibition of the PDGFB receptor might explain the atrophic phenotype 4
The treatment is similar to that used in the non-atrophic form. Mohs micrographic surgery is the first choice. The second choice is surgical excision with a margin of 3cm to 5cm, with chance of recurrence due to the possibility of invasion beyond the fascia and muscles.10 Although recurrences often arise within the 3 first years after the surgery, they can take place several years after, justifying watchfulness in the long term. 1
1. Lee SJ, Mahoney MC, Shaughnessy E. Dermatofibrosarcoma protuberans of the breast: imaging features and review of the literature. AJR Am J Roentgenol. 2009;193(1):W64¬-69.
2. Akay BN, Unlu E, Erdem C, Heper AO. Dermatoscopic findings of atrophic dermatofibrosarcoma protuberans. Dermatol Pract Concept. 2015;5(1):71-¬3.
3. Lambert WC, Abramovits W, Gonzalez¬-Sevra A, Souchon E, Schwartz RA, Little WP Jr. Dermatofibrosarcoma non¬protuberans: description and report of five cases of a morpheaform variant of dermatofibrosarcoma. J Surg Oncol. 1985;28(1):7-¬11.
4. Young CR 3rd, Albertini MJ. Atrophic dermatofibrosarcoma protuberans: case report, review, and proposed molecular mechanisms. J Am Acad Dermatol. 2003;49(4): 761-¬764.
5. Fleury LFF Jr, Sanches JA Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81(3):207¬-21.
6. Bakry O, Attia A. Atrophic dermatofibrosarcoma protuberans. J Dermatol Case Rep. 2012;6(1):14-¬7.
7. Gungor S, Buyukbabani N, Buyuk M et al. Atrophic dermatofibrosarcoma protuberans: are there specific dermatoscopic features? J Dtsch Dermatol Ges. 2014;12(5):425-¬7.
8. Gloster HM Jr. Dermatofibrosarcoma protuberans. J Am Acad Dermatol.1996;35 (3 Pt 1):355¬-74.
9. Ratner D, Thomas CO, Johnson TM, Sondak VK, Hamilton TA, Nelson BR, et al. Mohs micrographic surgery for the treatment of dermatofibrosarcoma protuberans. Results of a multiinstitutional series with an analysis of the extent of microscopic spread. J Am Acad Dermatol. 1997;37(4):600-¬13.
10. Haycox CL, Odland PB, Olbricht SM, Casey B. Dermatofibrosarcoma protuberans (DFSP): growth characteristics based on tumor modeling and a review of cases treated with Mohs micrographic surgery. Ann Plast Surg. 1997;38(3):246-¬51.
This study was performed at the Hospital Servidor Público Estadual (HSPE-SP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}